
Abstract
Abstract
Objective:
Delays in specialized palliative care (PC) consultation in end-stage liver disease (ESLD) patients may be explained by clinician attitudes toward PC. Our aim is to assess the attitudes of hepatology and liver transplant (HLT) and PC clinicians toward PC consultation and consultant roles in ESLD patient care.
Methods:
Clinician members of HLT and PC professional societies were surveyed. Using a five-point Likert scale, they rated their comfort level toward various PC consultant roles and their agreement with triggers for and reasons to defer PC consultation. Change in attitudes toward PC consultation resulting from liver transplant (LT) eligibility was evaluated.
Results:
A total of 311 HLT (6.2%) and 379 PC (8.1%) clinicians completed the survey. The vast majority of HLT clinicians (>80%) were comfortable if PC consultants palliate symptoms, provide support, or facilitate advance care planning in LT-ineligible patients. LT eligibility reduced HLT clinician comfort toward all PC consultant roles, except supportive care. A vast majority of PC clinicians (>90%) were comfortable assuming all PC roles, except pain management without opioids (43–51%). About 80% of HLT clinicians agree with PC consultation in LT-ineligible patients with decompensated cirrhosis or hepatocellular carcinoma (HCC), compared to 20–30% if LT ineligible. Common justifications for deferring PC consultation included mild disease, LT eligibility, unavailability of PC specialists, and lack of addressable palliative issues.
Conclusions:
Barriers to specialized PC consultation in ESLD include HLT clinician discomfort with PC consultant roles, patients' LT eligibility, perception that PC is end-of-life care, unclear triggers for PC consultation, and concern about opioid-based pain palliation.
Introduction
End-stage liver disease (ESLD) is defined by the onset of ascites, variceal bleeding, hepatic encephalopathy (HE), or jaundice in patients with cirrhosis. Without liver transplantation (LT), ESLD is a terminal illness that has a 60% one-year mortality rate.1,2 ESLD patients suffer from poor quality of life (QOL), pain and other physical symptoms, psychological distress, functional impairment, and financial hardship.3–6 Caregivers are heavily stressed and, occasionally, give up employment and educational plans due to heavy care demands.3,7,8
Palliative care (PC) is a holistic approach that addresses physical, psychosocial, and spiritual needs of seriously ill patients. 9 Often erroneously equated with end-of-life (EOL) care or hospice,10,11 PC is appropriate at all stages of serious illness, even alongside life-prolonging interventions. Over the years, specialized PC consultation teams have proliferated across the United States to aid clinicians in managing symptoms, communicating with patients and caregivers, providing support, and advance care planning (ACP).12,13 ACP explores patient values and goals and identifies surrogate decision makers and EOL care preferences. 14
Early involvement of specialized PC teams for patients with advanced cancer improves patient QOL, care satisfaction, physical symptoms, and, possibly, survival.15–17 There are data that integrating PC visits with LT evaluation reduces patients' physical and emotional symptoms and increases advance directive completion rates. 18 However, despite the recognition of PC as a quality care indicator in ESLD, 19 many ESLD patients are still referred to specialized PC teams or hospice and have goals of care (GOC) discussions near the time of death or, sometimes, not at all.20–22
Infrequent and late utilization of specialized PC teams in ESLD patients has been attributed to patients' LT eligibility, ESLD's unpredictable disease trajectory, clinicians' inaccurate perceptions of PC, absence of clear referral criteria, and clinicians' discomfort with EOL discussions.23–25 Similar to others' experience with heart failure, 26 lack of clarity on the PC consultant's role may dissuade hepatology and LT (HLT) clinicians from referring ESLD patients to specialized PC teams. HLT clinicians' discomfort with palliative interventions that the PC consultant may provide is another potential deterrent to PC consultation. In this article, we surveyed HLT and PC clinicians' level of comfort toward potential roles of the PC consultant in ESLD patient care. PC clinicians were also surveyed because they should also feel comfortable rendering palliative services to ESLD patients. We secondarily evaluated clinicians' attitudes toward possible triggers for and barriers to PC consultation in ESLD. Understanding HLT and PC clinicians' views on PC in ESLD may help guide efforts to enhance PC delivery to this patient population.
