
Abstract
Abstract
Background:
Therapeutic cannabis is being more widely used by patients to manage multiple symptoms, but the patterns of use in the palliative care population are not well defined.
Objective:
The primary aim of this pilot study was to describe the use of cannabis among patients attending a palliative care clinic (PCC).
Design:
The study was a retrospective chart review of patients seen at four different interval points during 2017 and 2018 in an ambulatory palliative care setting.
Setting/Subjects:
The study was conducted at a 396-bed rural academic medical center in the PCC, where the majority of patients have oncological diseases.
Results:
Clinicians saw 299 unique patients during the four one-month time periods reviewed. Eighty-three patients (27%) reported use of any form of cannabis. The most common reasons for cannabis use were pain (n = 49, 59%), anorexia (n = 16, 19%), insomnia (n = 14, 17%), nausea (n = 13, 16%), anxiety (n = 8, 10%), and depression (n = 5, 6%). Twenty-six patients (31%) used cannabis for more than one symptom. Among the 83 patients using cannabis, 60 (72%) were also prescribed opioids with 32% on immediate-release only and 25% on both immediate- and extended-release opioids. These 60 patients on opioids and cannabis represent 33% of all patients prescribed opioids in this clinic. Tetrahydrocannabinol was present in 25% of the 73 urine drug screens.
Conclusions:
Our data show a significant minority of patients in a PCC use cannabis. Further research should focus on more detailed information about formulation use, methods of ingestion, perceived efficacy, side effects, cost, and standardization of clinical practices. Given the prevalence of cannabis use, further research into its efficacy, side effects, and safety is needed, including whether patients with prior/active substance use receive more or less benefit or harm from cannabis use.
Introduction
Cannabis is increasingly available to palliative care patients in the United States. As of July 2018, 31 states and the District of Columbia had legalized medical cannabis, and 9 of these states and the District of Columbia also legalized recreational cannabis. 1 In 2016, 24 million Americans over the age of 12 were current cannabis users. 2 Medical cannabis became available in New Hampshire in 2016. 3 In Vermont (where half our patients reside) it became available in 2004, and recreational cannabis was legalized in 2018.4,5 For a clinician to certify a patient for therapeutic cannabis, both states require a three-month patient–clinician relationship or diagnosis within the past three months of an approved medical indication. Once certified, patients may purchase cannabis products at one chosen state-licensed dispensary.
Clinicians in our ambulatory palliative care clinic (PCC) noticed increased frequency of questions from patients and family members about cannabis for symptom management. The clinic is part of a rural tertiary care 396-bed academic medical center in Western New Hampshire. The clinic is staffed Monday through Friday with at least one board-certified physician or advance practice nurse and a palliative care social worker (MSW). Clinicians in the PCC do not promote cannabis use, but do support patients who want to try it after considering standard evidence-based therapies. Rarely are patients referred to the clinic specifically for assessment and certification of medical cannabis.
There are limited data on rates of use of cannabis among palliative care patients.6,7 Patients may integrate medical cannabis into their treatment regimens with or without the knowledge or supervision of a clinician. In our PCC, clinicians noted that tetrahydrocannabinol (THC) was being identified in urine drug screens (UDSs), which are routinely done as part of universal precautions for opioid management. This generated an interest in assessing and documenting patient cannabis use.
Methods
The aims of the current study were to (1) assess the use of therapeutic cannabis in our ambulatory palliative care population, (2) describe the reasons patients were utilizing cannabis, and (3) assess for any associations between opioid use and cannabis use in our population.
After obtaining Institutional Review Board approval, a retrospective chart review was conducted for all patients seen in PCC in one month from each quarter for the past year: October 2017 and January, April, and July 2018. The data were deidentified and securely stored in Research Electronic Data Capture (REDCap, Nashville, Tennessee). Descriptive statistics were calculated using Microsoft Excel.
Manually extracted data included patient demographics; cannabis use: medical or recreational; indication (i.e., which symptom); and, if available, formulation, dosage, and frequency of use. If a patient was seen multiple times, only the first visit was included in the study, unless a patient's cannabis use status changed, in which case two visits were included. For example, if a patient was not using cannabis in October 2017 but was using cannabis when re-evaluated in January 2018, both of the patient's charts were included in data analysis. Twelve visits were included in this manner.
