
Abstract
Abstract
Background:
Cancer-related physical symptoms can decrease patients' overall quality of life and are often underdiagnosed. The Edmonton Symptom Assessment Scale (ESAS) is widely used in palliative care for cancer patients to easily assess cancer patients' symptoms. It has been often modified, adding symptoms and explanations, and translated into many languages. The European Association of Palliative Care research team developed a database, which included the modified 12-item ESAS-r as the symptom assessment tool.
Objectives:
The purpose of this study was to achieve the translation and cross-cultural validation in French of the 12-item ESAS-r, the ESAS12-F.
Design:
A French version of the ESAS-r was developed using a standardized forward and backward translation method. Patients completed the ESAS12-F and provided feedback on the translation.
Setting/Subjects:
Forty-five patients with advanced cancer, followed by the palliative care team from the Lyon Sud University Hospital in France, were recruited.
Results:
Eighty-nine percent of patients considered the ESAS easy to understand. They highlighted some concerns more about the tool itself than the translation: the time line “now,” the difficulty to quantify a symptom in a numerical evaluation. Some items (sleep and appetite) needed to be reread and for some others (digestive and psychological symptoms, and well-being) to be reordered in the questionnaire.
Conclusion:
The ESAS12-F is well accepted and easy to use for the cancer patients. The next step is to carry out a psychometric validation of the definitive version of the ESAS12-F.
Introduction
The distress reported by patients facing cancer is strongly associated with their physical symptoms. 1 In a survey of 4600 cancer patients, respondents reported an average of five physical symptoms. 2 Earlier symptom management could improve quality of life.3,4 Assessment of physical symptoms improves patient satisfaction with care and clinical response. 5 Cancer-related physical symptoms can decrease patients' autonomy and overall quality of life6,7 and are often underdiagnosed and undertreated due to lack of knowledge and poor assessment.1,8–10 Patients are more likely to underreport their symptoms during a clinical interview than when assessment tools are used.6,11 To minimize the burden on oncology patients, the tool should be brief and manageable, easy to administrate and analyze, reliable and valid, and must also identify important symptoms.12–14
The Edmonton Symptom Assessment Scale (ESAS), with nine common symptoms, is widely used in palliative care for cancer patients.15,16 A good correlation has been shown between ESAS and the Brief Pain Inventory (BPI), and the Rotterdam Symptom Checklist, with weighted kappas between 0.46 and 0.61. 17 The ESAS (9 items) has good internal reliability (Cronbach's α 0.79), test–retest reliability (Spearman correlation coefficient 0.86 on day 2 and 0.45 on day 7), and convergent validity (correlation coefficient 0.85 with Functional Assessment of Cancer Therapy (FACT) pain, 0.83 with Memorial Symptom Assessment Scale (MSAS) pain, and 0.56 with BPI worst pain). 16
This tool has been modified many times to include more symptoms, and translated into many languages, including French but not in a French population.18–26 In response to concerns regarding the interpretation of some of the items, a revised version of the ESAS, the ESAS-r, has also been developed adding few explanations for some items. 27 A pilot study of the French translation of the ESAS-r was conducted with French-speaking Canadian patients, while a French translation of the ESAS involved French-speaking Swiss patients.28–30 Moreover, the European Association of Palliative Care (EAPC) research team is developing a “European palliative care patients” database, which includes the modified 12-item ESAS as the symptom assessment tool.23,31 This modified ESAS has not been translated and validated in French.
The purpose of this study was to achieve the translation and cross-cultural validation of the modified 12-item ESAS-r, the ESAS12-F, including content and face validation, with a French cancer population followed by a palliative care team.
Materials and Methods
Design
This is a prospective study of cancer patients followed by the palliative care team at Lyon Sud University Hospital, France.