Methodology
Survey population
Members of the American Association for the Study of Liver Diseases (AASLD) and the American Academy of Hospice and Palliative Medicine (AAHPM) were invited to participate in the survey. AASLD members were contacted using e-mail addresses available through the association's online member directory. The AAHPM e-mailed its members internally after the academy's research committee approved the study protocol.
Survey instrument
The Medical College of Wisconsin IRB (PRO00026625) approved the study. Potential participants were invited by e-mail to participate in an anonymous web-based survey (SurveyMonkey, Palo Alto, CA). The survey accepted responses for 15 days, and reminder e-mails were sent at 5, 10, and 15 days. Survey participation was not compensated. Informed consent was waived.
Survey questions were developed from a review of relevant literature and author experience. Authors are specialist physicians in PC (S.M.) and Gastroenterology and Hepatology (J.E., K.S.). Two similar surveys were developed, each with 79 questions, and designed to be completed in less than 10 minutes. One survey was distributed to AASLD members and was worded from the perspective of a clinician obtaining PC consultation, while the other was distributed to AAHPM members and was worded from the perspective of the PC specialist being consulted.
Personal identifiable information was not collected. Respondents were asked about their clinician category, primary field of practice, practice location and setting, patient population, and years in practice. Using a five-point Likert scale, respondents rated their level of comfort with palliative services that consulted specialized PC teams may provide for ESLD patients. Included palliative services covered pain and nonpain symptom palliation, management of portal hypertensive (PH) complications, supportive care, and ACP. Respondents gave separate ratings according to patients' LT eligibility. Respondents rated their agreement with potential triggers for specialized PC consultation and the rationality of justifications for deferring consultation. Surveys can be found in Supplementary Tables S1 and S2.
Analysis
Only completed surveys from respondents providing clinical care were analyzed. For study purposes, AASLD and AAHPM respondents were assumed as HLT and PC clinicians, respectively. To assess nonresponder bias, given low response rates, respondents were compared to nonrespondents using descriptors provided by AASLD and AAHPM. Wave analyses were performed. Baseline characteristics and mean Likert ratings to representative questions of respondent “wave” groups that followed each e-mail blast were compared using Cochran–Armitage and Jonckheere–Terpstra tests for categorical and ordinal variables, respectively. Wave analysis assumes that later wave groups are increasingly more similar to nonrespondents. 27 Frequency distributions of responses to each question were obtained and compared between HLT and PC groups using chi-square. Respondent level of comfort to each PC consultant role and level of agreement with decompensated cirrhosis and HCC as triggers for PC consultation for LT-eligible and LT-ineligible patients were compared using McNemar's test. Statistical significance was defined as p < 0.05. Statistical analyses were performed using Stata v14.1 (StataCorp, College Station, TX).
Results
Respondent characteristics
Survey response rates were 6.2% (n = 311/5009) for AASLD and 8.1% (n = 379/4678) for AAHPM. Baseline characteristics of respondents are shown in Table 1. AASLD respondents and nonrespondents had similar characteristics, whereas AAHPM respondents were more likely to be PC-board certified, U.S. based, or hospital based (Supplementary Tables S3 and S4). On wave analysis, AASLD wave groups had similar baseline characteristics, while later waves of AAHPM respondents were more likely to be trainees and located outside United States or Canada. AASLD and AAHPM wave groups answered representative questions similarly (Supplementary Tables S5 and S6).
Baseline Characteristics of Hepatology and Liver Transplant and Hospice and Palliative Care (HPC) Clinicians
AAHPM, American Academy of Hospice and Palliative Medicine; HLT, hepatology and liver transplant; HPC, hospice and palliative care.
