
Abstract
Abstract
Objective and Background:
Survival predictions by subjective evaluations are important for end-stage patients. However, subjective evaluations based on experience are difficult. Therefore, we investigated whether the Glasgow prognostic score (GPS), prognostic nutritional index (PNI), and C-reactive protein (CRP)/albumin ratio (CRP/Alb ratio) calculated from the laboratory values of objective evaluations are useful for predicting survival times in end-stage patients.
Methods:
We retrospectively investigated the age, sex, death cause, CRP levels, Alb levels, and lymphocyte counts in 363 cancer and noncancer patients who died in the 12-month period between April 2015 and March 2016. A multivariate analysis was performed to calculate GPS, PNI, and the CRP/Alb ratio from laboratory values and adjusted for confounding factors.
Results:
PNI and CRP/Alb ratio exhibited negative and positive correlations with survival days, respectively. All GPS, PNI, and CRP/Alb ratio were useful to predict two to four remaining weeks. Interestingly, CRP/Alb ratio, but not GPS or PNI, was higher in patients with predicted short-term survival of zero to two weeks than in that of two to four weeks (odds ratio 2.32; 95% confidence interval 1.61–3.34).
Discussion:
These results suggest that the CRP/Alb ratio is an independent factor that is beneficial to predict short-term survival of within two weeks.
Introduction
P
The prognostic nutritional index (PNI), 3 C-reactive protein/albumin (CRP/Alb) ratio, 4 and Glasgow prognostic score (GPS) 5 are calculated from laboratory values, which are objective evaluations and factors used to predict outcomes after solid cancer surgery. However, it currently remains unclear as to whether PNI, the CRP/Alb ratio, and GPS are useful for predicting the short-term survival of terminal patients.6,7 Further, it has not yet been established as to whether these prognostic factors are effective for hematological malignancies or noncancer patients. Therefore, we herein investigated whether PNI, the CRP/Alb ratio, and GPS calculated from the laboratory values of objective evaluations are useful for predicting short survival times in cancer and noncancer patients.
Patients and Methods
This study investigated the age, gender, and cause of death of 363 patients who died in the 12-month period between April 2015 and March 2016 at the Seichokai Fuchu Hospital. Blood tests, including those to measure CRP levels, Alb levels, and lymphocyte counts, were conducted 6054 times between April 2015 and March 2016. We used 363 patients corresponding to 5718, 5771, and 5553 laboratory data points on Alb, CRP, and the CRP/Alb ratio, respectively, and 355 patients corresponding to 4714 laboratory data points on PNI. Laboratory data were classified and compared for each predicted survival period: 0–2 weeks before death (0–0.5 months), 2–4 weeks (0.5–1 month), 4–12 weeks (1–3 months), and 12–52 weeks (3–12 months). We also used average values for multiple inspection data within the same period.
PNI was calculated according to the following formula as previously described: 10 × serum Alb value (g/dL) +0.005 × peripheral lymphocyte count (/μL). 3 GPS was constructed as previously described.5,8 Briefly, patients with an elevated CRP level (>1.0 mg/dL) and hypoalbuminemia (<3.5 g/dL) were allocated a score of 2. Patients in whom only one of these biochemical abnormalities was present were allocated a score of 1. Patients in whom neither of these abnormalities was present were allocated a score of 0. The CRP/Alb ratio was calculated from CRP and Alb values. This research was approved by the Ethics Committee of Seichokai Fuchu Hospital.
Statistical analysis
Spearman's rank correlation coefficient was used to study correlations of continuous variables that do not show a normal distribution. The Kruskal-Wallis test and Steel-Dwass method were used to compare three or more continuous variables not showing normality. Using the receiver operating characteristic (ROC) curve and variable of the predicted survival period, we selected optimal cut-off values for Alb, CRP, the CRP/Alb ratio, and PNI that provided the closest point to the left upper hand corner of the graph, and we then divided our patients into two groups. In the univariate analysis, comparisons of categorical variables were performed by using logistic regression. A multivariate logistic regression analysis was performed on factors considered to be important in the univariate analysis. We included variables with a p-value <0.05 in the univariate analysis in the subsequent multivariate analyses. In addition, we included the cause of death in the variables of the multivariate analysis. Collinearity was examined with the variance inflation factor (VIF). The variable we used for multivariate analysis was VIF <5. The results obtained were described as odds ratios (OR) and 95% confidence intervals (CI). A p value <0.05 was defined as being significant. All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), 9 which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).
Results
The characteristics of 363 patients who died during the study period are shown in Table 1. The causes of death among the patients analyzed were as follows: solid cancer 28.4%, blood cancer 11%, and noncancer 60.6%.
