
Abstract
Abstract
Background:
Latinos with end-stage renal disease (ESRD) have worse mental and kidney composite health-related quality of life (HRQOL) scores compared to non-Latino ESRD patients. Latino ESRD patients uniquely report that social factors (e.g., lack of care coordination, food insecurity, and low health literacy) and mental health influence their HRQOL. We developed a culturally tailored peer navigator (PN) intervention to improve the HRQOL of Latinos on hemodialysis.
Objective:
To determine the feasibility of the PN intervention.
Design:
Single-arm prospective study. The PN provided individualized support with advance care planning, care coordination, and counseling about the importance of diet and mental health.
Setting and Participants:
Latino with ESRD receiving scheduled outpatient thrice-weekly hemodialysis or reliant on emergency-only hemodialysis in Denver.
Main measures:
Recruitment, retention rates, data completeness, intervention dose, patient- and staff-reported satisfaction with the intervention.
Results:
Of 49 eligible patients, 40 (82%) agreed to participate. The majority of participants received scheduled outpatient hemodialysis (75%), 20 were women (50%), with a mean (standard deviation [SD]) age of 56 (13) years. No participants withdrew from the intervention. One participant died. The mean (SD) number of PN visits per participant was 7 (2) and the mean (SD) length of the visits was 97 minutes (49). The majority of visits took place at the hemodialysis facility (59%) and home (27%). The vast majority of participants reported that the PN improved their quality of life as a patient on hemodialysis (95%).
Conclusions:
The PN intervention achieved feasibility goals and was well received by participants.
Introduction
Latinos represent 17% of the United States end-stage renal disease (ESRD) population, yet, remain underrepresented in existing ESRD research. 1 Compared to the general United States population, patients with ESRD have a lower life expectancy, lower health-related quality of life (HRQOL), and a symptom burden similar to patients with advanced cancer.2–9 Multiple factors (e.g., symptom burden, mental health) associated with ESRD can affect HRQOL. In Latinos, these concerns are compounded by cultural factors (i.e., behaviors and values), social factors (i.e., socioeconomic status, health literacy), and access to hemodialysis (i.e., undocumented immigrants rely on emergency-only hemodialysis).4,10,11–14
A peer navigator (PN) intervention that provides individualized support by addressing patient-identified barriers and facilitators to care within a dialysis center has the potential to improve HRQOL. A PN (i.e., patient navigator, community health worker, lay health worker, or promotora) is a culturally and linguistically congruent individual who helps patients achieve their health care goals by helping them overcome modifiable barriers and facilitating the interaction between the patient and the health care system. The objective of this study was to assess the feasibility and acceptability of a PN intervention for Latino patients with ESRD receiving scheduled or emergency-only hemodialysis.
Methods
Design
This is a prospective, single-arm study conducted from January 2016 to December 2017 to assess the feasibility of a large-scale randomized controlled trial (RCT). The Colorado Multi-institutional Review Board approved this study.
Setting and participants
Participants were recruited from January 2016 to May 2017 at an inpatient dialysis center at a safety-net hospital, and at an outpatient inner city dialysis center in Denver, Colorado. Eligible participants were English or Spanish-speaking Latinos with ESRD receiving scheduled thrice-weekly outpatient hemodialysis or emergency only hemodialysis (EOHD). EOHD patients are undocumented immigrants with ESRD who must meet critically illness criteria (e.g., high potassium; uremic symptoms; and/or severe shortness of breath) to receive hemodialysis, while admitted to hospital. Patients were excluded from the study if they were <18 years of age, not Latino, pregnant, incarcerated, or lacked decisional capacity.
PN intervention
A community advisory panel composed of patient and caregiver stakeholders provided guidance on the tailoring of the PN intervention, informed by our previous research on the HRQOL preferences and needs of Latino ESRD patients.10,13,14 The PN intervention focused on four domains: (1) advance care planning (ACP); (2) care coordination; (3) dietary support; and (4) mental health support (Appendix Table A1). We chose a maximum of five planned visits based on preliminary studies. 15 The PN continued to be available to participants if they requested additional visits.
