
Abstract
Abstract
Background:
Gastrointestinal symptoms, including nausea, vomiting, bowel obstruction, ascites, constipation, and anorexia, are common and often refractory in advanced cancer patients. The palliation of gastrointestinal symptoms is important in improving the quality of life of cancer patients, as well as that of their families and caregivers. Currently published clinical guidelines for the management of gastrointestinal symptoms in cancer patients do not comprehensively cover the topics or are not based on a formal process for the development of clinical guidelines.
Methods:
The Japanese Society for Palliative Medicine (JSPM) developed comprehensive clinical guidelines for the management of gastrointestinal symptoms in cancer patients after a formal guideline development process.
Results:
This article summarizes the recommendations along with their rationale and a short summary of the development process of the JSPM gastrointestinal symptom management guidelines. We established 31 recommendations, all of which are based on the best available evidence and agreement of expert taskforce members.
Discussion:
Future clinical studies and continuous guideline updates are required to improve gastrointestinal symptom management in cancer patients.
Introduction
Gastrointestinal symptoms, including nausea, vomiting, bowel obstruction, ascites, constipation, and anorexia, are common and often refractory in patients with advanced cancer. An estimated 20–70% of patients with advanced cancer have nausea and vomiting,1,2 10–50% have bowel obstruction,3,4 15–50% have ascites,5,6 40–90% have constipation,7,8 and 6–74% have anorexia.9,10 These symptoms distress patients and decrease their quality of life (QOL).
Several clinical guidelines for gastrointestinal symptom management in cancer patients have been published worldwide in an effort to improve symptom control.1,3,4,9,11–16 The Japanese Society for Palliative Medicine (JSPM) first published its Clinical Guidelines for Digestive Symptoms in Cancer Patients in 2011. 17 However, the first JSPM guidelines focused only on the management of nausea, vomiting, and bowel obstruction, while the guidelines from other authorities did not cover the topics comprehensively or were not developed based on a formal scientific process. Thus, the JSPM decided to comprehensively revise the clinical guidelines for managing gastrointestinal symptoms in cancer patients using a validated methodology.
In this study, we present a short summary of the JSPM recommendations for the management of gastrointestinal symptoms in cancer patients with the rationale underlying the recommendations and their development process.
Development process
The objective of developing these clinical guidelines was to establish standard palliative interventions for gastrointestinal symptoms in cancer patients. The target patients of these guidelines are all cancer patients with gastrointestinal symptoms (nausea, vomiting, bowel obstruction, ascites, constipation, and anorexia), excluding those with symptoms induced by chemotherapy or radiotherapy, while the primary users are all health care providers who care for cancer patients, including palliative care physicians, primary care physicians, oncologists, nurses, and pharmacists. The interventions included in our recommendations are those which are available and commonly used in Japan.
Systematic literature search
First, 31 clinical questions (CQs) were developed based on the previous JSPM guidelines and a consensus meeting of taskforce members (11 palliative care physicians, 3 palliative care nurses, 2 pharmacists, and 1 epidemiologist for external evaluation). Thereafter, we performed a systematic literature search for each CQ in PubMed and the Cochrane Central Register of Controlled Trials (CENTRAL), with searches limited to articles written in English or Japanese and published before February 2016. We searched for Japanese articles not included in PubMed or CENTRAL in the Ichushi Web of the Japan Medical Abstracts Society. The policy used to identify relevant articles based on study design was as follows: first, we selected randomized controlled trials (RCTs). If none or only one such article was identified, we extended the search to observational studies. If no relevant articles were identified, we extended the search to RCTs in noncancer patients, since it is known that high-quality research in the area of gastrointestinal symptom management in cancer patients is poor.
The primary screening process included reviewing the titles and abstracts of all articles identified from the databases to select articles potentially relevant to each CQ. All potentially relevant articles underwent a secondary screening process in which the full texts were reviewed. After the secondary screening process, we selected relevant articles to provide evidence for each CQ. Additional articles were identified from the reference lists of selected articles and major palliative care textbooks by manual searches. 18 The literature search for each CQ was performed independently by two taskforce members.