Clinician comfort toward PC consultant roles–LT-eligible patients
Ninety-three percent of HLT clinicians were comfortable if PC consultants provide psychologic and emotional support to LT-eligible ESLD patients, and 70–80% were comfortable if PC consultants discuss EOL preferences and GOC, provide hospice care, document advance directives, provide medical decision-making support, and palliate nonpain symptoms in this patient population. HLT clinicians were less comfortable if PC specialists palliate PH complications (29–43%), manage pain with unrestricted opioids (51%), and discuss prognosis (47%). More than 90% of PC clinicians felt comfortable discussing EOL preferences and GOC; providing psychologic, emotional, and medical decision-making support; documenting advance directives; palliating pain (unrestricted opioids) and nonpain symptoms; providing hospice care; and discussing prognosis in LT-eligible patients. Around 70% of PC clinicians felt comfortable palliating PH complications, but only 43% were comfortable if asked to avoid opioids for pain management. Compared to PC clinicians, HLT clinicians were less comfortable with all palliative roles in LT-eligible patients, except for provision of psychologic and emotional support, where both groups were similarly comfortable (Fig. 1A).
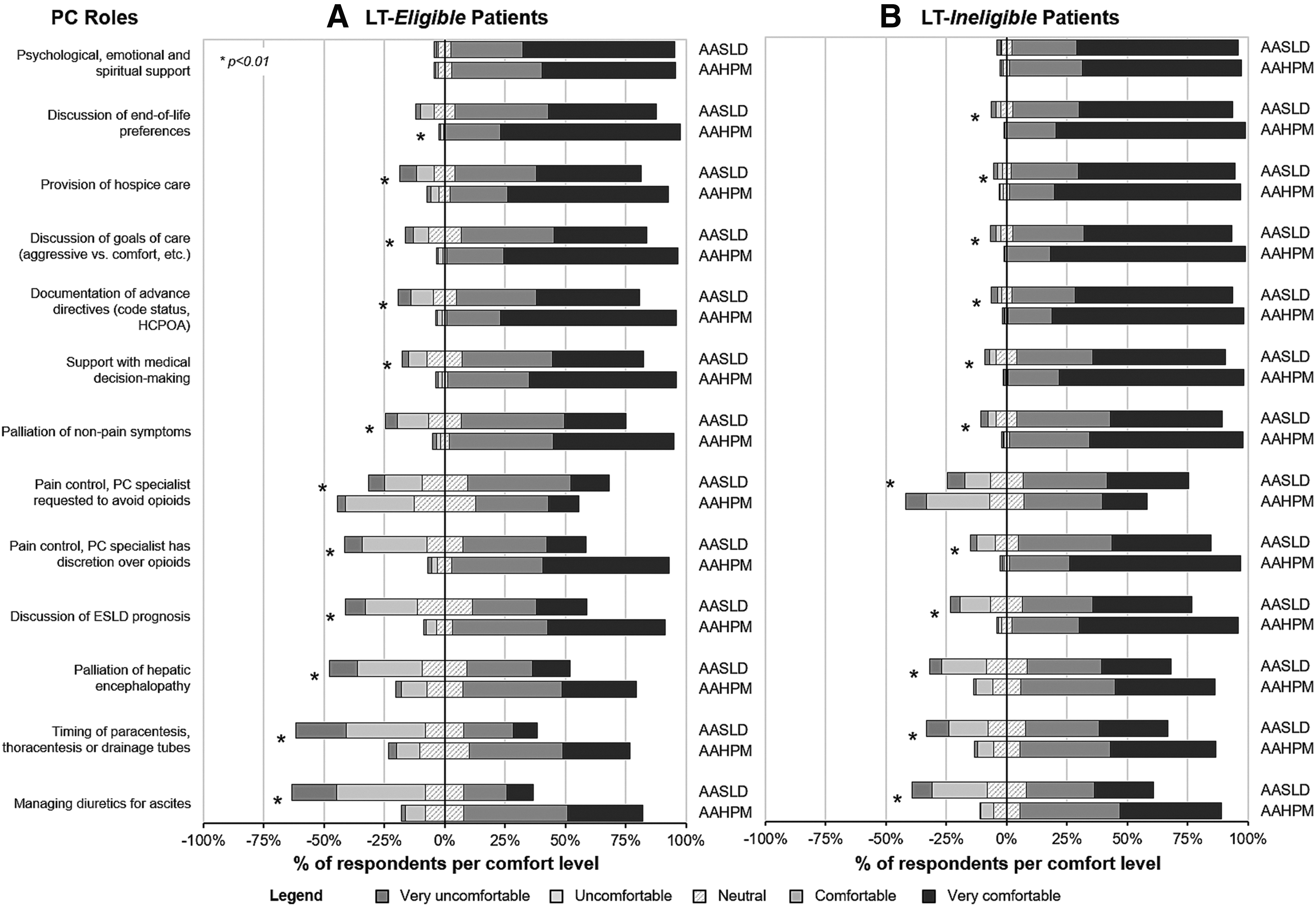
Comfort level among HLT and PC clinicians toward provision of various palliative services to ESLD patients who are
Clinician comfort toward PC consultant roles–LT-ineligible patients