PN training
The PN, a Latina fluent in English and Spanish, had personal experience as a caregiver for her ESRD family member. The PN also had previous experience in the health-related field as a medical Spanish interpreter for a safety-net hospital for four years and training as a certified nurse assistant. The PN was trained in motivational interviewing and navigator fundamentals through the Colorado Patient Navigator Training Program. 16
Outcome measures and data collection
The primary outcomes were feasibility and acceptability. To assess feasibility, we tracked recruitment and retention, intervention implementation, data collection, and intervention delivery (e.g., number of visits, visit duration, and visit content through detailed field notes). To measure patient acceptability, we used a modified version of the Patient Navigation Process and Outcomes Measure. 15 To measure dialysis center staff acceptance, we conducted semistructured interviews.
Exploratory measures were collected at baseline and study completion. Measures included the following: (1) Kidney Dialysis Quality of Life Short Form (KDQOL-SF 36)17,18; (2) Modified Edmonton Symptom Assessment Scale (ESAS-r:Renal) 19 ; (3) Patient Health Questionnaire-9 (PHQ-9); and (4) Generalized Anxiety Disorder-7 (GAD-7). To assess acceptability, L.C. conducted semistructured interviews with the PN and hemodialysis center staff. Interviews were audio recorded and transcribed.
Statistical analysis
Descriptive analyses were conducted using SAS Enterprise Guide 5.1 (SAS Institute, Inc., 2012). For continuous and normally distributed data, we calculated means with standard deviation (SD). Numeric counts with a percent were calculated for categorical variables. Our study was not powered to detect changes of exploratory measures, and we thus provide the results at baseline only. ATLAS.ti software (version 8.0.27.0) was used for thematic analysis of transcribed interviews.
Results
In total, 40 (30 scheduled hemodialysis and 10 EOHD) participants were enrolled. Participants had a mean (SD) age of 56 (13), a mean (SD) Charlson Comorbidity Index of 7.2 (2.7), 20 (50%) were female, and 28 (70%) were primarily Spanish-speaking (Table 1). Nearly one-third of participants had at least moderate depression (PHQ-9 ≥ 10) and/or moderate anxiety (GAD-7 ≥ 10). The ESAS-r: Renal showed that patients report a mean (SD) of 6 (3) symptoms, of which 4 (4) were moderate to severe.
Patient Characteristics
SD, standard deviation; KDQOL-SF, Kidney Dialysis Quality of Life Short Form; ESAS-r:Renal Modified Edmonton Symptom Assessment Scale; PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalized Anxiety Disorder-7; IQR, interquartile range; CVD, cardiovascular disease.
Feasibility
With respect to feasibility, 49 patients were approached and 40 (82%) agreed to participate. Of the 40 participants, none withdrew, and data collection was complete except for one participant who died (Fig. 1). Nearly all (95%) participants completed the five-visit protocol within 90 days. Overall, the mean (SD) number of visits was 7 (2), and the mean (SD) length of the visits was 97 (49) minutes. The majority of visits took place at the dialysis facility (59%) or the participant's home (27%) (Table 2).