SD, standard deviation.
Correlations were observed between predicted survival periods and Alb, PNI, CRP, and the CRP/Alb ratio (Fig. 1).
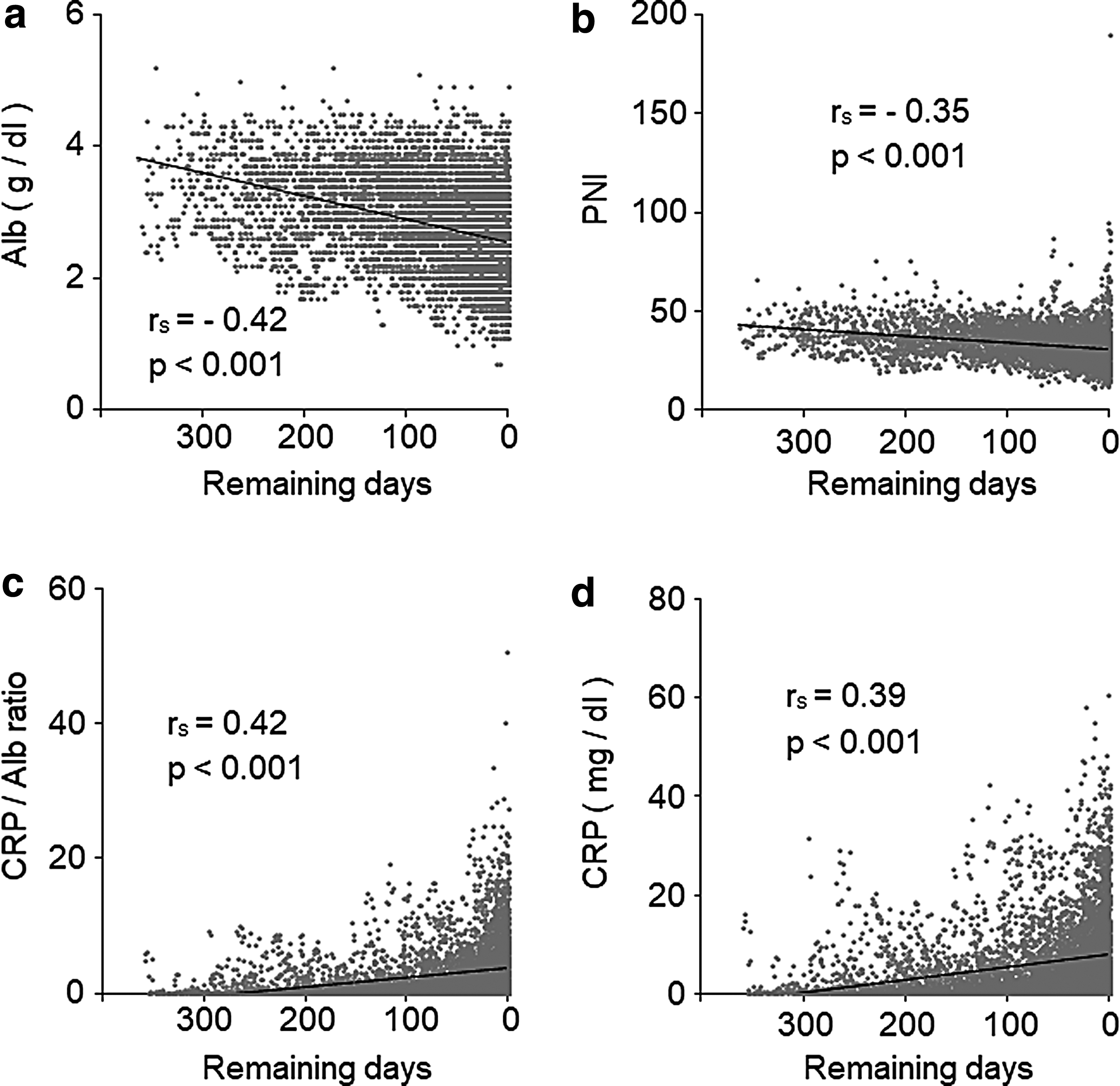
Correlations between predicted survival periods and Alb
Figure 2 shows the results of comparisons of laboratory values, PNI, and the CRP/Alb ratio for each predicted survival period. A significant difference was observed in CRP and the CRP/Alb ratio between the predicted short-term survival period of 0.5–1 and 0–0.5 months. There was a significant difference between Alb, PNI, the CRP/Alb ratio, and CRP between the predicted survival periods of 0.5–1, 1–3, and 3–12 months.