In LT-ineligible ESLD patients, >90% of HLT clinicians were comfortable if PC consultants provide psychologic and emotional support, provide hospice care, document advance directives, and discuss GOC and EOL preferences, and 80–90% were comfortable if PC consultants provide medical decision-making support and palliate pain (unrestricted opioids) and nonpain symptoms. HLT clinicians were less comfortable if PC consultants palliate PH complications (53–60%) or discuss prognosis (70%) and if opioids are restricted than if allowed (69% vs. 80%) in pain control. More than 95% of PC clinicians were comfortable palliating pain (unrestricted opioids) and nonpain symptoms, providing supportive care, and facilitating several aspects of ACP in LT-ineligible patients. About 80% of PC clinicians were comfortable managing PH complications, but only 51% felt comfortable if asked to limit opioid use in pain control. HLT clinicians were less comfortable with all palliative roles in LT-ineligible patients compared to PC clinicians, except for provision of psychologic and emotional support (Fig. 1B).
Change in clinician comfort toward PC consultant roles following LT eligibility
The possibility of LT changed comfort levels from “comfortable”/“neutral” to “uncomfortable” in <10% of HLT clinicians for supportive care, GOC discussion, and pain palliation with restricted opioids; 10–20% for palliation of HE and nonpain symptoms, documentation of advanced directives, disease prognostication, and provision of hospice care; and in >20% for management of ascites and pain palliation with unrestricted opioids. LT eligibility caused discomfort in <6% of PC clinicians. However, PC clinicians appeared more comfortable if asked to avoid opioid-based analgesia (Fig. 2).