Sample
The patients were recruited from the palliative care unit (PCU), the palliative care inpatient clinic, and the palliative care outpatient clinic. Patients older than 18 years, with French as their mother tongue diagnosed with advanced cancer, followed by the palliative care team, and without cognitive impairment, were included in the study. Participants were excluded if they lacked sufficient French literacy to complete the study questionnaires.
Forty-five patients were included. The sample size for this study was based on previous studies, 32 as well as general guidelines on conducting qualitative research.33,34
Measures
Edmonton Symptom Assessment Scale
The ESAS tested in this study is a modified 12-item ESAS, validated by Hannon et al. and used in the EAPC database.23,31 Items assessed are as follows: pain, tiredness, drowsiness, nausea, vomiting, constipation, appetite, shortness of breath, anxiety, depression, sleep, and well-being, on a numerical rating scale (NRS) ranging from 0 (not at all or no symptom) to 10 (worst possible symptom). The time period to assess the patients' symptoms was defined by “now.”
Translation protocol
The translation and cultural validation process followed a standardized forward and backward translation protocol to determine the conceptual, semantic, and operational equivalence.35–37 A rigorous multistep structure was applied for reviewing, revising, and drafting of the final translation.
After requesting the authors' permission to use the 12-item ESAS questionnaire, the translation was carried out according to the European Organization for Research and Treatment of Cancer (EORTC) standardized forward/backward translation procedure. 38 First, the ESAS was translated from English into French by two native French translators, independently of one another. After finding and examining the differences in the way it was interpreted and translated, these two initial translations were combined into a provisional version. This provisional version was then translated from French back into English by an English speaker. The steering committee compared this last English version with the original, to find the best French version. This second version was then tested on patients to obtain the final version of the ESAS12-F (Fig. 1).
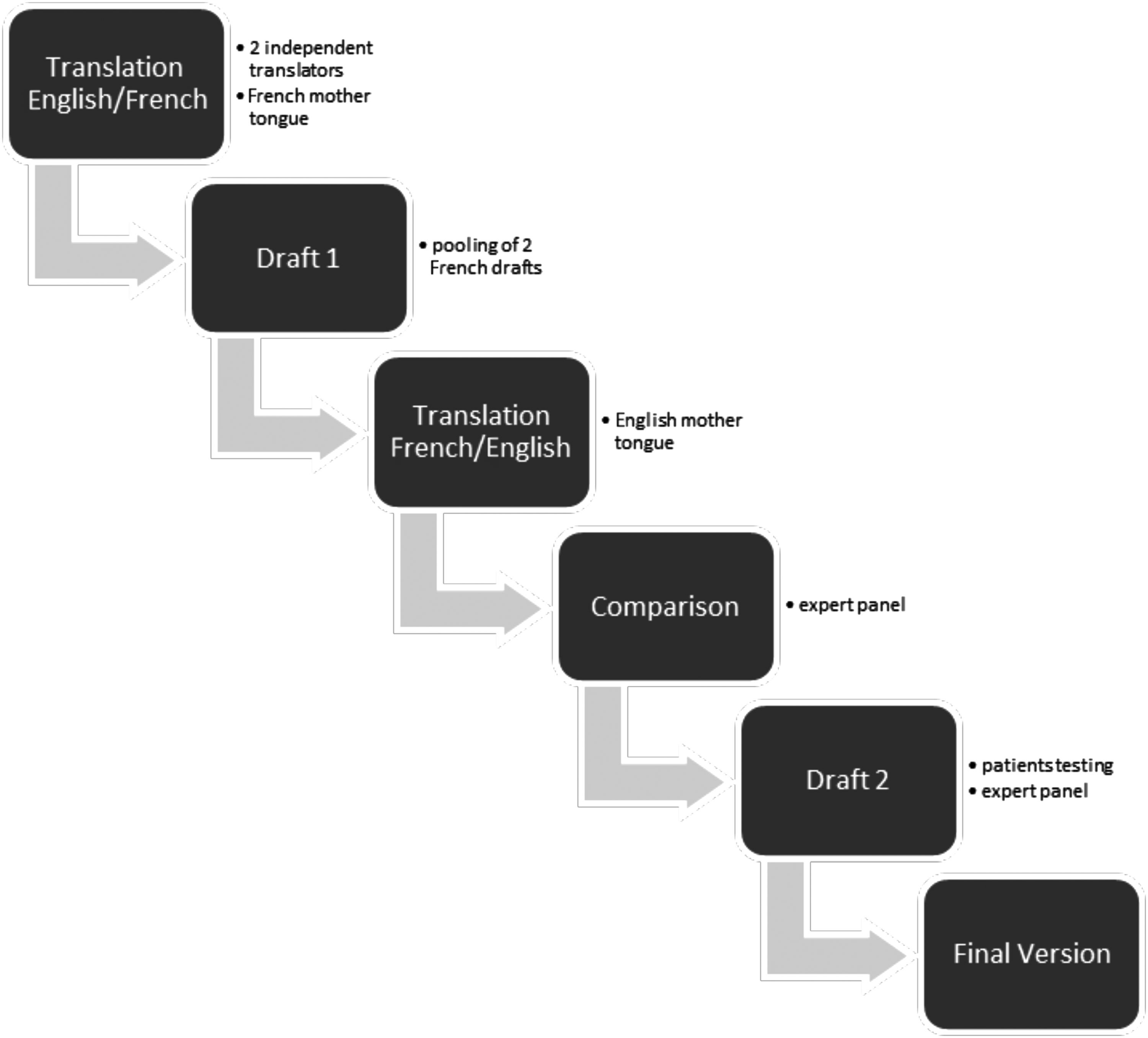
Translation protocol.
Demographic data