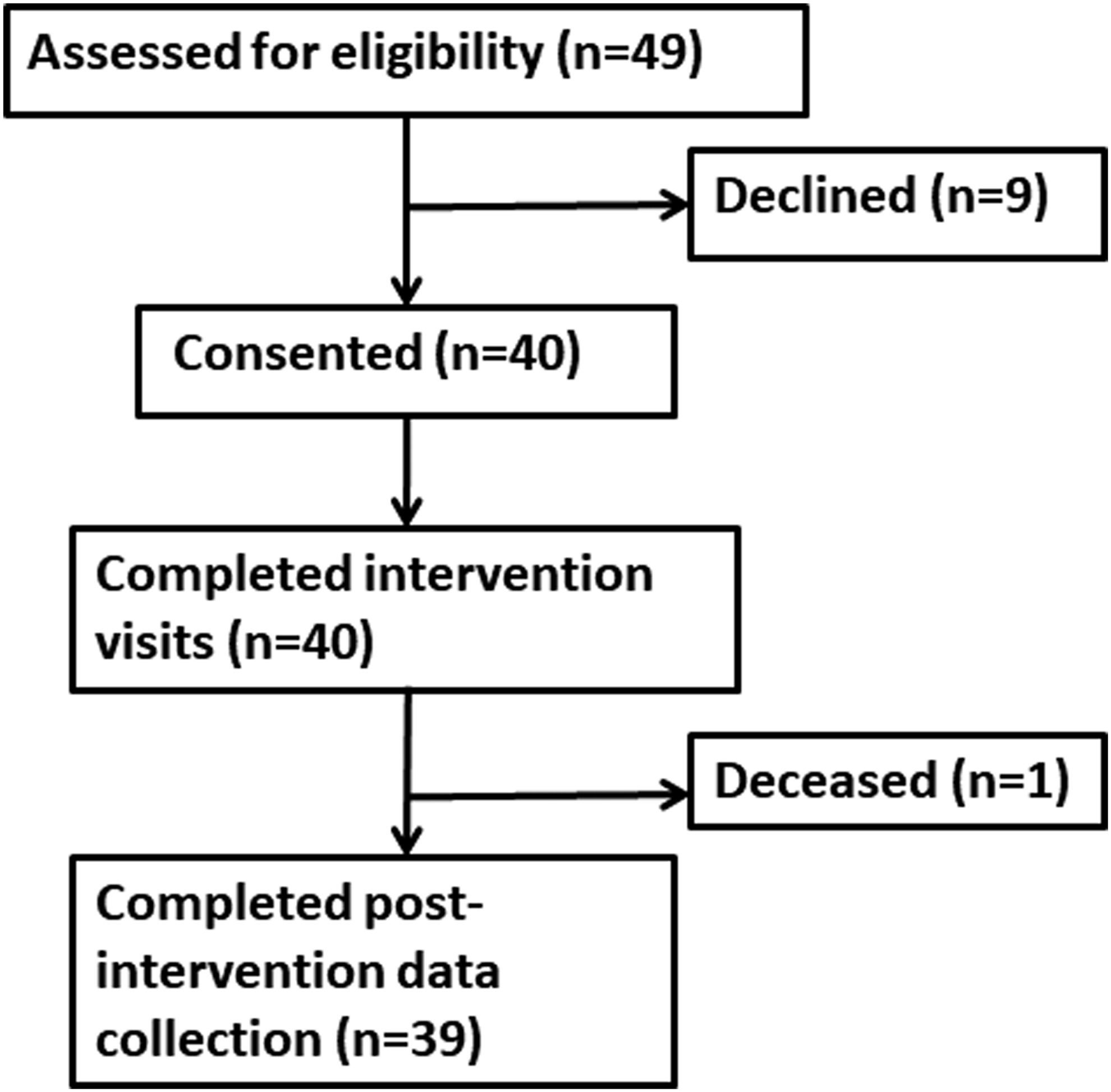
Study flow diagram.
Intervention Feasibility
Acceptability
The majority of participants felt that the PN improved their quality of life (95%), provided emotional support (100%), and helped them make important decisions about care (100%) (Table 3). When asked about the domains, the majority reported having discussed ACP (90%), diet (92%), mental health (95%), and having received social support with basic resources (e.g., food, housing, disability, and transportation paperwork) (95%). All dialysis center staff interviewed agreed that the intervention was well received by patients (Table 4). Staff also reported an increase in the number of patients listed for a kidney transplant and improvement of renal therapy adherence. The PN identified a major challenge in supporting depressed participants to seek mental health treatment due to a mix of cultural preferences and communication barriers.
Patient Acceptability, Patient Navigation Process Outcomes Measure
N = 39.
Illustrative Quotes from Acceptability Interviews
Discussion
To our knowledge, this is the first prospective culturally tailored PN program focused on improving HRQOL for Latino ESRD patients. Our findings demonstrated its feasibility and acceptability.