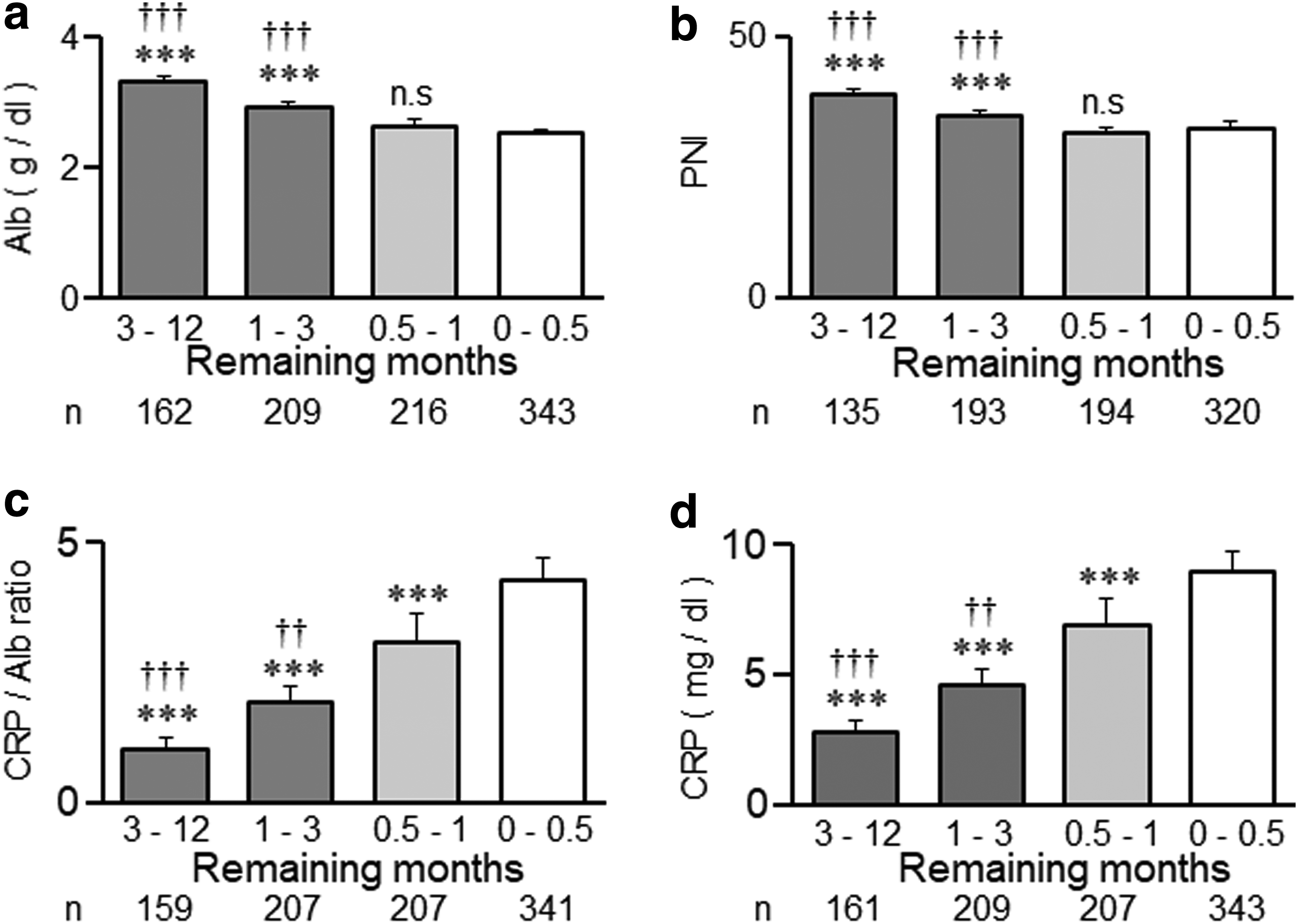
Comparison of blood test values Alb
A univariate analysis was performed by dividing patients into two groups with predicted short-term survival periods of 0–0.5 and 0.5–1 months to verify factors useful for identifying patients with a predicted short-term survival of within 1 month that was actually expected to be within 0.5 months (Table 2). The optimal cut-off values for continuous variables were as follows from the ROC analysis: age: 73, Alb: 2.5, CRP: 6.5, the CRP/Alb ratio: 2.9, and PNI: 31. GPS was previously reported to have a cut-off value of 2. 6 The areas under ROC curves were as follows: age: 0.554, Alb: 0.558, CRP: 0.596, the CRP/Alb ratio: 0.601, PNI: 0.528, and GPS: 0.523. The univariate analysis revealed significant differences in age, CRP, the CRP/Alb ratio, and the cause of death. A multivariate logistic regression analysis was performed to control confounding factors. CRP was not selected because of strong collinearity. The results of the multivariate logistic regression analysis showed that a higher CRP/Alb ratio correlated with short-term survival of two weeks (adjusted OR: 2.32, 95% CI: 1.61–3.34, p < 0.001). A univariate analysis was then performed by dividing patients into two groups with short-term survival periods of 0.5–1 and 1–3 months to verify factors useful for identifying patients with short-term survival of within 3 months that was actually expected to be within 1 month (Table 3). The optimal cut-off values for continuous variables from the ROC analysis were as follows: age: 73, Alb: 2.6, CRP: 4.1, the CRP/Alb ratio: 1.6, and PNI: 32. GPS was previously reported to have a cut-off value of 2. 6 The areas under the ROC curves were as follows: age: 0.495, Alb: 0.628, CRP: 0.588, the CRP/Alb ratio: 0.595, PNI: 0.619, and GPS: 0.588. The univariate analysis revealed significant differences in Alb, CRP, the CRP/Alb ratio, PNI, and GPS. A multivariate logistic regression analysis was performed to control for confounding factors. CRP was not selected because of strong collinearity. The results of the multivariate logistic regression analysis showed that lower Alb levels correlated with short-term survival of one month (adjusted OR: 0.53, 95% CI: 0.29–0.98, p = 0.044).
Alb, albumin, CI, confidence interval; CRP, C-reactive protein; GPS, Glasgow prognostic score; PNI, prognostic nutritional index; OR, odds ratio.
Discussion
The results of this study indicate that the CRP/Alb ratio is useful for predicting the short-term survival of patients with solid cancer, hematological malignancies, and noncancer of within two weeks. However, it was not useful for predicting longer outcomes. Therefore, the CRP/Alb ratio may be suitable to predict survival times within two weeks in both cancer and noncancer patients.