Participant sociodemographic and clinical characteristics were collected from self-report and medical chart by the interviewer: the patients' age, gender, marital status, level of education, diagnosis, time since initial diagnosis, cancer stage, location of metastases, current cancer treatment, previous treatment, Karnofsky performance scale, and cognitive status.
Study questionnaire
Each patient was asked to fill out ESAS12-F, for each item, to answer questions regarding his/her comprehension of the item, comprehension of the instructions, if it was difficult to respond to the question (yes/no), if the latter was unclear, annoying, or upsetting, and whether the various options were suitable responses to the question asked (yes/no). The patient also had the opportunity to comment on the instructions for filling out the scale, and his/her comprehension of the scale itself, and to make any general comments. The patients completed the ESAS and the questionnaire in the presence of a research assistant who transcribed the comments from the patients.
Data analysis
All data were anonymized. Responses were transcripted using Word and Excel, version office 2010.
Descriptive statistics (frequencies, means [M], and standard deviations [SD]) were used to analyze the data.
Ethics
Ethical approval of the study protocol was obtained from the Sud-Est IV ethics committee and board review by our institution.
Results
Population demographics and characteristics
This study involved 45 patients: 15 in the PCU, 15 in the palliative care inpatient clinic, and 15 in the palliative care outpatient clinic between August 2015 and January 2016 (Table 1).
Participant Characteristics (N = 45)
SD, standard deviation.
Forty percent of the population were male, the median age was 63 years (M = 62, SD 12), 69% were in a relationship, and 75% were educated to high school and upper level. The three most common types of cancer diagnoses were breast and gynecological cancer (29%), hematological (20%), and gastrointestinal (18%). Eighty-two percent had metastatic cancer, 62% were undergoing chemotherapy, and 20% no specific cancer treatment. Fifty-six percent had bone metastases. Opioids were the most prescribed treatment (73%). The median on the Karnofsky performance scale was 70% (M = 64, SD 17).
Descriptive statistics (median, mean, SD, frequencies) for the symptoms are summarized in Table 2. Based on the median scores, the symptoms tiredness, worse well-being, and lack of appetite had the highest symptom burden scores. Pain (96%) and fatigue (93%) were the most frequent symptoms; and vomiting (13%) had the lowest frequency.
