
Abstract
Abstract
Background:
Physical activity in palliative care patients is closely linked to independence, function, carer burden, prognosis, and quality of life. Changes in physical activity can also be related to service provision needs, including requirements for support and prognosis. However, the objective measurement of physical activity is challenging, with options, including self-report, invasive and intensive measures such as calorimetry, or newer options such as pedometers and accelerometers. This latter option is also becoming more viable with the advent of consumer technology driven by the health and exercise industry.
Objective:
In this article, we highlight our experiences of activity monitoring in palliative care patients as part of telehealth trial. We also highlight the strengths and limitations of activity monitoring in the palliative care population and potential applications.
Conclusions:
Although the advent of consumer technology for activity measurement makes their use seem attractive in clinical settings for palliative care patients, there are a number of issues that must be considered, in particular the reason for the activity monitoring and associated limitations in the technology.
Maintaining physical activity is a priority for palliative care patients given its association with independence and function, carer burden, prognosis, and quality of life. 1 Accordingly, the ability to objectively measure activity in palliative care patients provides opportunities to understand functional changes over time, identify service provision needs, including support for caregivers, and predict functional trajectories and prognosis.
Palliative care patients experience a downward functional trajectory that impacts both the patient and carer's ability to manage at home. Enabling activity and maintaining or improving strength and function have many possible benefits for palliative care patients, including promoting independence, well-being, reducing fatigue, and reducing caregiver burden. 2 An Australian study showed that timely coordination of care was associated with maintenance of functional status in the months leading to death. 3
Previous methods of measuring activity, such as self-report, direct observation, or activity monitors, have been limited by issues such as accuracy, invasiveness, and cost. Recent technological advances have led to increased consumer accessibility to and the utilization of activity monitoring in everyday activities. Activity monitoring for palliative care patients can serve a number of purposes:
as a longitudinal measure of habitual physical activity, potentially identifying triggers or thresholds for intervention or additional supports; as an outcome measure to assess the effect of interventions on activity or function; or as a motivational tool to promote physical activity where appropriate.
In 2013–2014, we performed a pilot study examining the use of telehealth to 43 community palliative care patients.4,5 Southern Adelaide Palliative Service is a specialist palliative care service with a nursing-led community care coordination service supported by a medical and allied health team. The community service is divided into four geographical regions, and one region had the telehealth intervention. This intervention was iPad based, allowing
videoconferencing between patients, carers, and clinical staff;
patient-reported outcomes, including regular symptom reporting (Symptom Assessment Scale), function (Australia-modified Karnofsky Performance Scale), and quality of life (Australian Quality of Life), with predefined thresholds for alert generation for the care coordinator; and
remote activity monitoring, using the FitBit Zip™.
The activity monitoring was for exploratory purposes only (feasibility and acceptability), and was not used as an outcome measure. Patients were each given a FitBit Zip and shown how to access activity counts at anytime on their FitBit Zip or iPad as part of their training for the intervention. They were encouraged to wear the device all wake hours. There was no formal follow-up of compliance.
Overall, the use of the activity monitor was low. Although all patients were offered a FitBit Zip, only a small proportion of patients used the FitBit regularly, and the majority had low compliance that further dropped over time. Most patients acknowledged that they frequently forgot to put the FitBit Zip on. Poor compliance was further exacerbated by inability to attach the FitBit Zip to clothing due to reduced manipulative skills, flat batteries, and loss of the device. A convenience sample of the readings over time for seven patients are shown in Figure 1, highlighting the difficulties in assessing activity levels due to high inter- and intraindividual variation, and distinguishing between low activity and compliance.
