
Abstract
Abstract
Context:
Prognosis communication is one hypothesized mechanism by which effective palliative care (PC) promotes preference-concordant treatment near end of life (EOL), but little is known about this relationship.
Methods:
This is a multisite cohort study of 231 hospitalized patients with advanced cancer who consulted with PC. We audio-recorded the initial consultation with the PC team and coded conversations for all statements regarding expectations for how long the patient will live. We refer to these statements as length-of-life talk. We followed patients for up to six months to determine EOL treatment utilization, including hospice enrollment. Patients completed a brief interviewer-facilitated questionnaire at study enrollment.
Results:
Forty-four percent (101/231) of observed conversations contained at least one statement about expectations for length of life, and 60% of patients (139/231) enrolled in hospice during the six months following these conversations. The association between length-of-life talk and hospice enrollment was strong among those (155/231) who endorsed treatment preferences favoring comfort over longevity in the last weeks to months of life (odds ratio [OR]adj = 2.98; 95% confidence interval [CI] = 1.34–6.65) and weak/absent among others (69/231; ORadj = 0.70; 95% CI = 0.16–3.04).
Conclusions:
Talking about expectations for remaining length of life during PC consultations is associated with six-month hospice enrollment among people with advanced cancer who endorse preferences for EOL treatment that favor comfort over longevity.
Introduction
Most people in the United States endorse medical treatment preferences for the last weeks to months of their lives that favor comfort over longevity. 1 Because the default mode in modern medicine is to focus on longevity rather than comfort, it is conceptually important for seriously ill people to have the opportunity to understand how long their clinicians expect that they will live to make informed decisions about the medical treatments they wish to pursue.2,3
Conversations about prognoses, including length of life, are common in specialty palliative care (PC) and hypothesized to be a fundamental mechanism by which PC consultation helps patients to make treatment decisions that comport with their preferences and values.4–12 However, despite the strong conceptual basis and indirect findings, very little is actually known about whether discussing length-of-life expectations are associated with subsequent preference-concordant end-of-life (EOL) treatment in PC. This is an important scientific gap to fill because scaling PC to meet population needs requires us to know which elements contribute meaningfully to the “active ingredients” of our interventions. Here, we contribute to this effort by addressing the following two questions: Is there an association between talking about expectations for length of life during inpatient PC consultations and rates of subsequent six-month hospice enrollment among people with advanced cancer? If so, is this association greater among people who more strongly endorse treatment preferences favoring comfort over longevity in the last weeks to months of their lives?
Methods
Overview
This is an analysis of data arising from the multisite Palliative Care Communication Research Initiative project, 13 a cohort study of inpatient PC consultations among people with advanced cancer. We collected patient questionnaires (including EOL treatment preferences) before the PC consultation, audio-recorded the initial consultation, and followed health utilization and mortality for six months.
Patient participants
The study occurred at the University of Rochester Medical Center and the University of California, San Francisco. Additional details of the study are described elsewhere. 13 All hospitalized patients referred for PC consultation during the study period were eligible for the study if they met the following criteria: diagnosed with metastatic cancer; English-speaking; older than 21 years; able to consent for research or had an established health care proxy who was able to consent. Patients were excluded if they had a “Comfort Measures Only” designation on their Medical Orders for Life Sustaining Treatment form or were already receiving hospice care at the time of referral. Patients' family and friends who were present during the audio-recorded PC consultation provided verbal consent for the audio-recording. No data were collected on family/friends, unless they were the consented health care proxy for patients who lacked such capacity. Patient or health care proxy participants were provided a $20 gift card for participation.
Clinician participants
All PC clinicians at both academic medical centers were invited to participate. PC clinicians included attending and fellow physicians, nurse practitioners, nurses, spiritual care providers, and social workers. Trainees rotating on the PC service were also eligible to participate. A research coordinator met with each clinician to introduce the study. At enrollment, participating clinicians were consented and completed a baseline questionnaire. Enrolled clinicians were offered $100 upon completion of the baseline questionnaire.
Measures
Length-of-life talk
Before entry of the PC team, a research coordinator placed a small digital audio-recorder with a built-in multidirectional microphone in the hospital room and initiated the recording. After the consultation, the research coordinator returned to the hospital room to end the recording and collect the digital audio-recorder. All participants were instructed how to stop recording should they wish; none did so.
