
Abstract
Abstract
Background:
Given the limited ability of hospice patients to assess, monitor, and respond to substandard care, quality oversight has an important role to play in the hospice sector. The IMPACT Act of 2014 required that agencies be recertified at least every three years, but it did not otherwise alter hospice quality oversight.
Objectives:
To illuminate the current hospice quality oversight process and discuss its role alongside other government monitoring and public reporting efforts.
Methods:
Retrospective analysis (2006–2015) concerning hospice accreditation status, deficiency trends, survey frequency and deficiency outcomes, and termination from the Medicare program.
Results:
The proportion of privately accredited hospice agencies increased from 15% to 39%, a trend driven largely by its increased use among for-profit agencies. The combined rate of deficiencies per agency increased 35% over the past decade, with issues around care planning, aide and homemaker services, and clinical assessment featured most prominently. Nearly half (45%) of all surveys resulted in deficiency citations; however, less than one-in-four hospice agencies were surveyed in a given year. Over the past decade, 28 agencies were terminated from the Medicare program; most of these agencies were unaccredited and operated on a for-profit basis.
Conclusions:
The IMPACT Act addressed one of the biggest shortcomings in hospice oversight. Our findings highlight additional reforms that could be considered. First, reporting inspection results from private and public recertification surveys could promote greater transparency and accountability. Second, making a wider range of intermediate sanctions available to oversight agencies could enhance enforcement efforts and, ideally, incentivize agencies to improve quality of care.
Introduction
Following media reports alleging aggressive hospice enrollment practices and deficient care,1–4 the IMPACT Act of 2014 included provisions to bolster hospice quality oversight, which had previously been minimal. The IMPACT Act required that hospice agency recertification surveys occur at least once every three years, representing the first statutory requirement for hospice survey frequency. The provision addressed a longstanding critique that hospice agencies could go several years without being surveyed.5–7 Along with the modestly enhanced certification standards, efforts to increase the availability and transparency of quality information have progressed as hospice agencies have begun reporting information on a range of quality measures as part of the Affordable Care Act-authorized Hospice Quality Reporting Program (HQRP).
Given the frail hospice patient population and their limited ability to assess, monitor, and respond to poor quality care, hospice quality oversight and monitoring have important roles to play. Following initial praise for the enhanced hospice quality oversight standards promulgated by the IMPACT Act, 8 there has been little discussion among policymakers and other stakeholders about hospice quality assurance and how to ensure its effectiveness. Outside of establishing a minimum frequency for recertification surveys, the IMPACT Act did little to alter the regulatory framework guiding hospice quality assurance efforts. Yet, as highlighted by recent reports by Kaiser Health News and the Office of the Inspector General, the current framework of hospice quality oversight arguably falls short of protecting patients in instances where poor quality care occurs.9,10
This article will illuminate the current hospice quality oversight process and discuss its role alongside other government monitoring and public reporting efforts. The article will focus in particular on efforts to assess and monitor hospice agencies' compliance with Medicare and Medicaid program requirements, commonly referred to as conditions of participation. Using longitudinal data from 2006 to 2015, the analyses document hospice agencies' accreditation status, detail hospice deficiency trends, and describe hospice agencies that have been terminated from the Medicare hospice program as a result of poor quality care.
Background
The federal statutes governing hospice fall under the purview of the Social Security Act of 1935.* These statutes provide the basic framework for the hospice benefit, and the regulations promulgated thereunder by the Department of Health and Human Services and the Centers for Medicare and Medicaid Services (CMS) further delineate conditions of participation in Medicare and detail the elements of quality oversight, the focus of this article. These regulations are found in 42 U.S.C. §1395 × and 42 C.F.R. §§418.52–419.78 and 418.100–418.116. To support states' implementation of these standards, the CMS Central Office also publishes the State Operations Manual, which includes guidance for interpreting the law and implementing federal regulations and details instructions for monitoring and enforcement. 11
Similar to other types of health care providers participating in Medicare, state agencies are generally responsible for licensure of hospice agencies and for assessing their compliance with federal quality standards. As it does for entities like hospitals and home health agencies, CMS allows hospice agencies to be certified or “deemed” compliant with conditions of participation either by state governmental agencies or by private accrediting bodies, such as the Joint Commission, the Community Health Accreditation Program, and the Accreditation Commission for Health Care. As mentioned above, the IMPACT Act of 2014 required that hospice recertification surveys occur at least once every three years. 12 This provision is currently scheduled to sunset in 2025 but can be renewed if it proves successful in improving patient care.