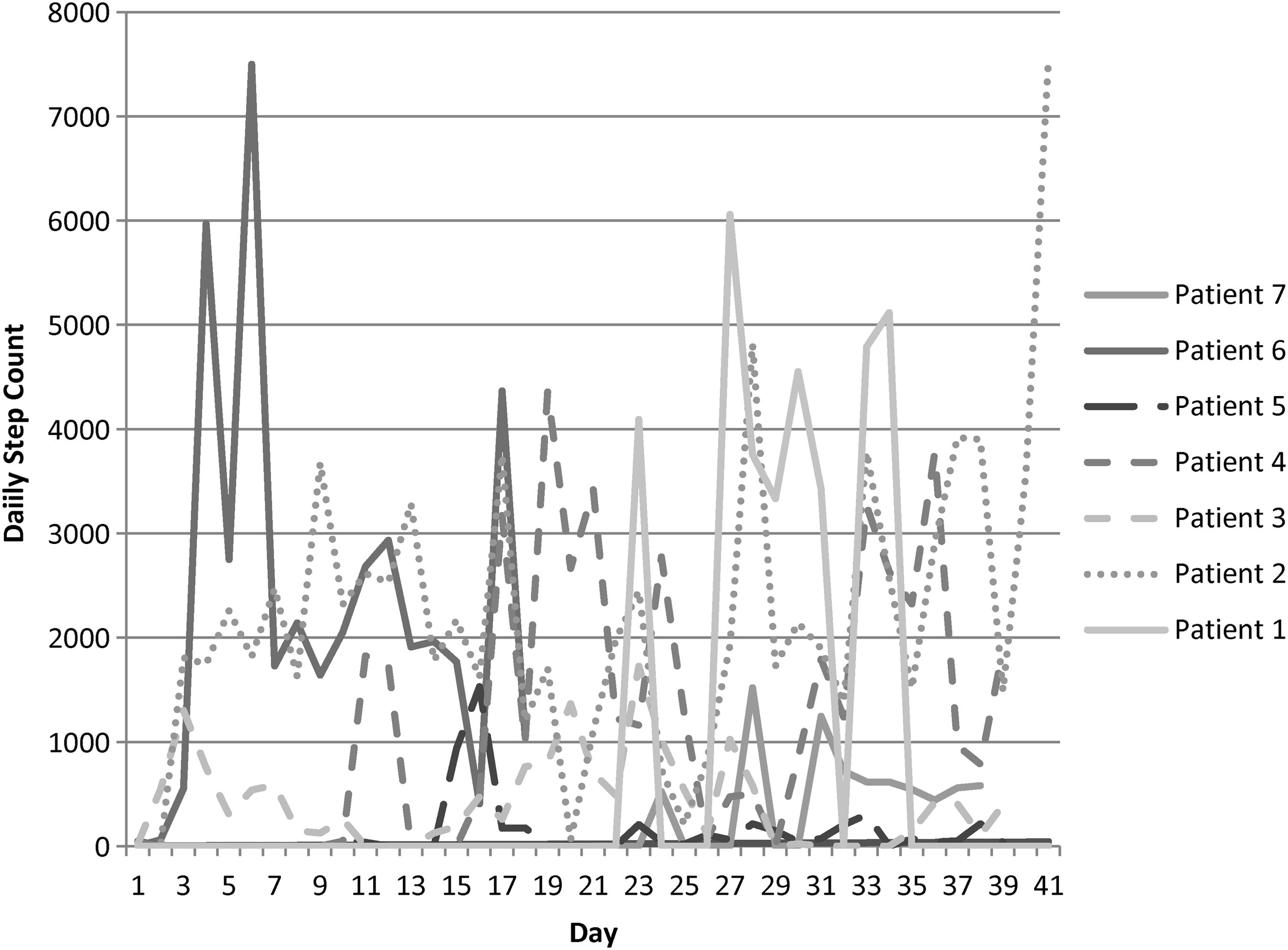
Activity counts of seven palliative care patients.
Furthermore, for palliative care patients the level and intensity of activity may be low. Low intensity activity may not be well captured on activity monitors, and thus under-represent the true activity levels. 6 A number of participants in our study found that the FitBit Zip did not record steps when ambulating slowly. However, research-grade accelerometers such as activPAL™ have been found to be more sensitive at detecting steps taken at different intensities and not to accrue additional steps during car travel. 7
For services considering using activity monitoring as part of their clinical service or for research in a palliative care population, there are a number of key considerations related to each of the three potential purposes as listed earlier.
Activity Monitoring for Longitudinal Monitoring of Habitual Physical Activity
The longitudinal monitoring of activity can provide important information about activity, function, and, indirectly, care needs. Services need to plan how they will respond to the activity data feed, such as considering thresholds and triggers for clinical or social care responses. Furthermore, compliance with wearing activity monitors, particularly over time can wane. This then requires the distinction for those performing the activity monitoring between low compliance with wearing the monitor, or low activity. This may well be exacerbated in palliative care patients, with changing health states, and dynamic and competing priorities. Our study demonstrated the difficulty in obtaining reliable activity measures in all patients because of the issues identified earlier, and accordingly the challenges on using such monitoring for palliative care patients.
Activity Monitoring for Measuring the Effect of an Intervention
The measurement of the effect of an intervention on activity is one of the most likely uses of activity monitoring. Given the issues with long-term compliance with activity monitors as discussed previously, one potential solution is that activity monitoring should be episodic and time-limited to capture changes in activity levels over time. Depending on the nature of the patient group, the intervention, and expected outcome, the frequency of monitoring should be chosen. The monitoring should be for short and focused periods to maximize compliance and minimize burden. In a study examining physical activity in patients with colorectal cancer, three to four days of monitoring was thought to be sufficient. 8 In addition, for this purpose, all patients should be blinded to activity counts given the risk of promoting physical activity. Consideration is also required for how the raw data will be obtained for analysis as not all commercially available activity monitors allow download of the raw data without further licensing.
Activity Monitoring for the Promotion of Physical Activity
An activity monitor can be used as a tool to promote physical activity, although the evidence of effect is limited.
9
It is postulated that a number of mechanisms may be part of the change in behavior related to activity monitors
9
:
self-monitoring, for example, access to step counts or targeted message through the day; goal setting, for example, setting a target of 6000 steps per day; rewards, for example, congratulatory messages for achieving milestones; social support from others, for example, groups encouraging each other to achieve goals or competition; and coaching from peers or professionals, for example, to motivate increases in physical activity.
Such a purpose requires the patient to receive feedback on their activity, such as through apps associated with the activity monitor that report activity.
Therefore, although the advent of commercially available activity monitors offers much potential for remote monitoring of palliative care patients, a number of issues must be considered in how and why they are to be used to make them effective. Strategies to address these issues depend on the nature of the monitoring required and the reasons for monitoring. For palliative care services, activity monitoring may allow for earlier recognition of change in functional status leading to increasing caregiver needs and support. This may reduce crises and allow better triaging of community health and social community supports.
Footnotes
Author Disclosure Statement
No competing financial interests exist.