We used well-established and reliable methods with which our team has experience to code for the presence and characteristics of prognosis communication.11,14 We defined length-of-life talk to be any prediction or anticipatory guidance about how long the patient would live. We trained two research assistants extensively using a detailed codebook containing precise definitions and examples of prognosis communication. Both research assistants coded a random selection of 20% of the audio-recordings to evaluate interrater reliability.
Other analytic variables
Patient/proxy participants self-reported their gender, educational attainment, and religious affiliations. We measured EOL treatment preferences by asking the extent of agreement or disagreement (five-point Likert scale) with the following modified version of the SUPPORT Study 15 item: “During the last few months of my life, I would prefer a plan of treatment that focused on my comfort and quality of life, even if that meant not living quite as long.” We evaluated financial strain by asking, “When you think about the amount of income that you have available in a typical month, how often is it enough for things you really need like food, clothing, medicine, repairs to the home, and transportation?” [None of the time/Some of the time/Most of the time/All of the time]. We assessed quality of life using the McGill Quality-of-Life Global item: “Considering all parts of your life—physical, emotional, social, spiritual, and financial—over the past two days, how would you rate the quality of your life?” (0–10 scale from “very bad” to “excellent”).16,17 Immediately following the PC consultation, we asked the PC clinician to make their “best guess” about the patients' “most likely survival time, assuming that their illnesses are allowed to take their natural course [<24/24 hours to <2/2 weeks to <3/3 months to <6/>6 months].”
At enrollment, clinician participants completed a baseline questionnaire to report demographic information: age, gender, race/ethnicity, specialization, and professional training and experience.
Analyses
We calculated the frequency and distribution of all study variables. We described the point estimate and 95% confidence intervals (CIs) for the prevalence and features of length-of-life talk among the full sample and stratified by patient characteristics. For statistical significance testing, we used t-tests for normally distributed continuous data and chi-square tests for categorical data.
We evaluated potential effect modification using stratified analyses. We adjusted for potential confounding using both forward and backward multiple logistic regression model building procedures through the iterative inclusion of potential confounders and confounder sets, retaining those with substantial (∼20%) change in the magnitude of the point estimate (i.e., odds ratio [OR] or risk difference). For each association, we identified potential confounders as those variables demonstrating either a theoretical or observed association with the independent and dependent variable.
Human subjects
This study was approved by the protection of human subjects review committees at the University of Rochester Medical Center, the University of California, San Francisco, Purdue University, and the University of Vermont Medical Center.
Results
Approximately half of the patient participants were women; 13% identified as Black or African American and 8% as Latino; two-thirds were <70 years, and 62% were not financially secure. The two most common sites of cancer were the lung (22%) and non-colorectal portions of the gastroenterological tract (18%). Of the 41 PC clinicians who participated, 61% were women (n = 25), 54% were attending physicians (n = 22), 33% were physician fellows (n = 13), and 14% (n = 6) were nurse practitioners. Most (21 of 41) were in PC practice for one to five years, and 20% (8/41) were in PC practice for >10 years (Table 1).
Demographics of Patient Participants by Length-of-Life Talk (n = 231)
EOL, end of life; HS, high school; GI, gastrointestinal; CRC, colorectal cancer.
Forty-four percent (101/231) of initial conversations included at least one statement regarding expectations for the patient's length of life. Among the 101 conversations with some length-of-life talk, statement frequency ranged from 1 to 10 with a count distribution having a mean of 1.1 and standard deviation of 1.7.
As shown in Figure 1 and in Table 2, patients involved in conversations having at least some length-of-life talk compared with others were substantially more likely to enroll in hospice during the follow-up period (OR = 2.16; 95% CI = 1.25–3.73), and controlling for potential confounding by age, sex, cancer type, race/ethnicity, quality of life, Palliative Performance Scale, clinician-estimated survival time, and proxy status did not weaken these findings (ORadj = 2.12; 95% CI = 1.10–4.07).