Beyond standard certification surveys, state and federal oversight agencies are also responsible for investigating reported incidents and complaints. When hospice patients suffer an adverse event or are dissatisfied with the quality of care rendered by an agency, they can file formal complaints to regulatory agencies. States are generally responsible for investigating these complaints, doing so in accordance with guidance included in the State Operations Manual. State agencies may also perform “validation” surveys on a small sample of privately accredited agencies to ensure that accrediting organizations are fulfilling their oversight responsibilities.
States have primary responsibility for enforcement of existing standards. Beyond ensuring that hospice agencies are certified, state agencies are responsible for addressing quality violations when they arise and working with providers to address identified problems. Importantly, oversight agencies are limited in their ability to sanction out-of-compliance providers and spur them to improve. In fact, although it can be relatively common to find deficiencies upon inspection (e.g., a 2013 OIG report found that 46% of hospice surveys resulted in health deficiency citations 6 ), the only sanction available to oversight authorities if providers do not correct identified deficiencies is termination from the Medicare program, an extremely rare outcome. 9
Methods
Overview
The analyses below seek to describe the current hospice oversight process and related trends over time (2006–2015), including the accreditation status for hospice agencies nationally, survey deficiency characteristics, survey frequency and outcomes, and traits of agencies that have been terminated from the Medicare hospice program. The analyses merge information about hospice characteristics from Medicare Cost Reports and Provider of Service (POS) files with inspection data from the CMS (see note for more details † ).
Data sources
Medicare cost reports
We use Medicare Cost Reports to obtain information about hospice ownership and chain affiliation. All Medicare-certified hospice agencies must submit Cost Reports on a yearly basis to the CMS, and these data are publicly available. As detailed elsewhere, 13 we have coded each hospice agency nationally over time as for-profit, not-for-profit, or government-owned and as nonchain or chain (i.e., part of a company owning more than one agency). For chain-owned agencies, we have coded the specific chains to which they belong.
POS files
Similar to Medicare Cost Reports, the POS data collection system requires Medicare-certified providers to report data to the CMS. POS files contain administrative information and limited practice data. For these analyses, we incorporated information on hospice agencies' accreditation status (yes/no); accrediting organization, if relevant; and the year the agency was initially certified by Medicare, from which we calculate the “agency age.”
Hospice inspection data
We obtained information on hospice deficiencies and enforcement actions from the CMS. Deficiency information in the 2567 Statement of Deficiencies Reports includes citations from regular surveys and from complaint investigations. Relevant data include the date of each deficiency, the provider against which the deficiency was levied, and the deficiency “tag” identifying the area in which the agency was out of compliance (e.g., in care planning, quality assessment and performance improvement, or patients' rights). We also obtained information from the CMS on the dates and type of all hospice surveys (including surveys that did not result in a deficiency), and on hospice agencies that have been terminated from the Medicare program, including the date of and reason for termination.
Analyses
The analyses focused on four regulatory elements for hospice agencies over the 2006 to 2015 study period: accreditation status, survey deficiencies, survey frequency and outcomes, and termination from the Medicare program. First, we describe the percentage of accredited hospice agencies over time, by ownership status (for-profit and not-for-profit), agency age, and operating chain. Second, we detail the number and type of hospice deficiencies over time. Using the hospice agency-year as the unit of analysis, we also document the percentage of agencies that are surveyed in a given year and the deficiencies that result from these surveys. Finally, we describe hospice agencies that have been terminated involuntarily (or terminated voluntarily due to the potential for an involuntary termination) from the Medicare program since 2006, including their ownership type, accreditation status, and age; their survey deficiency history; and the reason for termination from the program.