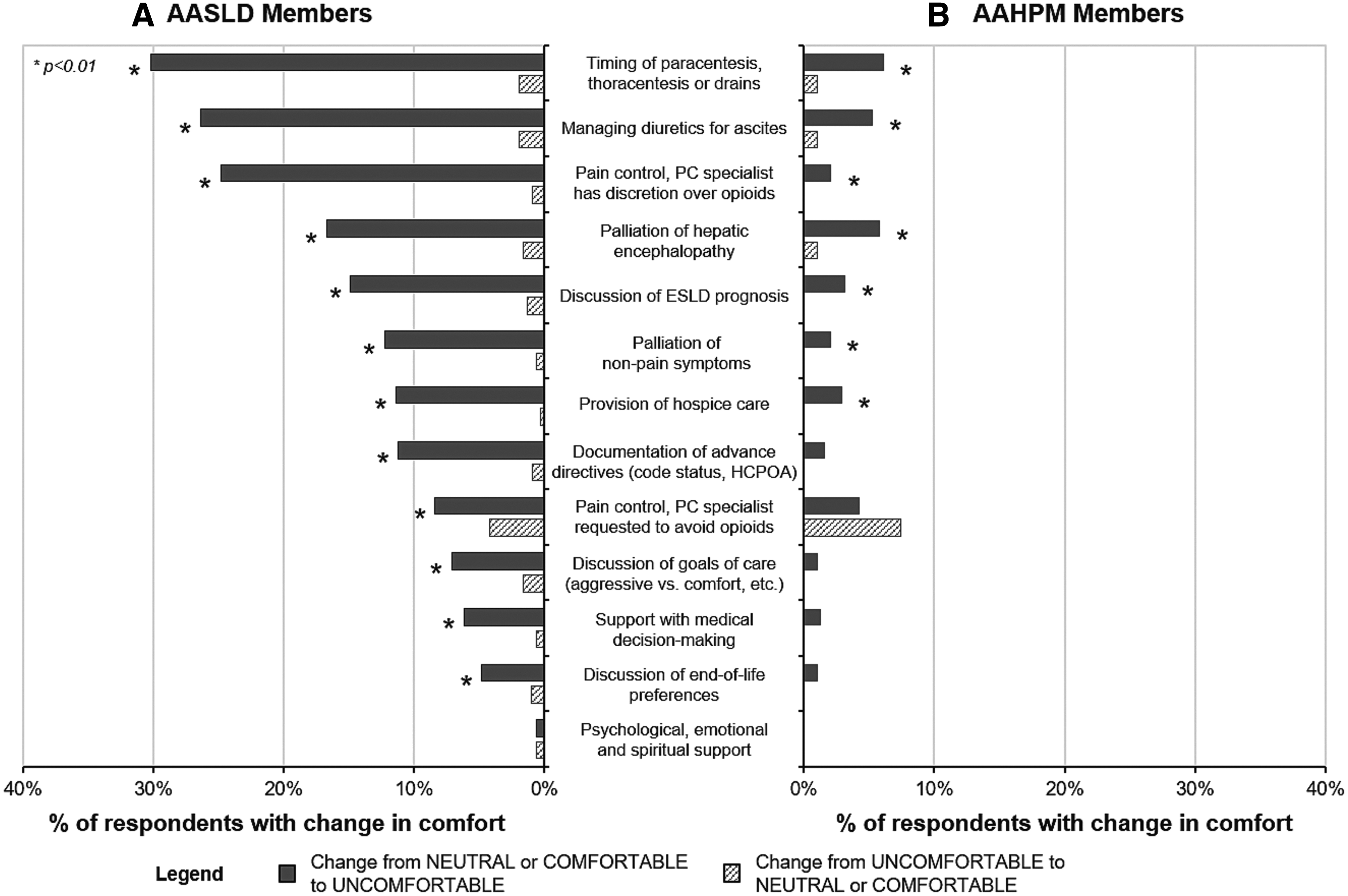
Change in comfort level among
Triggers for PC consultation
About 80% of HLT clinicians and >90% of PC clinicians agreed that LT-ineligible patients with decompensated cirrhosis or HCC should be referred to specialized PC teams. However, only 20–30% of HLT clinicians, compared to 75–85% of PC clinicians, agreed to PC consultation in LT-eligible patients. The possibility of LT in decompensated cirrhosis or HCC changed clinician response from “agree”/“neutral” to “disagree” in 37% and 48% of HLT clinicians, respectively, but in <5% of PC clinicians. Only 9% of HLT clinicians agreed that all cirrhotics, irrespective of compensation, should be referred to PC specialists. HLT and PC clinicians are less likely to agree with specialized PC consultation in Childs-Turcotte-Pugh (CTP) class C than class A (HLT: CTPA 5% vs. CTPC 58%; PC: CTPA 29% vs. CTPC 91%). Ninety-four percent of PC clinicians, compared to only 56% of HLT clinicians, agreed with PC consultation if subjective estimated life expectancy is less than one year. HLT clinicians were less likely than PC clinicians to agree with each referral trigger. Model for end-stage liver disease (MELD) scores considered by >50% of respondents as appropriate thresholds for PC consultation were ≥25 for HLT clinicians and ≥19 for PC clinicians. However, 31% and 21% of HLT and PC clinicians, respectively, did not specify MELD score referral thresholds (Fig. 3A–C).

