
Abstract
Abstract
There are more adults than children living with congenital heart disease (CHD) due to improvements in surgical and medical CHD management today. In 2011, though, fewer than 30% of adult CHD patients were following up with specialized providers. An ineffective transition from pediatric to adult-focused medical care can result in lapses in CHD medical care, patient noncompliance, and increased risk of late complications. Early involvement of a palliative care team offers development of autonomy, identification of potential barriers to care, and support for patient and family that may improve transition success and quality of life in CHD patients.
Introduction
Currently, there are more than one million adults living with congenital heart disease (CHD) in the United States who must transition from pediatric to adult-focused medical care.1,2 A successful transition leads to effective communication, independent self-care, and informed decision making. 2 However, this transition is often challenging. Fifty percent of parents express apprehension about the transition and struggle with their new role as secondary support. 3 Developmental delays associated with complex CHD, as well as overprotective parenting styles during childhood, also can blunt a child's ability to successfully gain independence.1,4 Challenges with emerging autonomy in the patient–parent relationship lead to ineffective transition, lapses in medical care, and patient noncompliance. 5 Incorporation of a palliative care team offers increased informed decision making and psychosocial support for patients and families that foster successful transitions for CHD patients. 6
Case Description
A 50-year-old male with history of transposition of the great arteries status postchildhood Mustard procedure was followed at an adult CHD clinic. His mother had attended all appointments since childhood. The patient was admitted to both the pediatric and adult hospitals on multiple occasions for acute heart failure exacerbations, as the patient's primary adult CHD subspecialist saw patients at both locations. The patient was found to be noncompliant with his medications during several admissions. At the adult hospital, he underwent evaluation for a left ventricular assist device and heart transplant.
After extensive evaluation, he was deemed ineligible due to repeated episodes of medication noncompliance and psychosocial concerns, in particular, maladaptive coping strategies. On several occasions, the patient had left clinic appointments and hospitalizations abruptly “against medical advice” when the team attempted to address barriers to compliance. He had also dismissed several of his inpatient team providers rather than continuing conversations with the team. The patient became very frustrated with the medical team, and as a result, the patient returned to the pediatric hospital during the next heart failure exacerbation instead of continuing his care at the adult hospital.
The pediatric palliative care (PPC) team was consulted to discuss goals of care and provide support for the patient. Initially, the patient exhibited poor insight about and frustration with his transplant ineligibility. He had difficulty understanding the importance of complying with medical recommendations, as well as why the team would be concerned about noncompliance after receiving a heart transplant. Multiple discussions demonstrated the patient's poor understanding of his illness, a discomfort for asking clarifying questions, and a pattern of choosing to have his mother lead all medical discussions.
Over the course of a weeklong admission, the PPC team helped the patient gain insight about his lack of autonomy and fostered the patient's ability to advocate for himself. Initially, the team used “Go Wish” cards to open conversation about what was important to the patient and his goals for treatment. After the patient felt comfortable expressing these, they began to delve deeper into how his actions of noncompliance did not align with his goal of transplant. Each day, the team met with the patient alone and continued their conversation where it had left off. Over the course of several meetings, he began to trust the team. The patient began to recognize the importance of communicating his needs to the team and expressing when he did not understand a concept. He also realized the effect of medication noncompliance on his transplant status and, for the first time, agreed to regularly take all of his medications. The patient actively participated in the conversations with the PPC team and even acknowledged some responsibility for the adult care team's determination that he was ineligible for a heart transplant. He remained firm that he wanted to continue work on his communication skills with the team and medication compliance. Ultimately, he advocated for a transfer to another institution to continue pursuing transplant.