Results
Clinicians saw 299 unique patients during the four months reviewed. The majority of patients had cancer. There was a fairly even distribution of men and women with a median age of 65 years (range 22–97). The patients' residences were evenly distributed between New Hampshire and Vermont. Fifty-eight percent of patients were on opioid therapy (Table 1). Eighty-three patients (27%) reported use of any form of cannabis, 114 (37%) reported no cannabis use, and 114 (37%) were not assessed for cannabis use. In the 197 patients assessed for cannabis use, 83 (42%) reported some form of use. Seventy-four patients reported using cannabis for medical purposes only, five reported only recreational use, and four reported both medical and recreational use. Of the 228 patients who did not use any form of cannabis at baseline, 9 (4%) were subsequently noted to use some form during the chart review period. Two patients (1%) who had reported cannabis use discontinued use.
Demographics (N = 311)
ER, extended release; IR, immediate release.
The most common reasons for cannabis use were pain (n = 49, 59%), anorexia (n = 16, 19%), insomnia (n = 14, 17%), nausea (n = 13, 16%), anxiety (n = 8, 10%), and depression (n = 5, 6%). Five patients reported cannabis use for alertness, concentration, mood, bladder spasms, or seizures (Fig. 1). Twenty-six patients (31%) used cannabis for more than one symptom. Our numbers are too small for statistical comparison between months, but pain remained the predominant indication for cannabis use across all months. Among the 83 patients using cannabis, 60 (72%) were also prescribed opioids with 32% on immediate-release only and 25% on both immediate- and extended-release opioids. These 60 patients on opioids and cannabis represent 33% of all patient prescribed opioids in this clinic. In the documented UDSs (n = 73), 25% (n = 18) had THC present.
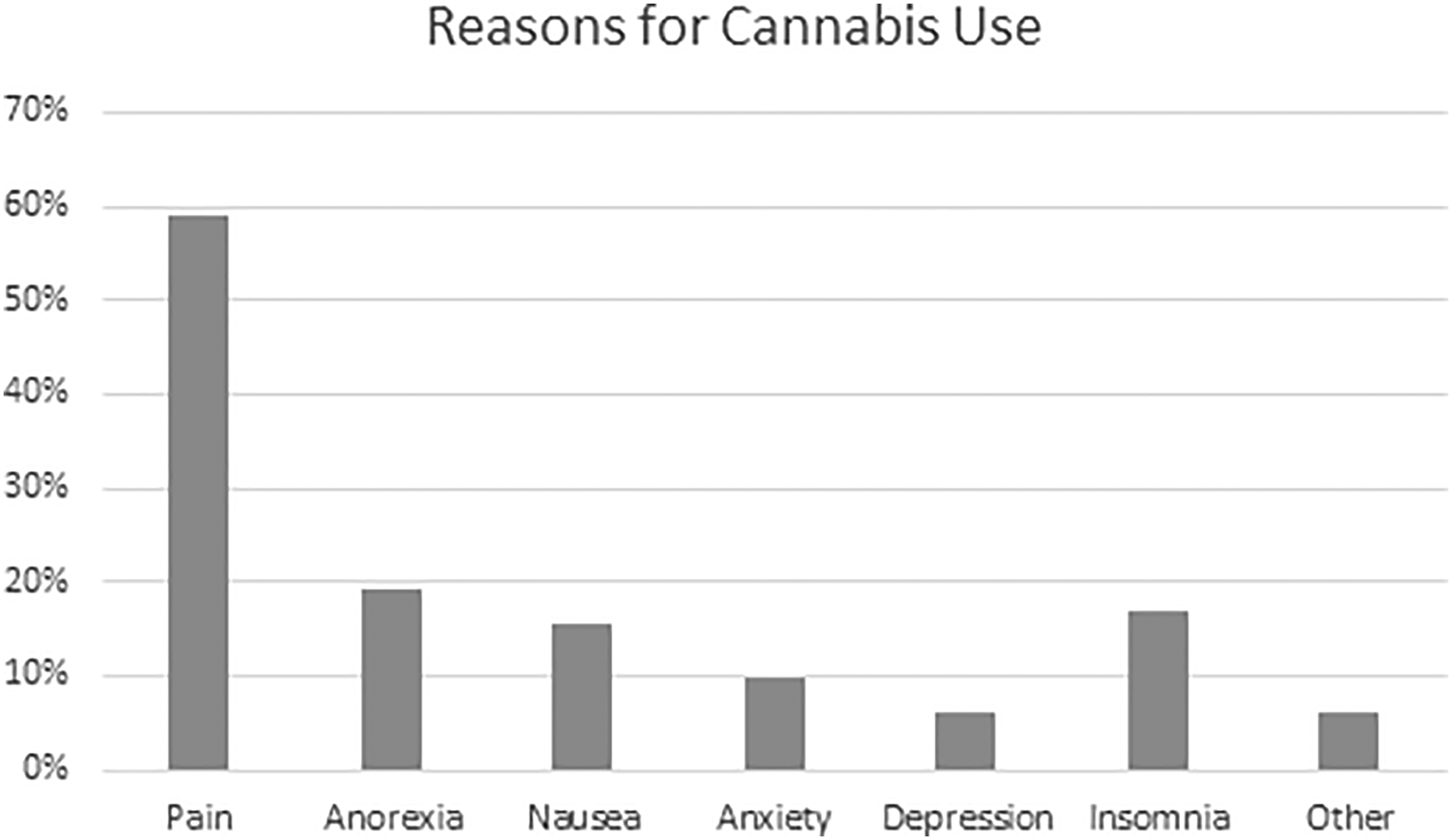
Percentage of cannabis users reporting use by symptom. Patients could report use for multiple symptoms.