Previous models to predict survival times were developed by using variables from a single time point (e.g., discharge or surgery date).10–13 In contrast, this study was based on robust data, utilizing laboratory variables monitored within one year before death events. A few recent studies have identified some candidate biomarkers that may be indicative of a common biological process to dying in cancer patients,14,15 whereas little such information is available for noncancer patients. The CRP/Alb ratio, PNI, and GPS are used as prognostic tools for estimating survival time in patients with gastric cancer,16–18 pancreatic cancer,19,20 colon cancer,21–24 liver cancer,25,26 lung cancer,6,27,28 and esophageal cancer.4,29–30 The present data from both cancer and noncancer patients were, in general, consistent with the previous studies on solid cancer patients. Although the CRP/Alb ratio is used as a tool to predict outcomes, as described earlier, few studies have evaluated short-term survival. Alb is also important for predicting outcomes.31–34
PNI,35,36 GPS, 37 and CRP 38 are used to predict the outcomes of patients with hematological malignancies. PNI, Alb, and CRP were previously demonstrated to be effective as a tool to predict the outcomes of noncancer patients (e.g., heart failure).10,39 A neutrophil/lymphocyte ratio, known to be useful for predicting the outcome of cancer patients, was not measured in this study. However, it is noteworthy that the neutrophil/lymphocyte ratio is well correlated with the CRP/Alb ratio. 40 PNI, 18 GPS 5 , and CRP/Alb ratio 4 have been reported to be useful for predicting survival time in a month-year range. Our study suggests that the CRP/Alb ratio, but not PNI or GPS, is also applicable for predicting relatively short-term (within two weeks) survival.
Accurate predictions facilitate the provision of optimal treatments to patients. The prediction of outcomes according to objective criteria is very useful in clinical practice, to avoid the administration of unnecessary parenteral hydration, since subjective outcome prediction requires skilled staff and may not be reliable. 41 Actually, parenteral hydration is not recommended for end-stage cancer patients with predicted short-term survival of less than two weeks.42–44 It is often emphasized that parenteral hydration for patients with predicted short-term survival is really disadvantageous. Potential limitations need to be considered when interpreting the results of this study. This was an observational study with a retrospective design and was performed at a single general hospital. Therefore, the available sample size in our study was small, resulting in a low predicted value and the potential necessity to combine these data.
In summary, this study suggests that the CRP/Alb ratio of objective data is effective for predicting short-term survival. The results obtained will contribute to improving treatments for end-of-life patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.