
Abstract
Abstract
Background:
Involvement of the palliative care service has potential for patient and family benefit in critically ill patients, regardless of etiology. Anecdotally, there is a lack of involvement of the palliative care (PC) service in the neuro-intensive care unit (neuro-ICU), and its impact has not been rigorously investigated in this setting.
Objective:
This study aims at assessing the effect of early involvement of the PC service on end-of-life care in the neuro-ICU.
Design:
Demographic variables and elements pertaining to the end-of-life care were obtained retrospectively via the electronic medical record from patients receiving their care at the University of Alabama at Birmingham Hospital neuro-ICU. The patient population was divided into two cohorts: patients who received PC services and patients who did not. Contingency analysis was performed to assess for associations with PC service involvement.
Results:
A total of 149 patients were included in the study. PC services were included in 56.4% of the cases. Involvement of the PC service led to more code status changes to comfort care–do-not-resuscitate p = 0.0021. This was more often a decremental change to less invasive measures rather than a direct change from full code to comfort care measures (p = 0.026). When PC specialists were involved, medications to treat anxiety/agitation, dyspnea/pain, and respiratory secretions were utilized more frequently (p < 0.001) and fewer procedures were performed on these critically ill patients within 48 hours of death (p < 0.001).
Conclusion:
Early involvement of the PC service has an impact on adjusting the treatment paradigm for patients suffering from devastating neurologic injuries. We recommend the creation of a standardized protocol to ensure early PC consultation in the neuro-ICU based on initial patient presentation parameters, imaging characteristics, and prognosis.
Introduction
I
As the ICU can already include a multidisciplinary approach to patient care, there exists a great opportunity to more regularly involve PC specialists in the care of the hospital's sickest and most complex patients. Currently, however, clinicians report that PC consultation is underutilized in the ICU setting, perhaps secondary to concerns regarding the appropriate roles of PC specialists in the ICU as well as the impact that this role may have on the relationship between the ICU team and patients' families. 5 A case history is illustrated in Table 1.
CC-DNR, comfort care–do-not-resuscitate; neuro-ICU, neuro-intensive care unit; PC, palliative care.
A case such as this is common in the neuro-intensive care unit (neuro-ICU), characterized by an often sudden decline in neurological functioning. In many cases, these patients have preexisting deficits or significant medical comorbidities. Barriers to utilizing palliative and end-of-life care services among surgeons include a lack of formal training, difficulty with prognostication, communication challenges, and discordant expectations between physician and family. 6 The ability (or inability) to prognosticate on both mortality and functional outcome is a major challenge across many terminal diseases, not only neurologic injuries. Physician gestalt and clinical judgment is likely less accurate than formal and validated scoring systems, particularly in stroke. 7 Scoring systems such as the intracerebral hemorrhage (ICH) score, ASTRAL, DRAGON, and Hunt Hess score offer validated and accurate (though at times imperfect) means for estimating mortality and/or functional outcome. 8
Within the neuro-ICU, many patients and their families could benefit from early involvement of PC services, especially in cases of nonsurvivable or catastrophic injury present at initial patient presentation. Unfortunately, patients with severe neurologic disease often do not receive PC consults, and those who do only receive it for discussion of hospice candidacy or comfort measures toward the end of their life rather than early in their hospital course. 9 The purpose of this study was to determine how involvement of the PC service affects a patient's end-of-life course. We suspect that early involvement of PC better facilitates the utilization of medications that mitigate symptom burden and suffering. In addition, PC services may provide a context to further establish goals of care early in the hospital course.
Methods
Institutional IRB approval (X141021004) was obtained for retrospective data collection via the electronic medical record from patients admitted to the neurosurgery service who received their care at the University of Alabama at Birmingham Hospital from May 2012 to July 2014. This included patients admitted to the neurosurgery service who either died in the neuro-ICU or were ultimately transferred to the inpatient PC unit. Data involving demographics and end-of-life care included: age, intracranial pathology (subarachnoid hemorrhage, traumatic brain injury, intracerebral hemorrhage, intracranial tumor, other), gender, code status, PC consultation, direct or graduated change of code status, restraints ordered, pastoral care consultation, palliative medications ordered to treat pain/dyspnea, anxiety/agitation, nausea/vomiting, and respiratory secretions. Outcome variables included: the time from code status change to PC consultation, and time from change to comfort care–do-not-resuscitate (CC-DNR) to death or transfer to the PC unit. Additional variables of interest included the number of PC visits/consults before transfer or death, the number of procedures performed in the 48 hours before death, and the etiology of death. Contingency analysis was performed by utilizing t tests, analysis of variance, and chi-square testing when appropriate.
