
Abstract
Abstract
Background:
There is no established method to objectively predict short-term prognosis. Recently, we proposed objective, short-term, prognostic predictive methods that are combinations of laboratory test items: WPCBAL score, derived from six values (white blood cell, platelet, C-reactive protein, blood urea nitrogen, aspartate aminotransferase, and lactate dehydrogenase). However, that study was conducted in an acute-phase hospital to identify the test items useful for prognostic prediction; thus, whether WPCBAL score could be applied to terminal cancer patients in a palliative care unit was unverified.
Objective:
To verify the usefulness of WPCBAL score for terminal cancer patients.
Design:
A retrospective study.
Setting/Subjects:
Patients admitted to the palliative care unit of Ashiya Municipal Hospital (N = 128) in Japan in 2016.
Measurements:
The sensitivity, specificity, positive predictive value, negative predictive value, accuracy, and area under the receiver operating characteristic curve (AUROC) were compared between WPCBAL score and the Glasgow prognostic score (GPS).
Results:
For predicting three-week prognosis, WPCBAL score showed higher AUROC compared with GPS (0.7540 and 0.6573, respectively). WPCBAL score predicting two-week prognosis showed greater AUROC than GPS predicting three-week prognosis (0.7491 and 0.6573, respectively).
Conclusion:
WPCBAL score was verified to objectively predict the two- or three-week prognosis for terminal cancer patients in a palliative care unit. WPCBAL score may be a new option for prognostic prediction for terminal cancer patients.
Introduction
Short-term prognostic prediction is very important for both patients and medical staff in palliative care. For patients, two- to three-week prognosis is the last chance for them to make final decisions. For physicians, short-term prognostic prediction is useful to determine appropriate medical interventions. For example, if depressed patients are unlikely to survive for several weeks, antidepressants would rarely be prescribed because they take at least two weeks to bring about improvement and could cause unpleasant anticholinergic side effects. Similarly, although midazolam is frequently used as a sedative for symptom relief in palliative care settings, tolerance can develop if it is administered for two weeks or longer. 1 Currently, there are several short-term, prognostic predictive methods, but most require subjective medical staff judgment, so predictions depend on staff experience.2,3 Therefore, a method that can objectively predict prognosis is required. Hui et al. 4 reported that prognostic prediction without subjective medical staff judgment showed high accuracy within 30 days of death. As a prognostic predictive method comprising only objective indicators, Miura et al. 5 reported that the Glasgow prognostic score (GPS) 6 can predict three-week prognosis with higher sensitivity than the Palliative Prognostic Index (PPI). 7 Chen et al. 8 reported that the Objective Palliative Prognostic Score could predict death within a week. However, evidence on these findings is insufficient; moreover, no method exists for objectively predicting two-week prognosis. We have previously reported a combination of six routinely measured items (white blood cell [WBC], platelet [PLT], C-reactive protein [CRP], blood urea nitrogen [BUN], aspartate aminotransferase [AST], and lactate dehydrogenase [LDH]) that predicted two-week prognosis with high accuracy, 9 termed “WPCBAL” (WBC, PLT, CRP, BUN, AST, and LDH) score. Blood tests are essential to obtain laboratory test values; however, it is difficult to conduct blood sampling at home or in palliative care units.10,11 In our previous report, 9 in an acute-phase hospital where blood tests are routine, we aimed to identify test items useful for prognostic prediction. However, it was unclear if the WPCBAL score was applicable to terminal cancer patients in a palliative care unit. Therefore, in this study, we aimed to verify its usefulness in a palliative care unit for terminal cancer patients.
Materials and Methods
Patients
Patients admitted to the palliative care unit of Ashiya Municipal Hospital in Japan from January to December 2016 were retrospectively analyzed. These patients met the following criteria: difficulties in alleviating various symptoms caused by cancer in outpatient care, admission requests from patients, and an agreement to the implementation of anticancer drug therapy. For patients with multiple admissions, only the first was selected for the study. Initially, 178 patients were enrolled, and 148 were selected after we recorded all examination results of WPCBAL score and GPS (a combination of CRP and albumin [Alb]). Twenty patients were excluded because of missing data within three days before and after admission. Finally, 128 patients were enrolled.
Data collection
Age, sex, body mass index, Eastern Cooperative Oncology Group Performance Status (ECOG PS), cancer primary site, chemo- and radiotherapy history, WBC and PLT counts, and BUN, AST, LDH, CRP, and Alb values were recorded at admission. Test results within three days before and after admission were extracted. Furthermore, the duration between admission and death was investigated.