Results
Between 2006 and 2015, the proportion of all U.S. hospice agencies with private accreditation increased from 15% to 39%. Accreditation trends differed considerably across for-profit and not-for-profit hospice agencies (Fig. 1). Although a higher proportion of not-for-profit hospice agencies were accredited at the beginning of the study period relative to for-profits (18% vs. 12%, respectively, in 2006), the proportion of not-for-profit accredited agencies grew more slowly over the study period, reaching a peak of 27% in 2011. In contrast, the percentage of accredited for-profit agencies increased considerably over the study period, especially between 2008 and 2015. By 2015, almost half (48%) of for-profit agencies were accredited, compared with only 13% of these agencies in 2008. Rates of private accreditation were highest among smaller for-profit hospices, especially those that were newer to the Medicare program (data not shown). Interestingly, accreditation differed considerably across some of the largest for-profit hospice chains, with companies like Heartland, Aseracare, and Compassionate Care Hospice accrediting almost all their agencies and Kindred/Gentiva, Curo, and Amedisys accrediting relatively few (not shown).
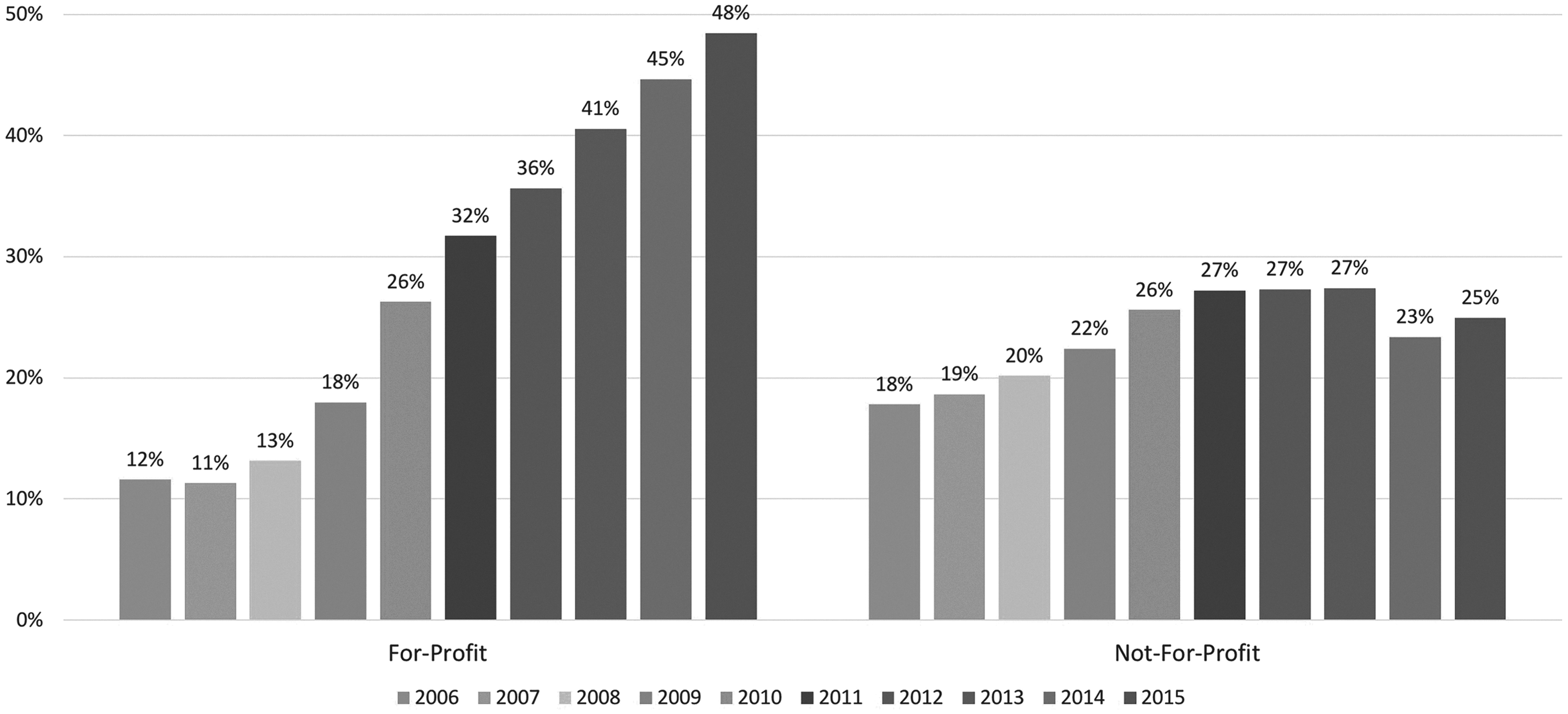
Percentage of accredited agencies by profit status. Data from Cost Reports and Provider of Service files. Accredited agencies were accredited by the Joint Commission, the Community Health Accreditation Program or the Accreditation Commission for Health Care.