Results
A total of 149 patients were included in the study. A representation of the cohort demographics and end-of-life course is included in Table 2. Admission diagnoses among these patients included intracerebral hemorrhage (28.2%), intracranial neoplasm (25.5%), traumatic brain injury (22.2%), subarachnoid hemorrhage (20.1%), and other (4.0%). A code status change to CC-DNR was ordered in 80.5% of the cohort. PC was consulted for 56.4% of patients. Palliative extubation was the most common mechanism of death (61.7%), followed by brain death (21.4%), cardiac arrhythmia (10.2%), and pulmonary failure (6.7%)—Figure 1. PC service involvement was associated with more frequent code status changes to CC-DNR (p = 0.0021).
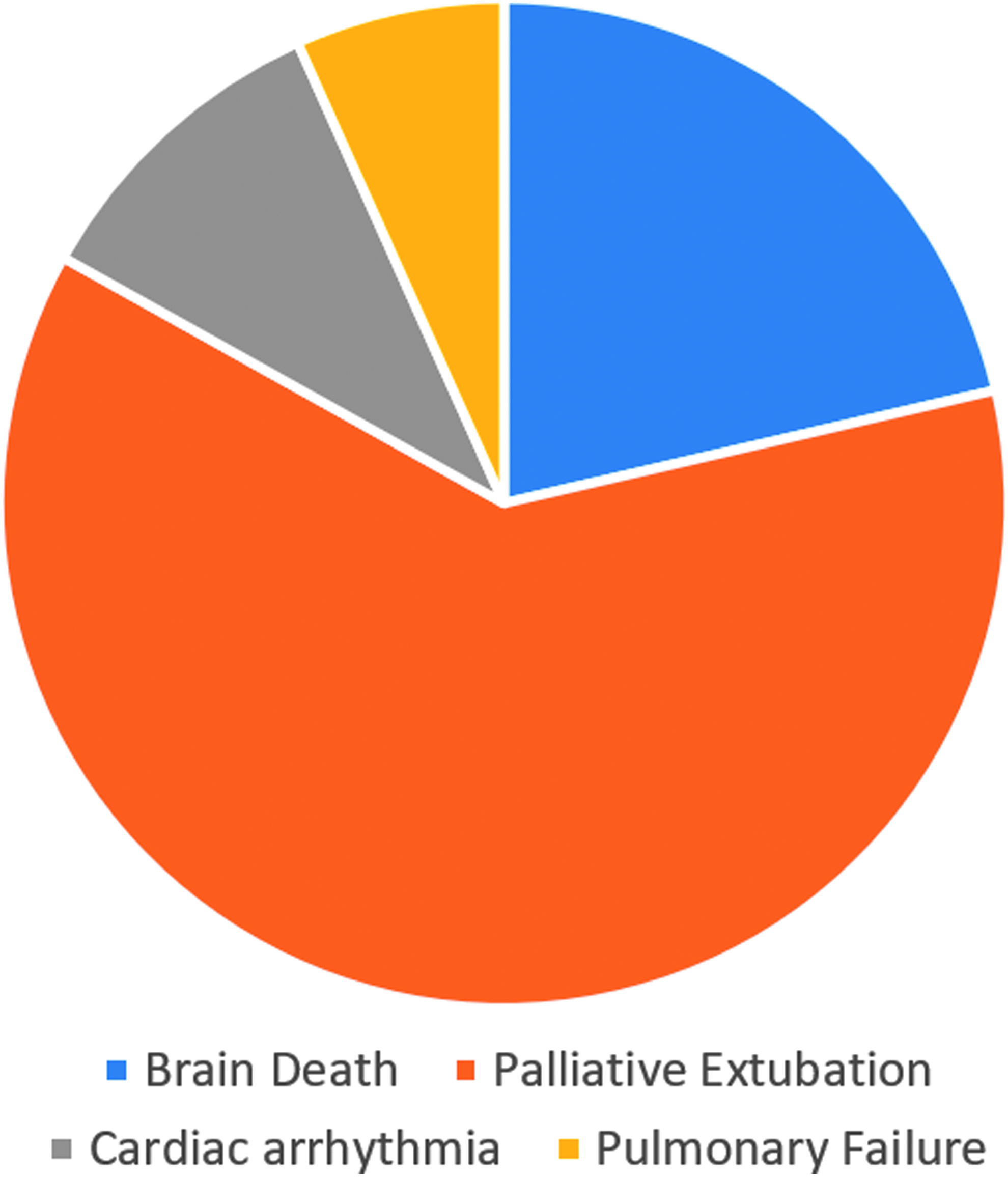
Mechanism of death.