Percentage of deaths according to WPCBAL score and GPS
WPCBAL score and GPS criteria are presented in Table 1. One point is given when the laboratory test values of the items constituting each method satisfy the criteria presented in Table 1. Therefore, WPCBAL score and GPS had maximum scores of 6 and 2 points, respectively. For the WPCBAL score, the percentage of patient deaths within two and three weeks of admission was calculated for each total score. For GPS, similar calculations were performed for deaths within three weeks after admission.
Reference Values of Predictors for WPCBAL Score and Glasgow Prognostic Score
Alb, serum albumin; AST, aspartate aminotransferase; BUN, blood urea nitrogen; CRP, C-reactive protein; GPS, Glasgow prognostic score; LDH, lactate dehydrogenase; PLT, platelet; WBC, white blood cell.
Predictive performance
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy for predicting two- or three-week prognosis were calculated for WPCBAL score, and the same factors were calculated for three-week prognosis using GPS.
Area under the receiver operating characteristic curve and statistical analysis
Cutoff values predicting prognosis and area under the receiver operating characteristic curve (AUROC) were determined by plotting a receiver operating characteristic curve (ROC) for WPCBAL score. Survival or death within two or three weeks after admission was defined as dependent variables; WPCBAL score was the independent variable. The Kaplan–Meier method and log-rank test were performed by classifying the total points of WPCBAL score as low (≤2), middle (3 or 4), or high points (≥5). Based on obtained WPCBAL score cutoff values, patients were divided into two groups and data were compared with the Kaplan–Meier method and log-rank test. Patients who were alive 180 days after admission were censored for analysis. For calculating sample size, we assumed that at least 100 patients with all examination results were needed to calculate accuracy within 20% width in 95% confidence intervals for a 50% value. The independence of each WPCBAL score factor was verified by calculating the phi coefficient, where 1 was assigned when a patient's laboratory test value exceeded the criteria listed in Table 1 and 0 was assigned when it did not. Statistical analysis was performed using Bell Curve (Social Survey Research Information Co., Ltd., Tokyo, Japan) for Excel (Microsoft Corporation, Redmond, WA). p-Values <0.05 were considered significant.
Ethical consideration
This study was approved by the ethical committee of Ashiya Municipal Hospital and the Pharmaceutical Sciences of Osaka University.
Results
Patient backgrounds are presented in Table 2. Median (interquartile range [IQR]) age was 77.5 (71.0–84.0) years. Ninety patients (70.3%) had ECOG PS of ≥3. Median (IQR) duration between admission and death was 19 (8–49) days.
Patient Demographics
BMI, body mass index; ECOG PS, Eastern Cooperative Oncology Group Performance Status; IQR, interquartile range.
The percentage of deaths according to WPCBAL score and GPS and the Kaplan–Meier survival curves for the three groups are presented in Figure 1. For WPCBAL score, mortality rates within three and two weeks after admission were both the highest at 5 points (35.4% and 38.9%, respectively). For GPS, mortality rates within three weeks after admission were highest at 2 points (87.7%). The Kaplan–Meier survival curves for the three groups showed that survival rates differed among them (log-rank test, p < 0.001 for all). After calculating the phi coefficient, no significant correlation was found between each WPCBAL score factor (Appendix Table A1). Figure 2 shows ROC analysis results. The closest WPCBAL score totals from the upper left corner were 4 and 5 within three and two weeks after admission, respectively. Figure 3 shows survival analysis results. For death within three weeks after admission, patients with WPCBAL score of ≥4 points had significantly higher mortality than did those with ≤3 points (p < 0.001, Fig. 3A). For death within two weeks after admission, patients with WPCBAL score of ≥5 points showed significantly higher mortality than did those with ≤4 points (p < 0.001, Fig. 3B). Table 3 shows the sensitivity, specificity, PPV, NPV, accuracy, and AUROC of each prognostic method calculated using the cutoff values from ROC and survival analyses. The GPS cutoff value was set to 2, according to Miura et al. 5 For predicting three-week prognosis, WPCBAL score had higher AUROC (0.7540), specificity (0.635), PPV (0.676), and accuracy (0.688) than did GPS. WPCBAL score for two-week prognosis had higher AUROC (0.7491), specificity (0.784), PPV (0.673), and accuracy (0.711) than did GPS for three-week prognosis.