Drafting recommendations and Delphi method
First, draft recommendation statements for each CQ with rationales were written by two-member taskforce teams. We did not consider the specific administration (dose, route, frequency, and time to onset) of each treatment. We used a modified Delphi method to examine the validity of each draft recommendation statement. 19 In brief, the Delphi method is a structured communication technique based on bringing together a group of experts who answer questions in two or more rounds, facilitating the formation of a consensus and recommendations. Delphi rounds were conducted by 11 palliative care physicians; 1 epidemiologist for external evaluation; 4 representatives from other specialties, including an oncologist (Japanese Society of Clinical Oncology), primary care physician (Japan Primary Care Association), nurse (Japanese Society of Cancer Nursing), and pharmacist (Japanese Society for Pharmaceutical Palliative Care and Sciences); and 1 representative of a cancer patient group. The scores for validity of each question were rated on a 9-point scale by each Delphi member. If the median was 8 or more and the difference between the minimum and the maximum was 5 or less, consensus was confirmed. After Delphi rounds and an external review by five external reviewers (three palliative care specialists [JSPM physician, nurse, and pharmacist] and two oncologists [Japanese Society of Medical Oncology and Japanese Society of Gastroenterology]), the final version of the recommendation statements was approved.
Evidence and recommendation levels
We used the grading system developed by the Medical Information Network Distribution Service (Minds) to articulate the level of evidence and the strength of the recommendations following the concepts of The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system 20 (Table 1).
Recommendation Table
Recommendations
Management of nausea and vomiting not induced by chemotherapy or radiotherapy
Selection of antiemetic drugs
Etiology-based antiemetic management
Etiology-based antiemetic management is suggested (2D): If the nausea and vomiting are not caused by chemotherapy or radiotherapy in a cancer patient, treat the etiology and use the appropriate antiemetic drug according to etiology (Fig. 1). If the first-line drug is ineffective or the symptom is refractory to treatment, another antiemetic drug in combination or a second-line antiemetic drug is suggested (2D).
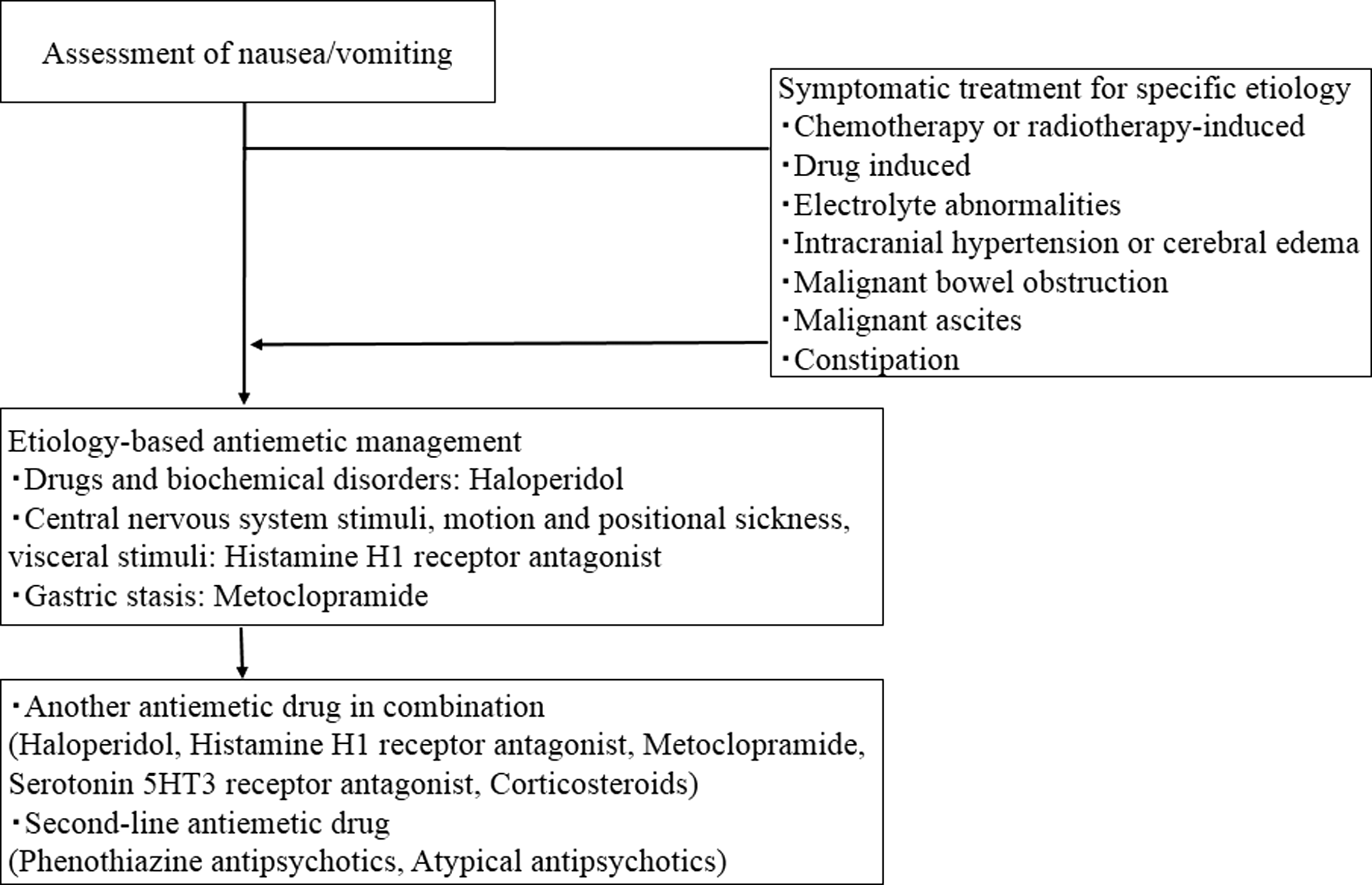
Overview of recommendations for the management of nausea/vomiting.