Discussion
Ninety percent of patients born with CHD are expected to live into adulthood. 5 Although this survival is certainly a success, adults who were born with CHD remain at risk for the development of heart failure, arrhythmias, and recurrent procedures and surgeries. 2 This highlights the importance of receiving consistent health care from childhood through the transition to adult-focused medical care. Nonetheless, studies show that ∼20% of patients with CHD are lost to cardiology follow-up. 7 This lack of regular medical care places the patient at risk for suboptimal preventative care, patient noncompliance, and increased health care utilization. 8
A successful transition to adulthood for patients with CHD requires partnership between a self-advocating and autonomous patient and his or her providers. Adolescents and young adults with CHD must achieve key developmental milestones, including the formation of self-identity, independence, and restructuring patient–parent relationships, all while managing a complex life-limiting illness. 9 This process is especially challenging, as patients with complex CHD have an increased risk for developmental delays related to intelligence, executive functioning, and psychosocial maturity. 4 Further complicating this matter is the potential that the stress of raising a child with a chronic illness may negatively impact parenting styles.1,10 The stress caused by sensing suffering in a child influences how parents interact with their child, and, thus may also affect the child's development. 1 Overprotective parenting styles have been linked to a decrease in the formation of adolescent independence and an increase in heart-focused anxiety in patients with CHD. 11 These effects may impact the patient's self-efficacy, even many years later.
Structured programs, such as Got Transition, associated with The National Alliance to Advance Adolescent Health, with support from Health Resources and Services Administration/Maternal and Child Health Bureau, facilitate the development of autonomy and independence. These programs use a stepwise approach that encourages the development of communication skills, decision making, and self-advocacy. 2 The end goal is to teach adolescents and young adults to become active partners in their care, in contrast to a more familiar pattern over many years of caregiver-driven care and decision making.
A standardized approach integrating palliative care earlier in the transition process could maximize the team's long-term impact and foster a successful transition to adult care. Initially families may be resistant to the option of incorporating palliative care, as many patients often believe, at first, that “palliative care” applies exclusively to those with end-of-life care needs. But introducing the palliative care team using a standardized timeline may normalize the inclusion of palliative care and help patients and families view palliative care as an important and necessary part of managing any chronic illness. Figure 1 shows a suggested timeline for involvement of the PPC team and check points for the transition of health care services for adolescents and young adults with special health care needs as described by Got Transition. 13
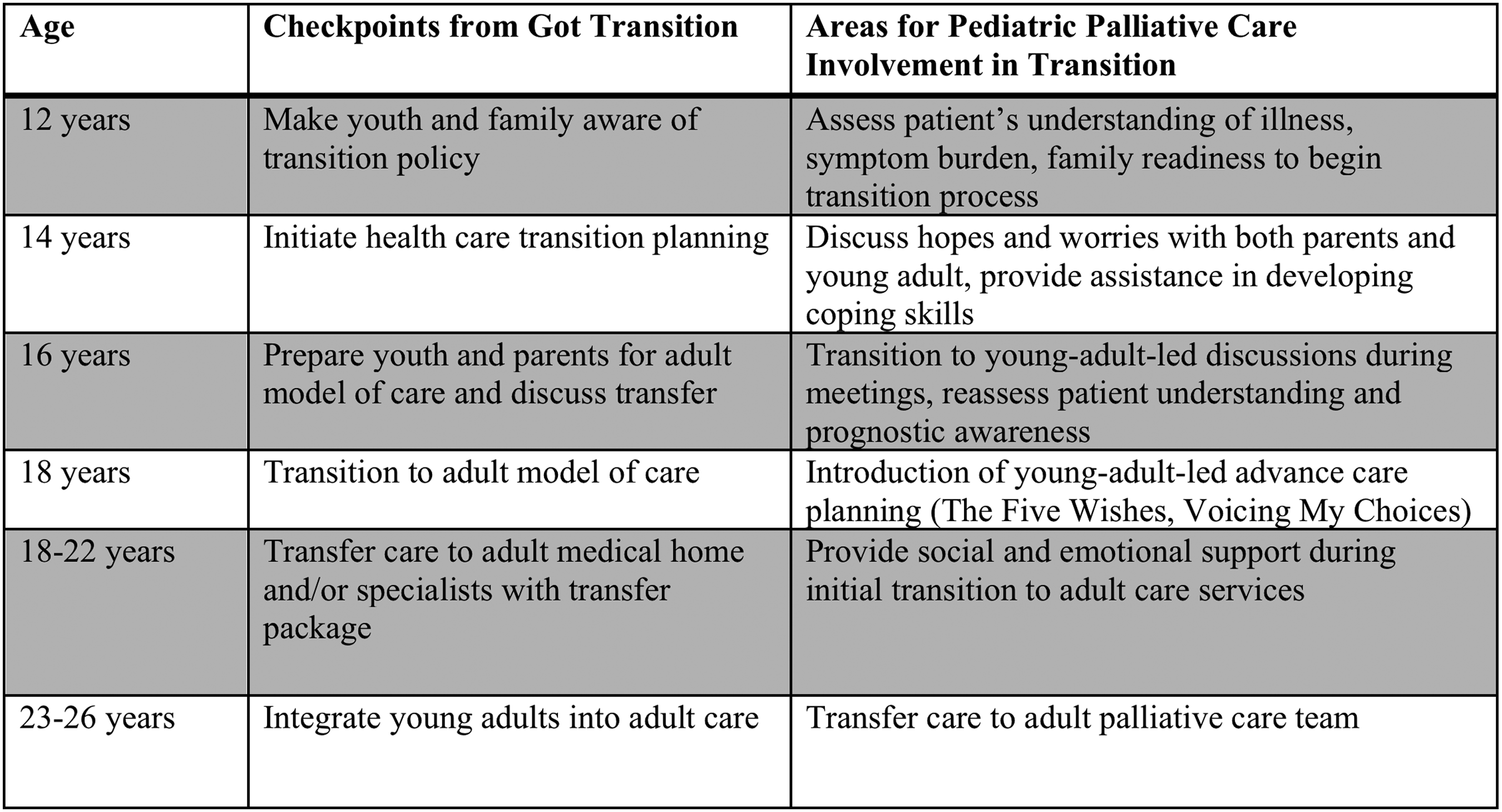
Suggested timeline for transition of health care services for adolescent and young adults with special health care needs as described by Got Transition (a program of The National Alliance to Advance Adolescent Health, with support from HRSA/MCHB), as well as suggested areas for involvement of pediatric palliative care team during transition process. HRSA/MCHB, Health Resources and Services Administration/Maternal and Child Health Bureau.