SD, standard deviation; SE, standard error.
Bold indicates clinically significant variables.
When PC was involved, this code status change was more frequently a decremental change to less invasive measures, from “full resuscitation” to “full support-DNR,” rather than a direct change from full code to comfort care (p = 0.026). In addition, fewer procedures were performed in these critically ill patients 48 hours before death when PC was involved (p < 0.001). In those patients in whom PC was involved, the mean time from code status change to death was 82 hours. Medications to treat pain, dyspnea, anxiety, agitation, and respiratory secretions were used more frequently in patients with PC service involvement (p < 0.001). PC consultation was associated with prolonged time from CC-DNR status change to death when compared with patients without PC involvement (p < 0.001). There was no association between PC involvement and patient gender, whether a code event occurred, or whether restraints were used within 48 hours of death.
Discussion
Patients with catastrophic neurologic injuries represent a population whose hospital care can be enhanced by drawing on the expertise of our colleagues in PC. Holloway et al. compared the pattern of PC consultations in stroke patients with nonstroke patients and reported that only 6.5% (101/1551) of all stroke admissions during a three-year study period received a PC consultation. 10 Physicians' attitudes regarding PC as well as patient progression and recovery goals likely affect the utilization of the PC consult service. Using in-person interviews of trauma surgeons and neurosurgeons, Tilden et al. found that a patient's prognosis, location in their illness trajectory, and the surgeon's desired outcomes are commonly involved in the decision-making pathway of whether or not to consult PC. 11 Interestingly, patients in whom imminent death was expected early in the hospital course and those who were expected to survive with few deficits would not typically receive PC consults, whereas those expected to die after a prolonged illness course or to have chronic deficits without improvement did receive PC consults. 12
Incorporating PC as a regular component of patient care in the neuro-ICU may aid in addressing goals of care, medical futility, hospice, and symptoms such as refractory pain, dyspnea, agitation, and depression.12–14 In this study, it is concerning how medications to treat pain, dyspnea, anxiety, and agitation were sparsely utilized when PC was not involved. This may be attributed to the fact that these medications are often explicitly avoided in the setting of severe neurologic injury, since scheduled neurologic exams are a key component to the care and assessment of these patients while being fully resuscitated.
Given the relative shortage of PC clinicians, it may be beneficial to incorporate PC methods during an intensivist's training. In addition, readily available order sets within the electronic medical record may guide providers who are less experienced in providing PC.
Metrics such as the Hunt Hess score for subarachnoid hemorrhage, ICH score for hemorrhagic stroke, and ASTRAL or DRAGON scores for ischemic stroke can help clinicians identify patients who may benefit from early involvement of PC. We propose a structured approach to include PC consultation for all patients admitted to the neuro-ICU with poor scores on the measures described earlier. We plan to pilot such a program where patients with poor predicted outcome receive consultation from the PC team within 24 hours of admission or neurologic decline. Future studies should focus not only on effective symptom palliation at end of life but also on cost-effectiveness, and physician and family perceptions on care delivery.
Conclusion
In our study, consultation of the PC service was associated with increased use of medications aimed at symptom palliation, a more gradual transition from full code to comfort measures only, and fewer invasive procedures within 48 hours of death. We advocate for more standardized utilization of palliative services in patients who present with a poor neurologic prognosis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.