Reasons for deferring PC consultation
Mild disease and nonimminent death, LT eligibility, lack of addressable palliative issues, possible patient demotivation following PC consultation, hospice noncandidacy, and unavailability of PC specialists were cited by 41–73% of HLT clinicians as reasonable justifications to defer specialized PC consultation. Only 21–31% of HLT clinicians cited personal discomfort with EOL discussions, unclear PC specialist roles, their ability to address their patients' needs on their own, potential opioid use, and inability to predict death as reasonable justifications to defer specialized PC consultation. About 40% of PC clinicians cite the ability of HLT clinicians to address their patients' needs on their own and lack of addressable palliative issues as reasonable justifications to defer specialized PC consultation. PC clinicians thought that most other cited justifications were unreasonable. HLT clinicians were more likely than PC clinicians to consider most justifications as reasonable, but less likely to consider their ability to independently address PC issues as a reasonable justification (Fig. 4).
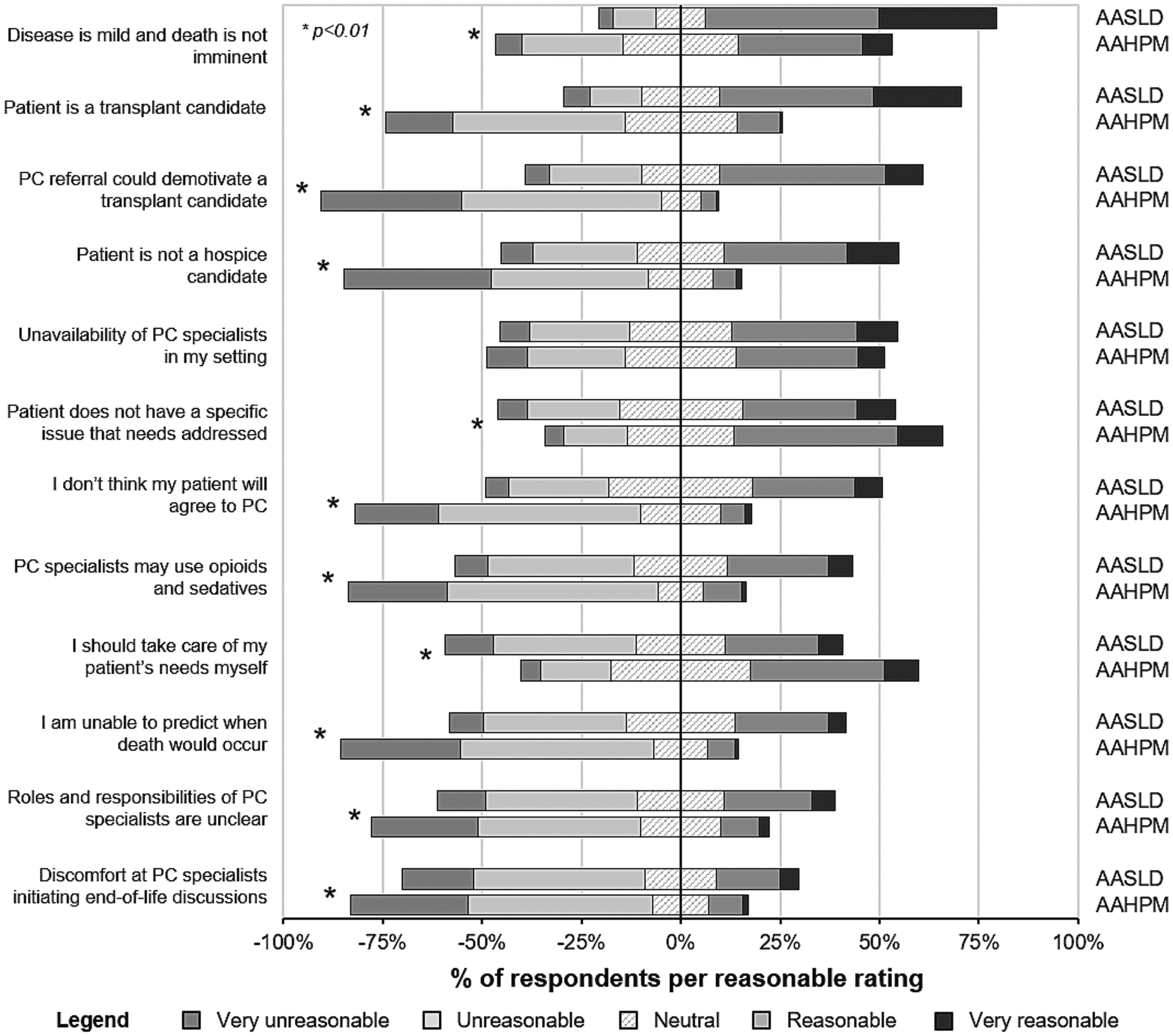
Rationality of justifications for deferring specialized PC consultation among HLT and HPC clinicians.