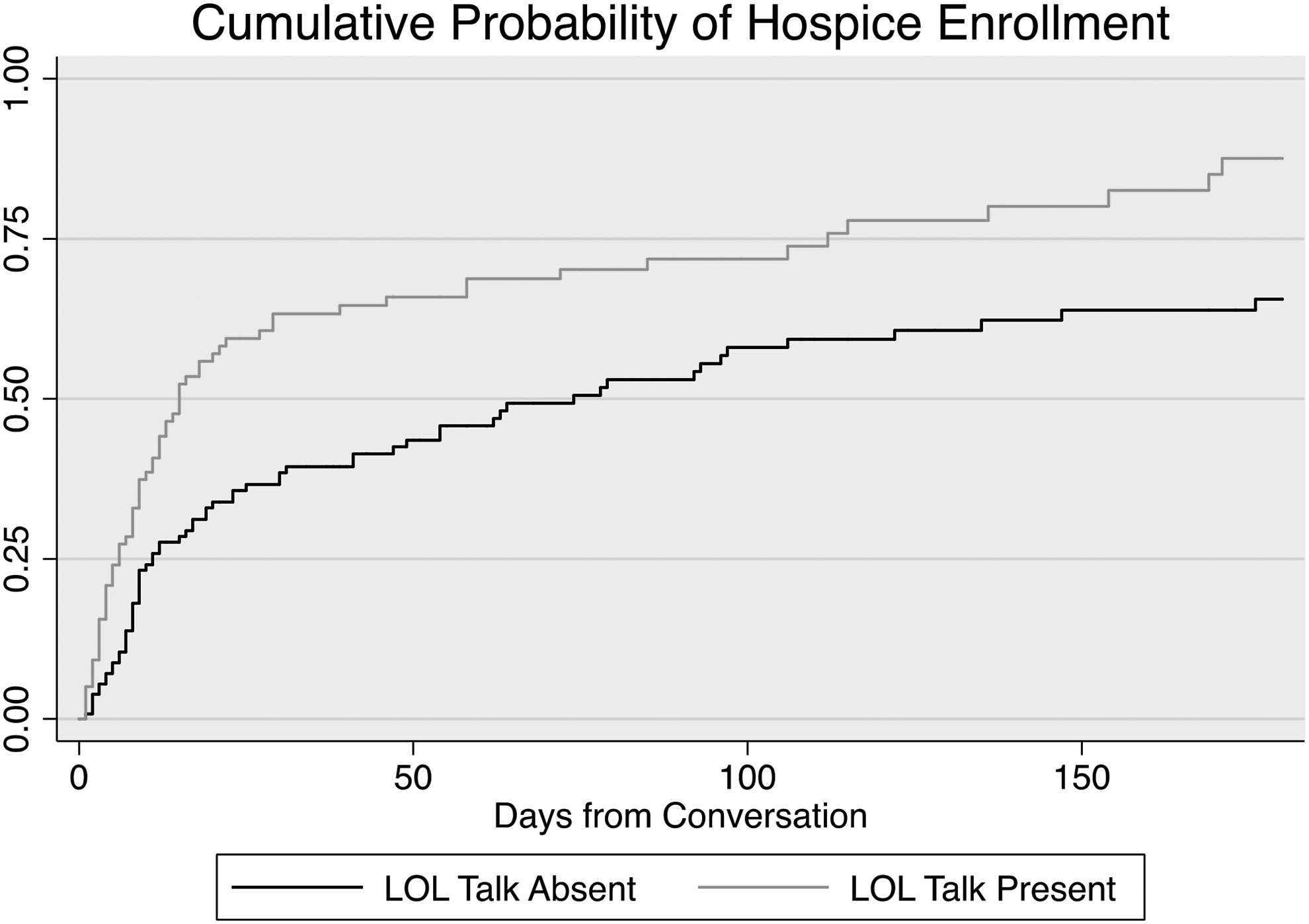
Association between occurrence of length-of-life talk during palliative care consultation and hospice enrollment during the six-month follow-up period. HR for occurrence/timing of hospice enrollment = 1.86; 95% confidence interval = 1.33–2.61. LOL, length of life; HR, hazard ratio.
Association between Length-of-Life Talk and Hospice Enrollment during Six-Month Follow-Up
Adjusted models include age, sex, cancer type, race/ethnicity, quality of life, Palliative Performance Scale, clinician-estimated survival time, and proxy status.
OR, odds ratio; CI, confidence interval.