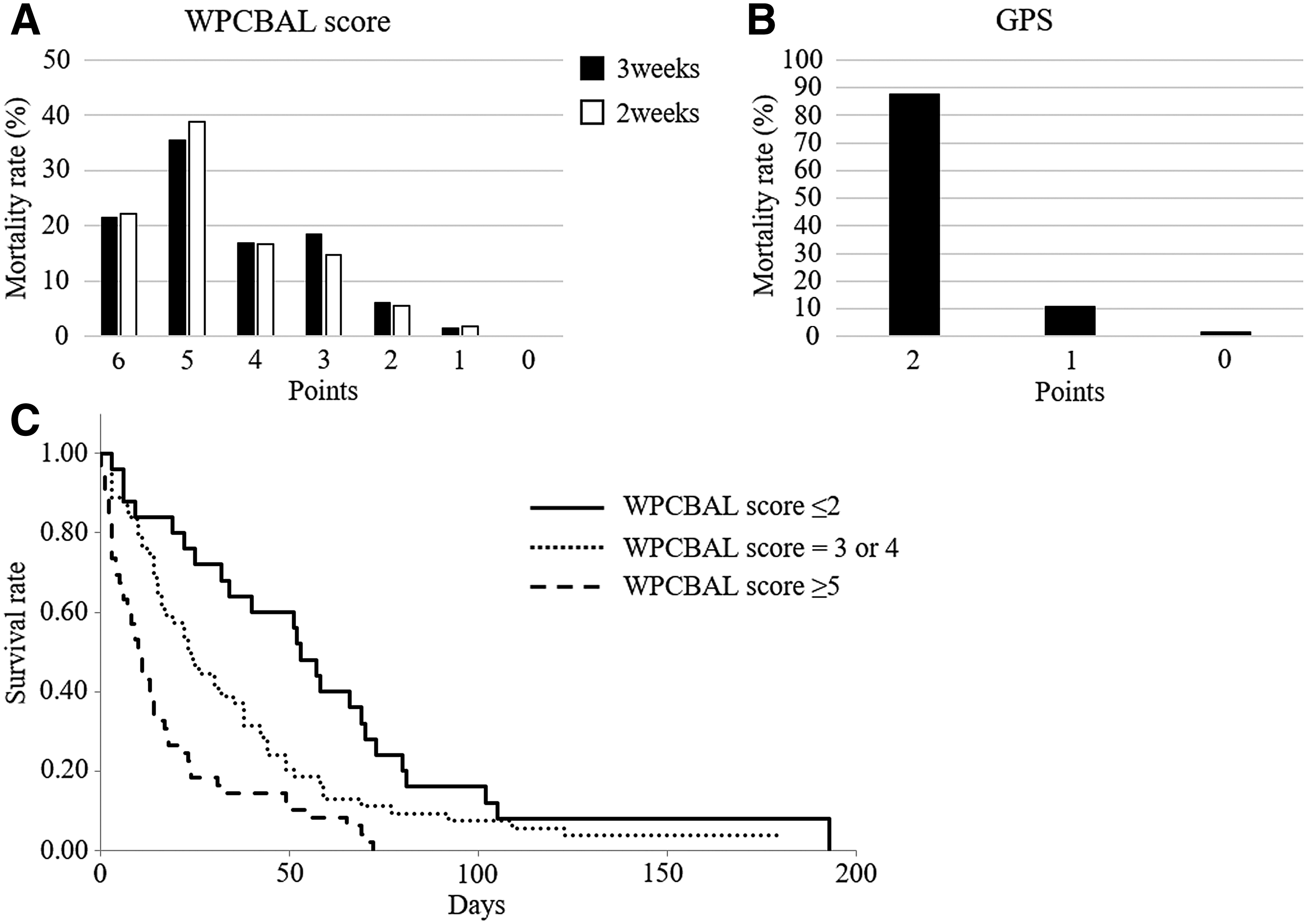
Percentage of deaths according to WPCBAL score and GPS, and survival rate classified as low points, middle points, or high points with respect to WPCBAL score. In WPCBAL score and GPS, 1 point is given when the laboratory test values of the items constituting each method satisfy the criteria presented in Table 1. In the WPCBAL score
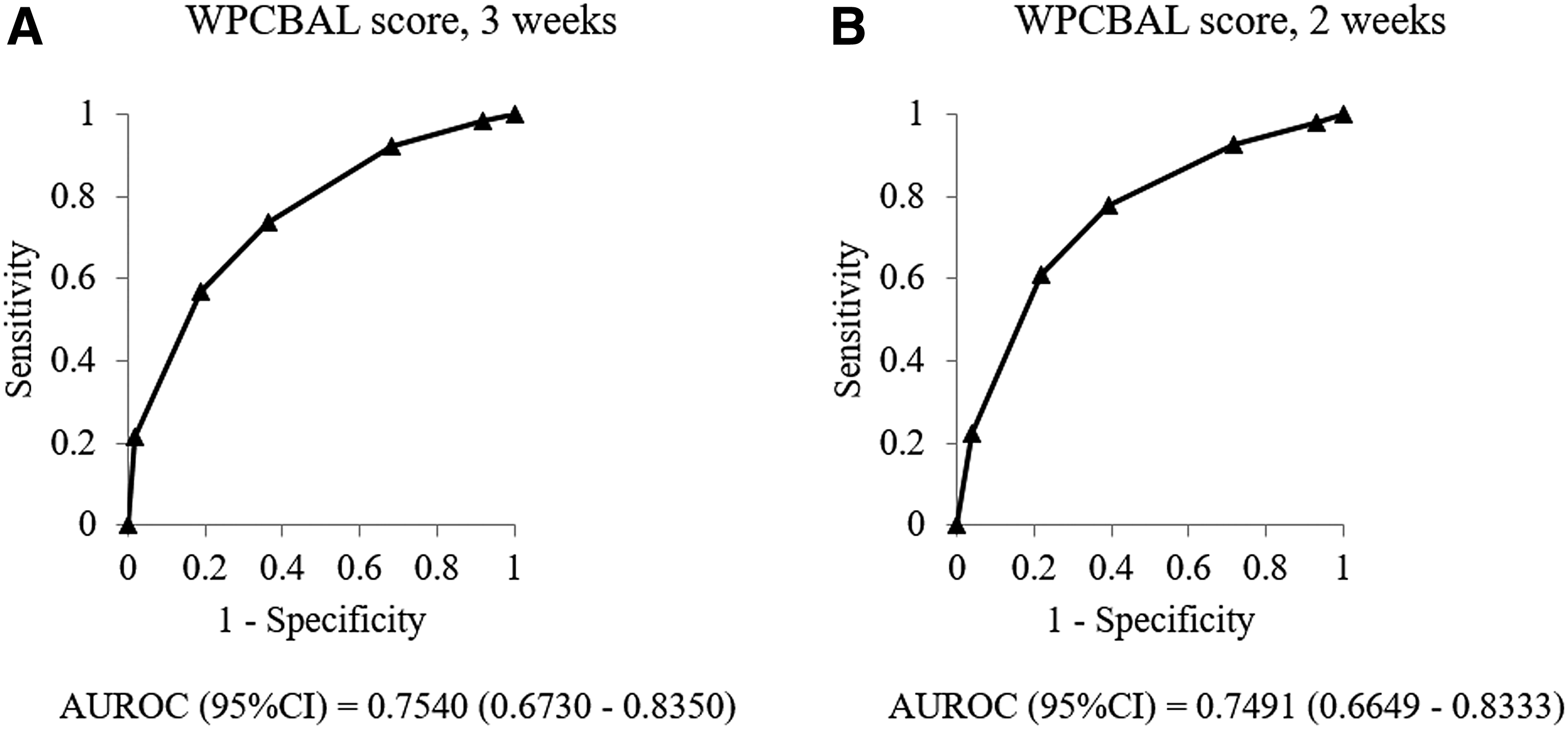
ROC analysis. The points of WPCBAL score were defined as independent variables, and death within three weeks
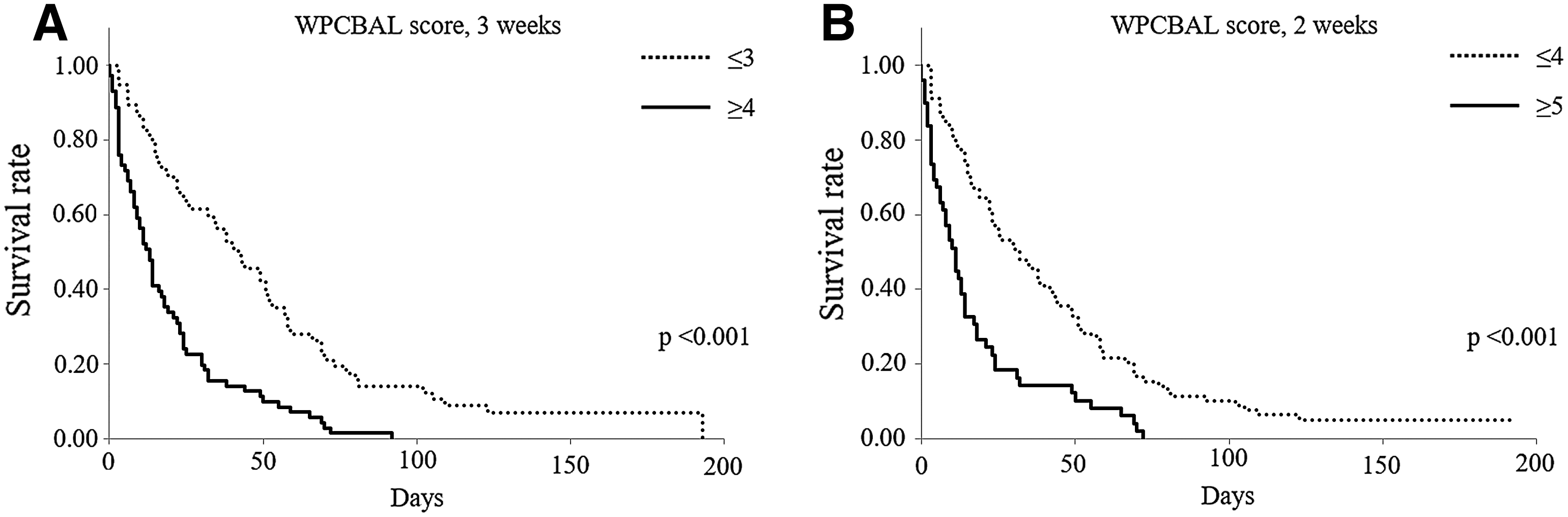
Survival analysis. Patients were divided into two groups based on the cutoff values calculated by the ROC analysis for WPCBAL score to predict the three-week prognosis
Sensitivities, Specificities, Positive and Negative Predictive Values, Accuracies, and Area Under the Receiver Operating Characteristic Curves of WPCBAL Score, and Glasgow Prognostic Score
AUROC, area under the receiver operating characteristic curve; CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value.
Discussion
Our findings suggest that WPCBAL score can objectively predict two- or three-week prognosis for terminal cancer patients in palliative care units. For predicting three-week prognosis, WPCBAL score had higher AUROC than did GPS. GPS