The high referral, enrollment, and retention rate as well as acceptability of this study are strengths. In this pilot study, the PN introduced the study and credited this initial recruitment encounter with enhancing study retention because participants developed a trusting relationship that may have facilitated subsequent visits. We designed the PN intervention to include five navigator-initiated visits for each intervention participant; however, the mean (SD) number of visits was 7 (2) and one-third of participants reported that the number of visits was “not enough” indicating a desire for ongoing support. Participants felt that the PN provided emotional support, improved their lives, and/or the health care they received. Our findings are consistent with the emotional support reported in a systematic review of the experiences of cancer patients in navigation programs. 20
One of the challenges faced by the PN was in supporting participants who faced depression and anxiety. Previous research demonstrated that patients with mental health issues did not want medications and did not want to see a psychiatrist or psychologist due to social stigma and their demanding hemodialysis schedule.10,13,14 In our study, the PN used motivational interviewing to connect participants to mental health services; however, participants were reluctant to follow-up with mental health care. An innovative approach that aligns with Latino ESRD participant preferences is Chairside Cognitive Behavioral Therapy (CCBT) delivered by a Licensed Clinical Social Worker during hemodialysis. In a small RCT of CCBT, English-speaking ESRD patients randomized to CCBT had a reduction in self-reported depression, greater improvement in HRQOL, and hemodialysis fluid adherence. 21 These findings are promising; however, more research is needed on the use of CCBT for minority ESRD groups.
Navigator programs have been highlighted by the nephrology community as an important strategy to address inequities. 22 Ethnic minorities are disproportionately burdened with both a high prevalence of ESRD and face inequities in various ESRD outcomes, including end-of life care.14,23 For example, compared to non-Latino Whites, Latino ESRD patients are less likely to report engagement in a conversation about ACP. 23 When examining patterns of end-of life care, Latino ESRD patients with a hospital death are more likely to receive intensive procedures during their last hospitalization. 24 In our study, the majority of participants reported having a conversation about ACP with their PN and their health care provider. Having a culturally congruent PN support, ACP has the potential to promote goal concordant care.
Our study has limitations, some of which are inherent to its design as a feasibility study. While this early pilot work was not powered to detect changes postintervention, we were able to demonstrate that the intervention could be successfully delivered. An additional limitation is that we had one highly invested PN who was culturally congruent with the study participants and in a single research setting. Future trials will be necessary to demonstrate fidelity in conducting the intervention and reproducibility in other hemodialysis centers,
In conclusion, we demonstrated that the PN intervention is feasible for Latinos on hemodialysis. A future multi-site RCT of the PN intervention among Latino groups could examine HRQOL, hemodialysis adherence, and kidney transplantation outcomes.
Footnotes
Acknowledgments
The work was supported by the Harold Amos Medical Faculty Development Award from the Robert Wood Johnson Foundation and grant 2015212 from the Doris Duke Charitable Foundation (University of Colorado School of Medicine Fund to Retain Clinical Scientists). The funding agencies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit article for publication.
Author Disclosure Statement
No competing financial interests exist.
Appendix
Appendix Table A1. Framework for Peer Navigator Visit by Domain
| Social support | Mental health support | ||
|---|---|---|---|
| Advance care planning | Care coordination | Diet support | |
| • Discuss values and goals using motivation interviewing through empathy and reflective listening. • Review advance directive and hospice educational materials • Use motivational interviewing to help patient complete advance directives and/or have advance care planning conversations with family and clinicians. |
• Discuss concerns related to health, finances, housing, transportation, and family. • Provide support with connection to community resources, clinic appointments, language interpretation, and logistical issues. |
• Accommodate cultural dietary preferences with renal restriction. • Provide recipes that are culturally and linguistically congruent. • Activate patient to troubleshoot diet issues. |
• Explore patient methods for coping and adjustment to illness. • Use motivational interviewing, and help patient obtain mental health support. |