For this CQ, there were four observational studies but no RCTs.2,21–23 One RCT was published after the publication of this guideline and is not reflected in the result. 24
Four observational studies classified disease etiology into central nervous system stimuli, motion and positional sickness, drugs and biochemical disorders, visceral stimuli, gastric stasis, and others. Depending on etiology, cyclizine, hyoscine, haloperidol, domperidone, metoclopramide, or levomepromazine was used, with an efficacy rate of 70–100%. In all studies in which the first-line drugs were ineffective, another class of antiemetic drug was used in combination with it or a second-line drug of another class was used.
There is insufficient evidence that etiology-based antiemetic management relieves nausea and vomiting in cancer patients. However, based on these observational studies, the etiology-based antiemetic approach has the potential benefit of relieving nausea and vomiting in this population. In contrast, all studies included a single arm and simultaneous treatment according to etiology; therefore, the treatment effect of an antiemetic drug alone cannot be judged. Thus, we suggest that the etiology-based antiemetic approach be used in cancer patients with nausea and vomiting.
Antiemetic drugs
Prokinetics: metoclopramide
The use of metoclopramide is suggested (2C). We found two RCTs that compared the efficacy of metoclopramide with placebo or other drugs. In 1 double-blind RCT of 26 patients with cancer-related dyspepsia that compared the efficacy of metoclopramide and placebo, metoclopramide significantly improved nausea on day 4. 25 In another RCT of metoclopramide, ondansetron, and placebo, no significant intergroup difference was observed in 92 cancer patients with opioid-induced nausea and vomiting. 26 Due to the risk of tardive dyskinesia, the U.S. Food and Drug Administration and the European Medicines Agency advise against its long-term use.
The results of these two RCTs were different, and the evidence is insufficient. In addition, extrapyramidal symptoms were caused by long-term administration. However, it was widely used in the clinical setting, and there were no severe adverse events in these trials. The taskforce members agree that metoclopramide is suggested to be used, but limited to four weeks if possible.
Prokinetics: domperidone
The usefulness of domperidone is inconclusive since we found no study regarding its effects in cancer patients with nausea and vomiting. By contrast, epidemiologic studies that did not include cancer patients showed that a domperidone dose >30 mg/day, elderly people (>60 years old), serious liver disorders or heart disease, and the concomitant drug that causes QT prolongation or CYP3A4 inhibitory action increased the risk of severe ventricular arrhythmias and sudden cardiac death.27–29 For this reason, individual countries have different restrictions and monitoring protocols; however, in Japan, there are few restrictions, and domperidone is widely used.
Due to the lack of evidence and adverse events not being evaluated in cancer patients, no recommendation about the use of domperidone can be made.
Haloperidol
The use of haloperidol is suggested (2C). We found one observational study that evaluated the effects of haloperidol in 42 cancer patients with nausea and vomiting. Regarding the primary end point, complete response was noted in 8 patients, while a partial response was noted in 12. 30 Another systematic review concluded that incomplete evidence is available from published research. 31
The evidence from previous studies is insufficient, and it is possible that adverse events were not sufficiently verified. However, it has been widely used in the clinical setting and was judged by taskforce members to have an assumed benefit that exceeds its harm. Therefore, we suggest the use of haloperidol for nausea and vomiting in cancer patients. However, since adverse events have not been sufficiently verified, the dosage and administration period should be minimized.