Discussion
Specialized PC consultation remains underutilized in ESLD despite its potential benefits. Survey findings suggest five potential barriers to PC consultation among ESLD patients.
Variable comfort level toward PC consultant roles
HLT clinicians have variable comfort levels toward different palliative services that PC consultants may provide ESLD patients. HLT clinicians feel comfortable with many palliative roles, including ACP and supportive care. However, discomfort in other roles, such as managing PH complications, discussing patients' prognosis, and opioid-based pain palliation, may be enough to discourage them from referring ESLD patients to specialized PC teams. It is surprising that discussing prognosis elicited relative discomfort considering HLT clinicians' comfort with other ACP components. HLT clinicians likely feel that they are responsible for this role, PC specialists lack a nuanced understanding of ESLD's illness trajectory, or patients will lose hope when they hear their prognosis.
PC consultants should recognize and take into consideration HLT clinicians' potential discomfort with palliative services. Consulting PC specialists should remember that, although patient well-being is their primary focus, the referring physician remains as the client and primary stakeholder. 28 Although PC clinicians appear comfortable providing virtually all palliative services, they should make a point to clarify the scope of their involvement with referring HLT clinicians at the beginning of the collaboration and throughout the course of the patient's illness. Doing so may encourage earlier and more frequent PC referrals from HLT clinicians. Up to 30% of surveyed HLT clinicians may defer PC consultation due to lack of clarity in PC specialists' roles.
Considering clinician comfort with palliative services, a potential model of early concurrent PC in ESLD will have PC specialists provide supportive care and, in LT-ineligible patients, ACP and nonpain palliation, while HLT clinicians discuss prognosis and manage PH complications. HLT clinicians are not as clearly comfortable with pain palliation and ACP in LT-eligible patients. However, PC consultants should attempt to obtain HLT clinicians' support in providing these services by increasing awareness of how these services benefit patients.
LT eligibility
Survey findings suggest that clinician discomfort with palliative services and concern for patient demotivation potentially contribute to the difficulty in providing palliative services to LT-eligible patients. Data from advanced cancer patients do not support the fear that discussing prognosis or EOL issues with patients diminishes hope or increases their risk for depression or anxiety.29,30 Nevertheless, discussing EOL issues with LT-eligible patients remains challenging because LT offers the possibility of long-term survival. Given their experience navigating delicate EOL conversations, specialized PC teams can assist in this daunting task. Surprisingly, only 20% of surveyed HLT clinicians would defer PC consultation because of discomfort with PC specialist-led discussions on EOL issues. However, the question did not distinguish between LT-eligible and -ineligible patients.
LT-eligible patients can benefit from specialized PC consultation. ACP is particularly beneficial by ensuring that patients don't receive unwanted care, given ESLD's unpredictable course and possible loss of decision-making capacity from HE. Moreover, listed patients, fearing removal from the waitlist, may feel obligated to comply with all treatment recommendations, even those inconsistent with their values. 31 Prognosis awareness is important because patients may be removed from the waitlist or die before transplantation or from transplant-related complications.32,33 Listed patients also suffer from poor QOL, psychological distress, and existential distress,34–36 which may improve with PC interventions. PC and LT are not mutually exclusive. Baumann et al. reduced symptom burden and increased advance directive completion rates by integrating outpatient PC consultations with LT evaluation visits. 18 Amazingly, Medici et al. successfully listed and transplanted a number of patients enrolled in hospice. 37
Inaccurate perception that PC is EOL care
“Mild disease” and “hospice non-candidacy” were commonly cited by HLT clinicians as reasonable justifications to defer PC consultation, indicating that PC is still erroneously equated with EOL care. Because clinicians tend to overestimate actual patient survival, 38 equating PC with EOL care increases the likelihood that patients will receive palliative interventions close to death, which diminishes PC's potential benefits. In the early stages of serious illness, PC consultants can manage incapacitating symptoms, provide additional support, and help patients understand their illness.