Descriptive Statistics (Median, Mean, Standard Deviation, Frequencies) of Edmonton Symptom Assessment Scale (N = 45)
Content validity
Comprehension
The majority of patients (89%) considered the items in the ESAS easy to understand (Table 3).
Content Validity, Acceptability, and Comments of Patients (Verbatim) (N = 45)
ESAS, Edmonton Symptom Assessment Scale.
However, there was a tendency to interpret items regarding appetite and sleep in the opposite way from that intended: the less intense the symptom, the higher the number. Certain patients had to reread these particular items to give an accurate response to the question.
Patients' comments on each item are summarized in Table 3.
Response modality and acceptability
Eleven percent of patients had difficulty responding to the questions, and 2% found the questions unclear, annoying, or upsetting; and patients found 91% of the numeric scale tool appropriate. The ESAS12-F has a good acceptability as only one data is missing: 0.2% of the questionnaire.
Time taken to fill in
The mean time taken to fill in the questionnaire was 10 minutes (minimum 1 minute, maximum 30 minutes, SD 7), which patients considered acceptable.
Face validity
Patients generally reported that the symptom tool was clear and comprehensible. They reported that it was suitable for assessing the general state of their health and the main symptoms causing them distress. Ninety-eight percent of patients agreed that the instructions were clear.
However, they highlighted certain difficulties:
The fact that symptoms rated as “now” are assessed, as they often reported a large fluctuation in symptoms over time, and would have preferred an “on average” response. The difficulty to quantify a symptom in numerical form on a wide range (0–10). Some patients would have preferred to be able to respond “yes” or “no,” or with a verbal scale “good, average,…” or on a smaller numerical scale than the one provided. The need for certain items (sleep and appetite) to be reread to properly understand the meaning of the responses to the item. The need to review the order of certain items in the questionnaire to be more logical: gathered digestive issues together, grouped psychological issues, and ended by well-being as a summary of the assessment.
Based on these comments and recommendations, a final French version, the ESAS12-F, was created (Annex 1).
Finale Version of the ESAS12-F
Discussion
Through this study, we were able to carry out a transcultural adaptation of the 12-item ESAS with a French population. The results demonstrate very good levels of comprehension and acceptability for the scale.
The population study is comparable with the population cared for in palliative care by our team. 39
Transcultural validation
For most symptoms, no difficulties arose when translating into French. However, certain terms or turns of phrase had to be modified, and explanations added to items, to improve comprehension. The term “worst” (le pire) in the original translation thus became “maximum” (maximal) to improve comprehension.
The order of the items was changed: digestive problems (constipation, nausea, and vomiting) grouped together and psychological problems (anxiety and depression) grouped together, and the assessment of general well-being at the end as in the ESAS-r.
There was no problem with the translation of the item on pain: the English and French terms having the same meaning. An explanation had to be added to the translation of the item on tiredness (“tiredness = lack of energy”): the French word “fatigue” can mean both frailty and exhaustion, as is the case in Spanish.18,40 An explanation also had to be added to the item on drowsiness (“drowsiness = feeling sleepy”), to avoid any confusion between tiredness and drowsiness.
There were no problems with the translations of the items on nausea (nausées), vomiting (vomissements), or constipation (constipation). The Canadian research team who conducted a French translation study of the ESAS-r recommended the expression “envie de vomir” (the need to vomit) to “nausée” (nausea). 28
It appeared that the term “lack of appetite,” translated with a double negative: “pas de manque d'appétit” (no lack of appetite) in the first version, was harder for patients to understand. We therefore tested the terms “bon appétit” (good appetite) and “manque d'appétit maximum” (maximum lack of appetite), which were equally hard to understand. We therefore decided to leave the double negative “pas de manque d'appétit” (no lack of appetite) and “manque d'appétit maximum” (maximum lack of appetite) to maintain coherence with the rest of the scale. In the Canadian and Portuguese versions, the double negative was removed to avoid any confusion over the meaning.28,41 This was also the case for the term “best sleep.” The literal translation “meilleur sommeil” was changed by the scientific committee due to a lack of coherence between the words to “bon sommeil” (good sleep), which was not very well understood by patients. We therefore decided to use a double negative: “pas de trouble du sommeil” (no trouble sleeping) in the final version.