Anticholinergics
The use of anticholinergics (scopolamine hydrobromide) is suggested (2D). We found two observational studies that evaluated the effects of anticholinergics. Scopolamine was administered sublingually to 26 cancer patients with nausea, and the nausea score decreased significantly after 15 minutes. 32 In another study, transdermal scopolamine was administered to 13 cancer patients, 11 of whom reported significant improvement. 33 Evidence is insufficient from previous studies, but based on agreement among the taskforce members, the use of scopolamine hydrobromide is suggested in cancer patients with nausea and vomiting.
Histamine H1 receptor antagonist
The use of histamine H1 receptor antagonists is suggested (2D). We found one observational study that evaluated the effects of the histamine H1 receptor antagonist promethazine in 98 cancer patients with nausea and vomiting; the mean score improved significantly. 34 Evidence from previous research is insufficient, but based on agreement among the taskforce members, histamine H1 receptor antagonist use is suggested for cancer patients with nausea and vomiting.
Phenothiazine antipsychotics (chlorpromazine, levomepromazine, and prochlorperazine)
The use of phenothiazine antipsychotics is suggested (2D). We found two RCTs on chlorpromazine, two observational studies on levomepromazine, and one observational study on prochlorperazine.
One RCT compared the effects of tropisetron and chlorpromazine in 160 end-stage cancer patients with nausea and vomiting. No significant intergroup difference was observed on the third day. 35 Similarly, no significant difference was observed in another RCT of 280 patients. 36 In these two trials, patients treated with chlorpromazine reported significantly improved nausea and vomiting compared to before and after administration.
In an observational study in which levomepromazine was administered to 70 cancer patients with refractory nausea and vomiting, the nausea intensity decreased significantly. 37 As an adverse event, 6 patients had numeric rating scale scores ≥7 for drowsiness. Similarly, another observational study on levomepromazine reported improvement in 62% of patients. 38
One observational study that evaluated the effects of prochlorperazine in 359 cancer patients with nausea and vomiting reported significantly improved nausea and vomiting scores. 34
The evidence from previous studies is insufficient, but based on agreement among the taskforce members, the use of phenothiazine antipsychotics is suggested for cancer patients with nausea and vomiting. However, attention should be paid to adverse events, including drowsiness, circulation inhibition, and extrapyramidal symptoms.
Atypical antipsychotics (perospirone, risperidone, and olanzapine)
The use of atypical antipsychotics is suggested (2D). We found three observational studies that evaluated the effects of atypical antipsychotics, showing 64–100% improvement with perospirone, risperidone, and olanzapine administered to 5–20 patients with nausea and vomiting that were refractory to first-line antiemetic drug treatment.39–41 Although the evidence from previous studies is insufficient, based on agreement among the taskforce members, the use of atypical antipsychotics is suggested for cancer patients with nausea and vomiting that is refractory to first-line antiemetic drug treatment.
Serotonin 5HT3 receptor antagonist
The use of serotonin 5HT3 receptor antagonists is suggested for patients in whom the nausea and vomiting are refractory to first-line antiemetic drug treatment (2D). We found three RCTs that compared serotonin 5HT3 receptor antagonists with placebo or other drugs. One double-blind RCT of 92 cancer patients compared the efficacies of ondansetron, metoclopramide, and placebo for relieving nausea and vomiting. No significant intergroup differences were noted. 26 Two other unblinded RCTs of 160 and 280 cancer patients compared the efficacies of tropisetron and other drugs. In the two trials, patients receiving tropisetron reported significantly improved nausea and vomiting compared to controls.35,36 In a previous study, the results were inconsistent and the evidence was insufficient, but based on agreement among taskforce members, serotonin 5HT3 receptor antagonist use is suggested for cancer patients with nausea and vomiting that is refractory to the initial treatment.
Corticosteroids
Corticosteroid use is suggested when a cancer patient's nausea and vomiting are caused by tumor-induced inflammation or cerebral edema (2C). One double-blind RCT of 84 cancer patients compared the efficacies of dexamethasone and placebo for cancer-related fatigue. The secondary endpoint of nausea improved after dexamethasone administration, but the intergroup difference was nonsignificant. 42 Another double-blind RCT of 51 cancer patients whose symptoms were refractory to metoclopramide compared the efficacy of dexamethasone and placebo. 43 Although patients reported symptom improvement after dexamethasone administration, the intergroup difference was nonsignificant.