predicts three-week prognosis with higher sensitivity than did the PPI. 5 WPCBAL score had higher specificity, PPV, and accuracy than did GPS, and the sensitivity, specificity, PPV, NPV, and accuracy showed moderate or high values of >0.6; however, GPS showed low specificity (0.429).
Currently, no method can predict two-week prognosis with only objective indices. However, the AUROC, specificity, PPV, and accuracy of WPCBAL score in predicting two-week prognosis were superior to those of GPS in predicting three-week prognosis.
The WPCBAL score is a versatile tool because its parameters can be measured by routine blood tests. While GPS also has this advantage, WPCBAL score is more accurate in predicting prognosis. This may be because, compared with GPS, WPCBAL score utilizes more indices reflecting physical changes occurring before death. Previous reports have revealed that WBC, BUN, AST, LDH, and CRP increase, but PLT and Alb decrease before death.12–17
This study had some limitations. First, since it was retrospective, WPCBAL score could not be directly compared with existing prognostic predictive methods like the PPI and Prognosis in Palliative care Study predictor models, 18 which are used to predict two-week prognosis. Second, the findings, including the cutoff values in Table 1, cannot be generalized because verification was performed at a single facility. Therefore, a multicenter validation study is required to improve the accuracy of WPCBAL score.
We suggest that WPCBAL score can objectively predict two- or three-week prognosis for terminal cancer patients in palliative care units. The usefulness of this score must be verified in the future by prospectively comparing it with commonly used prognostic predictive methods at international multiple facilities.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
The Correlation among Factors of WPCBAL Score by Calculating the Phi Coefficient
| WBC ≥4.87 × 10 3 /μL | PLT ≤225 × 10 3 /μL | CRP ≥2.75 mg/dL | BUN ≥14 mg/dL | AST ≥30 U/L | LDH ≥264 U/L | |
|---|---|---|---|---|---|---|
| WBC ≥4.87 × 10 3 /μL | 1 | |||||
| PLT ≤225 × 10 3 /μL | −0.201226439 | 1 | ||||
| CRP ≥2.75 mg/dL | 0.069924681 | −0.038263668 | 1 | |||
| BUN ≥14 mg/dL | 0.136378832 | 0.025963697 | −0.033180919 | 1 | ||
| AST ≥30 U/L | 0.165856471 | 0.060435527 | −0.006665284 | 0.136742135 | 1 | |
| LDH ≥264 U/L | 0.09166985 | 0.234632917 | 0.299854676 | 0.184427778 | 0.516192418 | 1 |
AST, aspartate aminotransferase; BUN, blood urea nitrogen; CRP, C-reactive protein; LDH, lactate dehydrogenase; PLT, platelet; WBC, white blood cell.