This model of transitional care does require increased involvement of PPC providers, which may be difficult given limited PPC staffing at many institutions. This challenge can be overcome by ensuring that pediatric subspecialty teams whose patients have high morbidity and mortality risks increase their ability to provide palliative care. Recently, Morrison et al. proposed a new model of palliative care integration in the intensive care unit (ICU) setting. 12 The article recommended all ICU team members maintain a basic “primary” palliative care skill set, including leading conversations about goals of care, assisting families with decisions at the end of life, and symptom management. These “primary” palliative care skills should be obtained in any generalist or subspecialist field and do not require specialized training in palliative care. In addition, a subset of team members have more specialized knowledge of certain palliative care topics, designated “secondary” palliative care. Skills offered by a team member with expertise in “secondary” palliative care may include management of complex ethical issues, advanced or difficult-to-control symptoms, and specialized communication training. Finally, certain patients have more complicated disease courses requiring knowledge of palliative care across many areas and locations in the health care system, from outpatient clinics to inpatient wards and to ICUs. These patients require the consultation of a consultant who has completed subspeciality training in palliative care and offers a “tertiary” palliative care skill set. 12
This model of utilization of tiered skill sets may also apply to the outpatient care setting, specifically in transition medicine clinics. Although this case focuses on patients with adult CHD, the model applies to other adolescent and young adult patient populations with chronic diseases, such as cystic fibrosis, spina bifida, and cerebral palsy. Current health care providers at transition medicine clinics have the “primary” palliative care skills required to initiate and facilitate discussions about symptom management and treatment plans. However, many of these patients with special health care needs require more frequent hospitalizations and have more complicated social dynamics. These multifaceted needs necessitate the skill set of a PPC team, such as the patient described in this case. Therefore, although most visits in a transition medicine clinic may be led exclusively by the primary team, the PPC team should be consulted to meet with the patient and family at each of the transition checkpoint ages listed in Figure 1. This allows for the primary team to remain the principal health care providers throughout the transition augmented at anticipated intervals through the palliative care specialists to best ensure a successful transition and to normalize the early incorporation of palliative care in the management of a chronic illness.
Futures studies are needed to analyze the effects of early incorporation of palliative care into the transition from pediatric to adult-focused medical care. Important outcomes include percentage of appointments attended, compliance with therapies, rates of depression and anxiety, rates of completion of advanced care planning documentation, and, most importantly, quality of life. These outcomes may also be studied by applying this model of PPC involvement to other diseases affecting adolescent and young adult patients, such as cystic fibrosis, cancer, spina bifida, and cerebral palsy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.