Discussion
More than one-quarter of patients in this PCC report using cannabis for symptom management. Many patients use cannabis for more than one symptom, including physical and neuropsychiatric symptoms. Most patients using cannabis are also prescribed opioids. One-third of all patients prescribed opioids were also using cannabis. These rates are higher than those reported in some other studies. Rauenzahn et al. report 13% of cancer patients in a supportive care clinic had cannabis in their UDSs, although the decision to check a UDS was based on clinician assessment rather than a universal precautions approach to opioid prescribing. 6 Pergam et al. surveyed patients in a large cancer center in Washington state finding that 24% of patients reported active cannabis use, with 14% of UDSs being positive, consistent with 18% of respondents reporting at least weekly cannabis use. 7
Our patients' higher rates of cannabis use may be understood in part in the context of a high regional prevalence of opioid use disorder (OUD) (35.8 opioid-related overdose deaths per 100,000 in New Hampshire in 2016; 18.4 per 100,000 in Vermont; national average 13.3 per 100,000).8,9 Cannabis may (1) pose less harm to family acquaintances who have OUD, (2) be perceived as safer, (3) carry less stigma, or (4) be used in the hope of minimizing opioid use. Patients for whom pain is managed by our PCC tend to have more complicated or difficult to manage pain syndromes, which may increase their desire for alternative pain management options. They may prefer a symptom management option that is minimally regulated and thus easier to obtain and manage on their own. Some referrals are for pain management in the setting of concern for a substance use disorder, which may select a patient population more likely to use cannabis.
In our study, rates of patient-reported cannabis use are consistent with UDS data, adding internal validity. Our results are similar to those reported by Pergam et al., 7 adding external validity. Since our clinicians routinely assess opioid and cannabis use, the data reflect current patient use, compared with other studies that assess general use. It is unusual for patients to be referred to our clinic specifically for certification of medical cannabis. Thus, the prevalence in our setting is likely more representative of the general palliative care population compared with a clinic where patients are referred explicitly for medical cannabis certification. However, cannabis use in our clinic population may not be generalizable to clinics with fewer patients with cancer or in regions with lower rates of OUD. Because all patients were not routinely asked about recreational cannabis use, and one-third of all patients were not asked about any cannabis use, these data likely miss patients using cannabis; thus, the actual number of patients utilizing cannabis is most likely higher than reported. In this descriptive study, it was not possible to follow specific patients or assess changes among individual patients over time. Although the reason for cannabis use was documented as part of symptom assessment, the formulation, content, or frequency of use was not routinely documented.
Our study demonstrates that a substantial proportion of palliative care patients may use cannabis for symptom management, often without medical oversight. Palliative clinicians may be unaware of patient use, which may lead to misattribution of symptoms, underdiagnosis of disorders masked by cannabis use, and missed opportunities for counseling to reduce potential adverse side effects. For these reasons, routine screening of palliative care patients for cannabis use could improve patient care.
Further research should focus on the effectiveness of cannabis for symptom management and adverse effects. Understanding the effects of cannabis on opioid use or quality of life in the population of patient with symptoms related to cancer or treatments may lead to better symptom control. Finally, it will be important to assess whether patients with prior/active substance use or mood disorders are more or less likely to utilize cannabis and benefit from or be harmed by use.
Footnotes
Author Disclosure Statement
No competing financial interests exist.