Between 2006 and 2015, the combined number of hospice survey and complaint deficiencies increased by 81% (from 3021 to 5456 deficiencies) and increased by 35% on a per-agency basis (from 1.03 to 1.39 deficiencies per agency per year) (Fig. 2). Among the 32,982 deficiencies levied against hospice agencies over the study period (Table 1), the top deficiency categories were care planning (e.g., failing to have an individualized written plan of care for each patient that reflects patient and family goals), 24% of all survey deficiencies; aide and homemaker services (e.g., failing to make a registered nurse visit to the patient's home at least once every 14 days to assess the quality of care and services provided by the hospice aide), 9% of survey deficiencies; clinical records (e.g., failing to have clinical records containing past and current findings for each hospice patient), 9% of survey deficiencies; quality assessment (e.g., failing to develop, implement, and maintain an effective, ongoing, hospice-wide data-driven quality assessment and performance improvement program), 8% of survey deficiencies; and patient assessment (e.g., failing to maintain a drug profile that includes all the patient's prescription and over-the-counter drugs, herbal remedies, and other alternative treatments that could affect drug therapy), 8% of survey deficiencies.
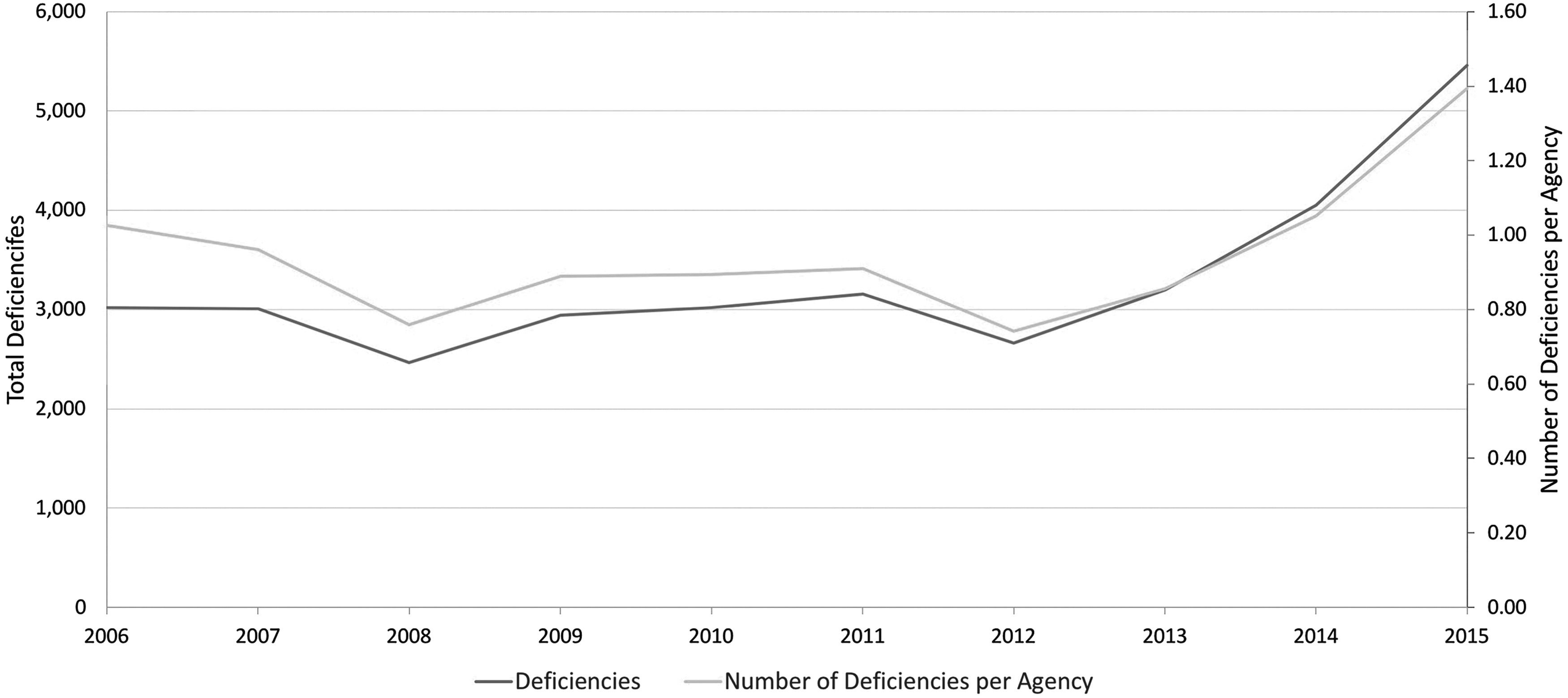
Total deficiencies and number of deficiencies per agency. Deficiency data from Statement of Deficiencies files (CMS form 2567) and include survey and complaint deficiencies. Data include all 50 U.S. states and District of Columbia. One thousand six hundred nine deficiencies dropped because there was a greater than two-year difference between the date recorded in the survey deficiency data and the closest year in the Cost Report data for that provider number. One thousand three hundred eighty deficiencies altered by one year to correspond with the closest Cost Report data. CMS, Centers for Medicare and Medicaid Services.
Total Deficiencies by Type, 2006–2015
