
Abstract

Dear Editor:
A previous study reported that hospital identification badges using current terminology were a source of confusion among both patients and nurses. 1 As a solution, some multidisciplinary teams wear original badges to easily identify the team members. However, the influence of team badges (TBs) on interactions among coworkers has not been investigated.
The palliative care team (PCT) in our hospital created an original TB in July 2017, and all PCT members have worn this badge on their nameplate. We asked nurses working in our institution for more than one year to answer a questionnaire about the PCT in June and December 2017. We then calculated the number of requests for intervention by the PCT six months before and after the introduction of the TB. A chi-square test was used in the statistical analyses.
A total of 211 and 219 questionnaires out of 260 and 243 were collected in June and December, and 134 (64%) and 147 (67%) nurses had managed patients in palliative care, respectively, with no statistically significant differences in responses between the two questionnaires. The rate of awareness of the presence of a PCT increased from 95% in the first questionnaire to 99% in the second (p = 0.009). Although roles other than doctors, nurses, and pharmacists were less frequently recognized in the first questionnaire, their rate of recognition increased in the second, with significant differences noted in the recognition of medical social workers, rehabilitation staff members, and nutritionists as PCT members in the second (Fig. 1). The total number of requests for intervention by the PCT in the six months before and after the introduction of TBs was 16 and 27, respectively.
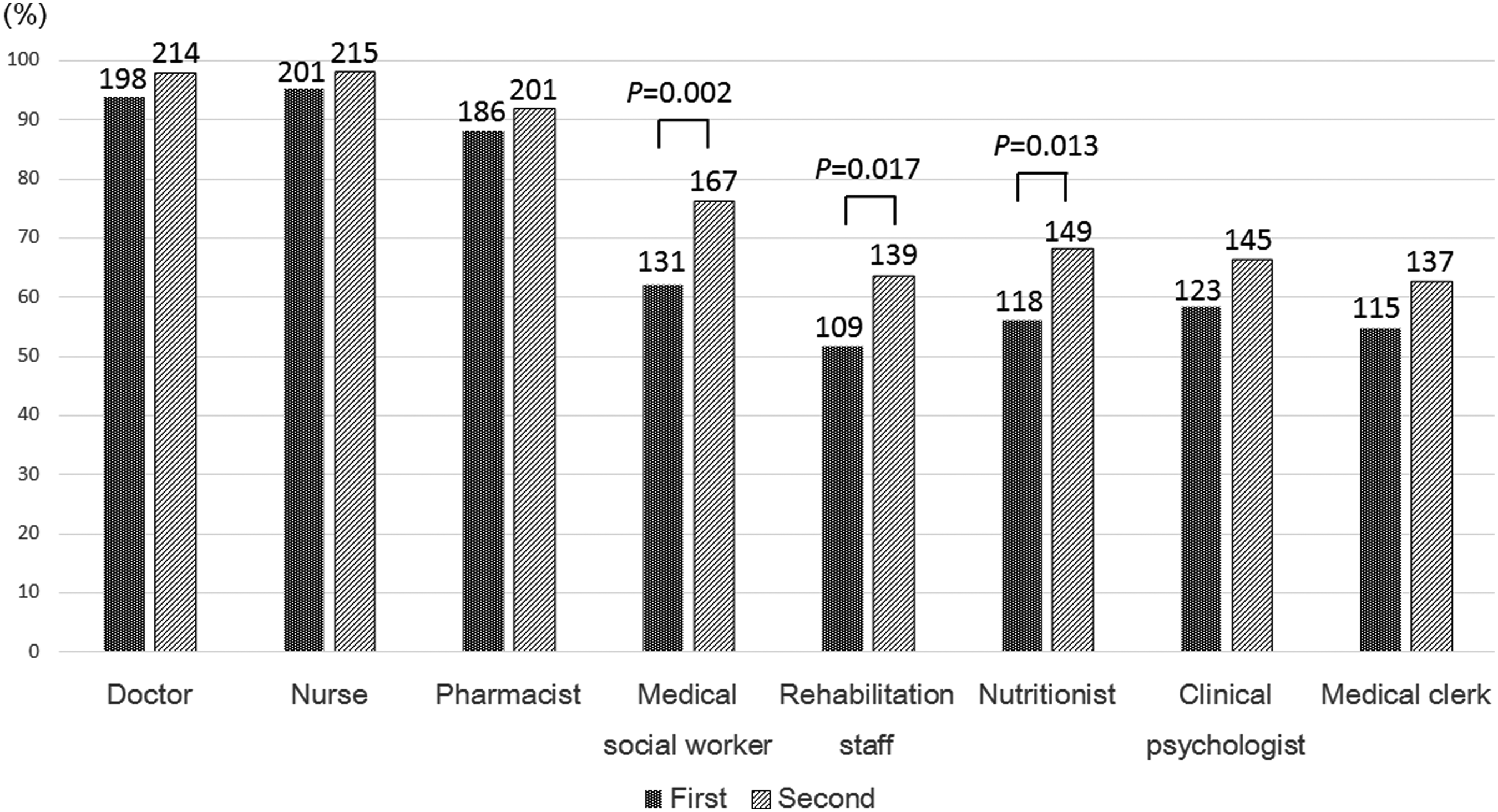
The results of the following question: select the members of the palliative care team (PCT). (Respondents could choose one or several listed occupations.)
Before the introduction of TBs, approximately one-third of nurses were unaware that the PCT was a multioccupational team. Medical staff aside from doctors, nurses, and pharmacists may be less memorable because they have fewer chances to interact with nurses as a PCT member.
However, the results of the second questionnaire showed a significant increase in the recognition of the PCT and its members. There were no changes made to the style of the team activities between the time the two questionnaires were administered, and the number of nurses who had managed palliative care patients had not increased. These findings indicate that the TBs rather than the team activities helped visually facilitate recognition of the PCT and its members. Furthermore, our results suggest that more doctors became interested in palliative care after the introduction of the TBs because the total number of requests for PCT intervention markedly increased. To our knowledge, this is the first study to demonstrate the usefulness of a TB for facilitating not only the recognition of the PCT but also palliative care performance in general.
In conclusion, the recognition of several PCT members, especially paramedics, was not satisfactory among nurses. However, the introduction of a TB for the PCT has facilitated the recognition of the PCT and its members. Furthermore, it promotes requests for team intervention, which enables us to offer high-quality hospitable palliative care to patients.