In previous studies, the therapeutic effect of corticosteroids did not differ from that of a placebo, and evidence of their efficacy was insufficient. However, since corticosteroids are considered to be effective in tumor-induced inflammation and cerebral edema by the taskforce members, the use of corticosteroids is suggested when a cancer patient's symptoms are caused by tumor-induced inflammation or cerebral edema.
Mirtazapine
The usefulness of mirtazapine is inconclusive. We found one observational study that evaluated the effects of mirtazapine. Of the 42 cancer patients diagnosed with depression with nausea or insomnia, 28 reported improvement in their nausea. 44 However, it is possible that the depression simply improved with mirtazapine, and since high-quality research is lacking, we cannot determine whether mirtazapine use should be recommended.
Management of nausea and vomiting in malignant bowel obstruction
Nasogastric tube
The use of a nasogastric tube is suggested, but limited to short periods (2D). We found no studies regarding the effects of a nasogastric tube on malignant bowel obstruction (MBO). However, it is frequently used in clinical practice, and its treatment effect has been established. In addition, its effect can be quickly and easily evaluated. In contrast, patient preference and adverse events (esophageal erosion, sore throat, sinusitis, and aspiration pneumonitis) require attention. 4 There is insufficient evidence of whether nasogastric tube use relieves nausea and vomiting in patients with MBO. Nonetheless, based on taskforce member agreement, nasogastric tube use is suggested.
Percutaneous endoscopic gastrostomy/percutaneous transesophageal gastro-tubing
The use of percutaneous endoscopic gastrostomy (PEG) and percutaneous transesophageal gastro-tubing (PTEG) is suggested when patients have a prognosis that exceeds two months (2C). We found four observational studies of PEG and one observational study of PTEG for relieving nausea and vomiting caused by MBO. In these observational studies, the effective rate for nausea/vomiting in cases wherein the procedure could be performed was 77–97%, the incidence of infections was 8–14%, and the rate of serious complication such as death was 0.2%.45–49 The evidence from previous studies is insufficient; however, based on agreement among the taskforce members, PEG/PTEG is suggested for nausea and vomiting due to MBO.
Corticosteroids
Corticosteroids are suggested to be used (2C). We found two RCTs that compared the efficacy of corticosteroids and placebo. One double-blind RCT of 39 cancer patients compared the efficacy of dexamethasone and placebo in MBO. However, the study was terminated because of slow accrual; moreover, comparison between the groups was not performed. 50 Another double-blind RCT of 58 MBO patients compared the efficacy of methylprednisolone and placebo. There was no significant difference between the two groups with regard to the primary end point, but corticosteroid use showed a significant improvement in patients without a nasogastric tube. 51 The previous studies were small-scale RCTs, and the superiority to placebo was not clearly evident; however, based on agreement among the taskforce members, corticosteroids are suggested to be used.
Octreotide
Octreotide is suggested to be used (2C). We found six RCTs that compared the efficacy of octreotide and placebo or butylscopolamine. One double-blind RCT of 87 MBO patients compared the efficacy of octreotide and placebo. There was no significant difference in the number of days free of vomiting between groups and total number of people free of vomiting for 3 days. 52 Another double-blind RCT of 64 MBO patients compared the efficacy of long-acting release octreotide and placebo. There were no significant intergroup differences because of insufficient recruitment and premature discontinuation. 53 Another double-blind RCT of 97 patients with MBO due to ovarian cancer compared the efficacies of octreotide and butylscopolamine for nausea. Octreotide showed significant improvement compared to butylscopolamine on days 2 and 3. 54 In three other small RCTs, compared to butylscopolamine, octreotide significantly reduced the number of vomiting episodes, degree of nausea, and drainage from the stomach.55–57 The evidence from previous studies is insufficient and the evaluation methods differed among studies, but based on taskforce member agreement, the use of octreotide is suggested.
Butylscopolamine
The use of butylscopolamine is suggested (2C). We found four RCTs that compared the efficacy of butylscopolamine and octreotide. All studies were designed as control groups of octreotide and showed significant inferiority of butylscopolamine to octreotide. However, the degree of nausea and number of vomiting episodes were significantly improved.54–57 The evidence was insufficient, but based on taskforce member agreement, the use of butylscopolamine is suggested.