Survey deficiency data from Statement of Deficiencies files (CMS form 2567) and include survey and complaint deficiencies. Data include all 50 U.S. states and District of Columbia. One thousand six hundred nine deficiencies dropped because there was a greater than two-year difference between the date recorded in the survey deficiency data and the closest year in the Cost Report data for that provider number. One thousand three hundred eighty deficiencies altered by one year to correspond with the closest Cost Report data.
Deficiencies coded according to the pre-2010 Survey Procedures and Interpretive Guidelines revisions were recoded to match the corresponding current deficiency codes.
Other includes hospices that provide inpatient care directly; licensed professional services; personnel qualifications; nursing services; medical director; short-term inpatient care; compliance with federal, state, and local laws; physical therapy, occupational therapy, and speech–language pathology; and furnishing of noncore services.
CMS, Centers for Medicare and Medicaid Services; SNF/IFC, skilled nursing facility/intermediate care facility.
The percentage of agencies that had a full survey visit in a given year (including initial certifications, recertification, validation surveys [for accredited agencies], full surveys after complaints, and termination surveys) was 23% (Table 2). Focusing on the last five years of data (2011–2015), agencies went around 4 years since their last full survey (4.24 years, data not shown). The percentage of agencies surveyed in a given year generally increased over the study period—from 23% in 2006, dropping to a low of 18% in 2009, and increasing to 38% of all agencies by 2015. Around half of all surveys (45%) resulted in a deficiency citation, a proportion that was relatively steady over the past decade. An average of 3.0 deficiencies was found per survey, and an average of 6.7 deficiencies was cited when deficiencies were found.
Survey Frequency and Deficiency Outcomes, 2006–2015
Agency data from Cost Reports and POS files. Survey data from Statement of Deficiencies files (CMS form 2567). Data include all 50 U.S. states and District of Columbia. One thousand six hundred nine deficiencies dropped because there was a greater than two-year difference between the date recorded in the survey deficiency data and the closest year in the Cost Report data for that provider number. One thousand three hundred eighty deficiencies altered by one year to correspond with the closest Cost Report data.