There were long discussions on the terms depression and anxiety. The decision was made to keep the medical terms, as in the original version, with explanatory notes (“depression = feeling sad, anxiety = feeling nervous”)15,31 and these terms did not pose a problem for patients. Watanabe et al. reported the same comments from patients regarding those terms. 32
The term “best/worst wellbeing” was translated with two phrases “je me sens bien” (I feel good) and “je me sens mal” (I feel bad), which patients understood. The problem arose when responding with a number on the NRS, as was the case during transcultural translation of the Thai, 19 Italian, 42 and Canadian 28 versions. The term “wellbeing” is therefore a complex concept, measuring overall quality of life and the link with suffering, which is difficult to translate.43,44 Watanabe et al. reported the same difficulties from the patients. 32
Definitive version
The modifications made are the result of a compromise between patients' comments on comprehension, the acceptability and feasibility of the scale, and the constraints imposed by the questionnaire itself. The definitive version therefore took into account the various comments patients made, which led to some changes in the way items were expressed and the order in which they were presented, but without changing the meaning. The only comments that could not be taken into account were those regarding the structure of the scale itself: the spread being too large with the numbers 1–10 on an NRS, while some patients preferred the QLQ C30 scale with only four numbers (1–4), which are defined by the terms “not at all,” “a little,” “quite a bit,” and “very much.” 45
Time frame
In our study the time frame was specified as “now” because this was how the tool was originally designed and how the EAPC research group proposed the tool. However, it was difficult for some patients to answer on this basis: they preferred to answer “on average” because of the fluctuations in their symptoms. Hannon et al. reported that the participants in their study preferred to talk about the “past 24 hours” rather than “now.” 23 In a qualitative, “think-aloud” study of the original ESAS, Watanabe et al. reported that some patients suggested clarifying the time frame for rating symptoms. 32 In a study of 1147 cancer outpatients, Shi et al. reported that ratings for worst pain over the past week correlated more closely with pain interference than ratings for current pain. 46 Although symptom intensity over the past 24 hours does correlate with symptom intensity “now,” there are significant differences given that symptom burden fluctuates over time. Hui and Bruera suggest that the ESAS, which assesses symptoms “now,” may be particularly useful in assessing interventions with a rapid onset (i.e., the effect of intravenous opioids on dyspnea “now”), whereas the “24-hour” ESAS may be more suitable for everyday clinical practice. 24
French language limitations
Even if a standard French language is generally understandable for everyone in all the mentioned francophone countries, the usual patient population could use a different -national- wording on a daily basis and this is why we are trying to validate a French version in a French population. It would be interesting to study the same version in the three mentioned French-speaking countries (Canada, France, and Switzerland); a future research could focus on that topic.
Limitations
There were limitations in this study. The patients were recruited in a single center. They were also mostly cared for at home and were therefore outpatient, in a relatively stable state and with a high-performance status. We also had a well-educated population. The acceptability and comprehension of, and time taken to fill in, the scale would probably have been different with a population of patients in a generally more advanced stage of illness.
Conclusion
The purpose of this study was to obtain a transcultural validation of the modified 12-item ESAS, ESAS12-F. This enabled us to assess the linguistic qualities of a tool used on a daily basis to assess the symptoms of patients looked after by palliative care teams. The essential next step is now to carry out a psychometric validation of the definitive version of the 12-item ESAS, ESAS12-F.
Footnotes
Acknowledgment
This work was sponsored by Hospices Civils de Lyon.
Author Disclosure Statement
No competing financial interests exist.