As shown in Table 3, the association between length-of-life talk and enrollment in hospice showed an important degree of effect measure modification by EOL treatment preferences. The relationship was strong among people who endorsed a preference for treatment in the last weeks to months of life that favored comfort over longevity (ORadj = 2.98; 95% CI = 1.34–6.65) and weak or absent among those not endorsing a comfort-over-longevity tradeoff (ORadj = 0.70; 95% CI = 0.16–3.04).
Effect Modification of the Association between Length-of-Life Talk and Hospice Enrollment by End-of-Life Treatment Preferences
Adjusted models include age, sex, cancer type, race/ethnicity, quality of life, Palliative Performance Scale, clinician-estimated survival time, and proxy status.
Discussion
We evaluated the association between directly-observed length-of-life communication during inpatient PC consultations and subsequent rates of hospice enrollment among people with advanced cancer. We found two important findings that address clinically important gaps in the existing science.
First, we observed that discussing expectations for the patient's remaining length of life during initial PC consultations was substantially associated with hospice enrollment among people with advanced cancer. This direct observation evidence supports what others have observed indirectly. For example, Greer and colleagues have observed that randomized PC consultations resulted in (i) patients' self-ratings of their survival prognosis changing over time to better align with clinical expectations 6 and (ii) less aggressive EOL care.7,8 Hoerger et al. 5 evaluated the association between PC clinician reports about the content of consultations and subsequent EOL treatment among patients with advanced cancer. They observed an association between clinician reports of having discussed treatment decisions or advance care planning (both of which may contain some length-of-life talk) and lower rates of hospitalization and higher rates of hospice enrollment. 5 Our findings provide the first direct observation evidence that prognosis communication is strongly associated with the course of EOL treatment.
Second, preferences for EOL treatment had an important impact on the association between length-of-life talk and hospice enrollment. This interaction is conceptually sound—that people who hold prognosis-sensitive preferences would experience the greatest impact of length-of-life information on choices to enroll in hospice. Interaction in observational studies can lend important insights into whether associations are potentially causal, 18 and we believe that this observation lends stronger support to the hypothesis that prognosis communication is an important causal mechanism underlying the impact on preference-concordant EOL treatment. Preferences are dynamic phenomena, and assessing preference-concordant EOL treatment can be challenging methodologically.19–21 We propose that this conceptually-strong interaction also suggests that EOL treatment preferences reported immediately before PC consultation have a degree of stability that can be useful from a research standpoint for characterizing preference-concordant treatment at EOL.
This study has important limitations. First, this sample includes academic medical center sites in California and New York; inferences about other geographic or institutional sites with substantially different prognostication norms might not be valid. Second, we observed only the initial PC consultation visit. Conversations about EOL decision-making are not single-event phenomena; they evolve over time. Therefore, it is likely that some people with whom length-of-life communication did not happen during the observed visit would have such conversations at a subsequent visit. However, even if this did happen, as we suspect it did for some, we would expect it to bias the association toward the null. This might mean that the timing of such conversations is an indicator of their perceived salience to at least one conversation participant or other marker of decision-making processes. Third, preferences for EOL treatment are dynamic phenomena; it is possible that late or absent enrollment in hospice might represent concordant EOL treatment even among people whose reported EOL preferences at study enrollment would suggest this not to be the case. Other work, however, observes that the typical direction of change in EOL preferences is toward a greater comfort focus rather than away from it. 22 Finally, this is an observational study and precludes strong inferences about causality. Despite the intriguing and suggestive interaction with EOL preferences, reverse causality (i.e., intention to pursue hospice led to communication behaviors supporting discussion about length of life) remains a potential explanation. More research using different methodologies (e.g., randomization or qualitative inquiry) is necessary to confirm our findings.
In summary, we observed that talking about expectations for remaining length of life during PC consultation is strongly associated with rates of hospice enrollment during the subsequent six months. These findings add to the growing empirical literature regarding the fundamental role of prognosis communication underlying the beneficial effects of PC.
Footnotes
Acknowledgment
This work was funded by a Research Scholar Grant from the American Cancer Society (RSG PCSM124655; PI: R.G.). We thank the American Cancer Society and the PC clinicians, patients, and families who participated in this work for their dedication to enhancing care for people with serious illness.
Author Disclosure Statement
No competing financial interests exist.