POS, Provider of Service.
Twenty-eight hospice agencies were terminated from the Medicare program between 2006 and 2015 (Table 3). Of all terminated agencies, 23 (82%) were for-profit and 24 (86%) were unaccredited. Most terminated agencies had a high number of deficiencies in the year of termination (22 on average). Of those agencies that were terminated involuntarily, 10 were terminated due to failure to meet conditions of the provider agreement and 13 were terminated for failing to meet specific health/safety requirements.
Summary of Terminated Providers, 2006–2015
Termination data from the CMS. Terminated providers include providers who were involuntarily terminated or who voluntarily terminated due to a risk of involuntary termination between 2006 and 2015. Four terminated providers were not included because provider number not included in Cost Reports and/or POS files. Termination years were adjusted to correspond to the most recent Cost Report and survey deficiency data. Patient and age data from Cost Reports. Deficiency data from Statement of Deficiencies files (CMS form 2567).
Discussion
Over the last decade, the proportion of privately accredited U.S. hospice agencies increased from 15% to 39%, a trend driven largely by its increased use among for-profit agencies. By 2015, around half of all for-profit and one-quarter of all not-for-profit hospice agencies maintained compliance with Medicare Conditions of Participation through private accrediting organizations. Newer for-profit agencies and select large chains have placed relatively greater emphasis on this approach, perhaps as a mechanism to speed market entry (e.g., if state certification were delayed) or as a market signal to potential referral sources. As discussed below, these trends have implications for hospice quality oversight.
The combined rate of survey and complaint deficiencies per hospice agency increased 35% over the last decade, with issues around care planning, aide and homemaker services, and clinical assessment listed as the most prominent challenges. Over the last decade, around half of all surveys resulted in deficiency citations; yet, less than one-in-four hospice agencies were surveyed in a given year. Of the 28 agencies terminated from the Medicare program over the last decade, most were for-profit agencies and almost all were unaccredited agencies.
Our results offer important context for hospice oversight policy and illuminate at least three key constraints to its effectiveness.
First, the increasing proportion of hospice agencies that are privately accredited necessarily lessens the role of government oversight. Rather than relying on government regulators to verify program compliance, privately accredited hospice agencies are deemed compliant following inspections from CMS-approved accrediting organizations. On its own, this is not necessarily a positive or negative development, as both government agencies and private organizations could either falter or excel in their oversight activities.14–16 Yet, the private accreditation process is, at present, less transparent to the public. Accrediting organizations report information to the CMS about provider inspections, but details of identified deficiencies and plans of correction are generally hidden from public view. An April 2017 proposed CMS rule would have made private accreditation reports available to the public, but the provision was criticized by providers and accrediting organizations and scrapped in the final rule. 17 More recently, in October 2018, CMS announced an initiative to strengthen oversight of accrediting organizations and make limited information about accredited providers' compliance available to the public. 18
Second, quality oversight of hospice agencies arguably has been hampered by its relative infrequency. In a 2013 report, for instance, the Office of the Inspector General noted that 17% of hospice agencies had gone more than 6 years without a full survey. 14 As noted above, passage of the Impact Act in 2014 aimed to address this limitation, requiring that agencies be surveyed at least every three years. Embedded in this strengthened requirement is the expectation that a standardized minimum frequency of hospice inspections will have a beneficial impact on quality of care that outweighs any potential burden of the inspections on providers. It is difficult to see the potential effect of the law in our data, which extend only to 2015. Yet, survey frequency increased over the latter half of the study period, especially in the last year observed. Going forward, it will be important to monitor continued implementation of these standards and their potential impact, especially if the requirement is to be continued past its current legislative sunset in 2025.