Unclear triggers for appropriate PC consultation
In the absence of consensus referral criteria for PC in ESLD patients, timing of PC consultation is likely determined by HLT clinicians' attitudes toward PC. Clinician attitudinal barriers to PC consultation may be mitigated by defining referral triggers that are easy-to-identify, based on illness severity, and systematically implementable. 39 Clinical triggers that obtained the agreement of >50% of surveyed HLT and PC clinicians may be reasonable referral criteria and include subjective estimated life expectancy less than one year, CTP class C, and LT-ineligible cases of HCC and decompensated cirrhosis. A third of surveyed HLT clinicians did not provide a threshold MELD score for PC consultation; although in >50% of those who did, MELD >25 seemed an appropriate referral trigger. While only 20–30% of surveyed HLT clinicians agree with PC consultation in LT-eligible patients with HCC and decompensated cirrhosis, PC consultation should still be considered in these patients.
Concern about opioid-based pain palliation
Survey findings highlight HLT clinicians' apprehension toward opioid-based pain palliation in ESLD patients. While opioids are invariably effective analgesics, their use raises concerns of worsening HE, substance abuse, or alcohol recidivism in ESLD patients. 40 However, ESLD patients can experience pain comparable to advanced cancer, severely diminishing QOL. 3 Opioids have been safely used in liver failure with conservative dosing and close follow-up. 41 To our knowledge, no study has associated opioid use with alcohol recidivism in pre- and post-LT settings. Understandably, PC clinicians are uncomfortable with imposed restrictions on their practice. Dialog between HLT and PC clinicians addressing opioid-related concerns is essential in strengthening their collaboration and, importantly, improving patient well-being.
Study limitations
First, ESLD patient and caregiver attitudes toward PC were not evaluated. Patient and caregiver reluctance to engage PC specialists—potentially from negative perceptions of PC, lack of symptoms, or fear of delisting—is a frequently cited barrier to PC consultation.10,14,42–44 Second, low response rates predispose to nonresponse bias. However, sample-to-population comparisons and wave analysis suggest that HLT and PC clinician respondents are likely representative of their respective professional societies. Despite low response rates, overall respondent numbers remain sizable, and, to our knowledge, this is the largest survey of clinician attitudes toward PC in the ESLD population. Third, respondents may overestimate their comfort with PC consultation due to its perceived desirability (response bias). Fourth, real-world utilization patterns of specialized PC teams for ESLD patients were not evaluated. Findings also reflect the practices of individual respondents and do not apply to all clinicians. Nevertheless, the study provides insights into clinician attitudes that potentially influence medical decision making, which can guide strategies to improve PC utilization in ESLD. Fifth, the survey was not designed to measure HLT clinicians' comfort level with providing palliative services independently. If HLT clinicians provide basic symptom management, supportive care, and ACP, then PC consultation may reasonably be reserved for complex issues.13,45 Routine PC consultations without specific palliative needs are minimally beneficial to patients. 46
In conclusion, the study highlighted the following five potential barriers to specialized PC consultation for ESLD patients: HLT clinician discomfort with PC consultant roles, LT eligibility, inaccurate perception of PC, unclear triggers for PC consultation, and concern about opioid-based pain palliation. These factors should be considered in strategies to improve PC delivery to ESLD patients. Convening a task force of HLT and PC leaders may help identify the optimal collaborative model that addresses the unmet palliative needs of ESLD patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.