A third potential constraint to hospice oversight is the limited availability of enforcement sanctions beyond termination from the Medicare program. Unlike for nursing homes, 19 hospice statutes do not provide for intermediate-level sanctions in instances of noncompliance (e.g., civil monetary penalties, denial of payment for new admissions, and temporary management). 20 If CMS finds violations worthy of citation or determines that an agency is delivering poor quality care, it can request a plan of correction from the hospice agency, but it does not have the option of imposing fines or employing other approaches to remedy the problem. Instead, CMS is limited to the extreme option of license revocation to address quality deficiencies, a solution that was used only 28 times between 2006 and 2015. In its 2018 report on hospice oversight, the Office of the Inspector General recommended that CMS “seek statutory authority to establish additional intermediate remedies for poor hospice performance.” 10 In the context of this effort, it is important to note that there is relatively limited evidence about how effective penalties are in deterring poor quality care and what their optimal level or form might be.
These limitations do not imply that government oversight of hospice care is absent. In fact, hospice regulatory burden has increased in recent years, both as a result of increased concerns about fraud and abuse and because of recent statutory requirements around hospice quality reporting. For instance, reflecting longstanding attention to billing practices and the appropriateness of hospice use from MedPAC, the Office of the Inspector General, and others,21–24 hospice agencies began receiving Program for Evaluating Payment Patterns Electronic Report information in 2012. 25 These data are meant to be used by hospice agencies and the government to monitor potential inaccuracies in Medicare billing and include information about elements, such as live discharge, long hospice stays, and the provision of care in long-term care settings. Similarly, the medical record review and face-to-face recertification requirements triggered by long-stay patients add further scrutiny to ensure appropriate use of the benefit. Despite these efforts to ensure program integrity, however, it is important to emphasize that monitoring billing and enrollment practices and assuring adequate quality of care are distinct exercises.
A more quality-focused government initiative is the ACA-mandated HQRP, which includes clinically focused measures from Hospice Item Set and experience-focused measures from the Hospice Consumer Assessment of Healthcare Providers and Systems (CAHPS). A key product of this effort was the August 2017 launch of the Hospice Compare tool, 26 a website modeled on similar efforts in the nursing home, home health, and hospital sectors. Although implementation challenges have arisen and its utility is somewhat modest in its current form (e.g., most reported measures have limited variability across agencies, limiting the ability to discern higher and lower performance, and the website includes no information about inspection reports or patient complaints),26–28 it has the potential to become a useful tool for referring clinicians and for patients and their families as additional measures are added in the future. Still, even though public reporting can create greater transparency and awareness concerning hospice quality of care, it is not a substitute for quality assurance. Beyond the fact that it is unclear whether and how stakeholders will use this information, public reporting generally does not aim to assess agency compliance with quality standards and has no mechanism for enforcement.
Importantly, considerations for how best to assure hospice quality of care extend beyond the Medicare hospice benefit. In particular, as health care providers and plans seek to expand access to community-based serious illness programs (including palliative care, hospice, and other types of supportive services), creating national standards for certification and ongoing accreditation will be an important part of these endeavors. 29 These activities should be guided by the need to ensure a baseline level of quality among providers and to identify, correct, and (if necessary) sanction instances of poor performance.
Government quality assurance efforts must meet the challenges posed by the way hospice is currently used and delivered. By requiring agency recertification to occur at least once every three years, the IMPACT Act addressed one of the most visible shortcomings in hospice oversight. Our findings highlight two additional changes that could be considered. First, reporting inspection and deficiency information from private as well as public recertification surveys could promote greater transparency and accountability across the hospice sector. Whether through public websites such as Hospice Compare or other sources, these data convey important information and should be broadly accessible to providers and consumers. Second, making a wider range of intermediate sanctions available to oversight agencies could enhance the enforcement of existing standards, offering an alternative to terminating hospice agencies from the program and, ideally, incentivizing them to improve their practices. Ultimately, policymakers, advocates, and providers must continue working together to advance our ability to measure and assure high-quality hospice care for the individuals who use it.
Footnotes
Acknowledgments
We thank Haiden Huskamp and Joan Teno for their comments on a previous draft. This work was funded by the Gordon and Betty Moore Foundation.
Author Disclosure Statement
No competing financial interests exist.