Histamine H2 receptor antagonist or proton pump inhibitor
The use of a histamine H2 receptor antagonist (H2RA) or proton pump inhibitor (PPI) is suggested (2D). We found no studies regarding the effects of H2RA or PPI on nausea and vomiting in MBO patients. Using a review of seven studies of patients in the perioperative period as a reference, we found that both PPI and H2RA reduced gastric secretions and that the most superior agent is ranitidine. 58 Although only indirect evidence is currently available, the drugs are safe and widely used as a cotreatment for MBO; thus, the use of H2RA or PPI is suggested.
Antiemetic drugs
The use of antiemetic drugs is suggested (2D). We found five observational studies that evaluated the effects of antiemetic drugs against nausea and vomiting in MBO patients. Haloperidol, phenothiazine antipsychotics, olanzapine, metoclopramide, and granisetron were administered. The effective rate was 75–100%, and some agents caused drowsiness as a side effect.59–63 Most of the previous studies could not exclude the effects of corticosteroids as cotreatment, and the evidence was insufficient. However, based on taskforce member agreement, the use of antiemetic drugs is suggested.
Management of malignant ascites
Diuretics
The use of diuretics (spironolactone and furosemide) is suggested (2D). We found three observational studies that evaluated the effects of diuretics for abdominal distension of malignant ascites. In the three trials of spironolactone, spironolactone and/or furosemide, and tolvaptan, the drugs were administered to 15, 16, and 10 patients, respectively, and their abdominal distension improved significantly. Adverse events included renal dysfunction and electrolyte abnormalities.64–66 Previous studies were small in size and observational by design with insufficient evidence, but based on taskforce member agreement, the use of spironolactone and furosemide is suggested. Tolvaptan use requires caution because of the risk of electrolyte abnormalities and renal failure; thus, it is not recommended.
Abdominal paracentesis
The use of abdominal paracentesis is suggested. If puncture occurs frequently, the use of an indwelling peritoneal catheter should be considered (2D). We found seven observational studies that used peritoneal catheters for continuous drainage67–73 and one on simple paracentesis using needles 74 and evaluated the effects of abdominal paracentesis for abdominal distension induced by malignant ascites. In these studies, the devices and outcome assessment methods were different, and the improvement rate of abdominal distension was 37.5–100%, which is a large difference. Evidence is insufficient despite its established effectiveness; however, based on taskforce member agreement, the use of abdominal paracentesis is suggested.
Cell-free and concentrated ascites reinfusion therapy
The usefulness of cell-free and concentrated ascites reinfusion therapy (CART) cannot be concluded. We found one observational study that evaluated the effect of CART. Although abdominal symptoms improved in this study, symptom improvement cannot be determined to be a benefit of CART treatment alone because reinfusion is performed after peritoneal puncture drainage. 75 No previous studies are of high quality, the evidence is insufficient, and practicing medical institutions are limited in Japan; thus, a recommendation of its use cannot be made.
Denver peritoneovenous shunts
The usefulness of Denver peritoneovenous shunts cannot be concluded. We found four observational studies that evaluated the effects of Denver shunts. In these studies, in 87 MBO patients, the abdominal symptom improvement rates were 67–100%. However, serious adverse events such as heart failure, pulmonary edema, and disseminated intravascular coagulation syndrome were observed in 20% of the patients.76–79 It is possible that abdominal paracentesis is unnecessary in patients using peritoneovenous shunts, but the safety evidence is inadequate; thus, its use cannot be recommended.
Management of constipation
Osmotic laxative and stimulant laxative
The use of osmotic laxatives is recommended (1C). The use of a stimulant laxative is recommended (1C). We found one RCT and one non-RCT that compared the efficacy of osmotic, stimulant, and other laxatives.
One RCT of 75 cancer patients using opioids compared the efficacy of lactulose and senna for constipation. In the 7-day study period, the number of defecations over 72 hours was 0.9 in the lactulose group and 0.9 in the senna group, a nonsignificant intergroup difference. 80 Another non-RCT of 348 cancer patients compared the efficacies of lactulose, sodium picosulfate, and polyethylene glycol for constipation. There was a nonsignificant intergroup difference in the incidence of constipation. 81 There were no significant differences in adverse events and tolerability in these two trials. Thus, the superiority and inferiority of each laxative in previous studies are unclear, 82 but their clinical efficacies have been established and they have been widely used. Osmotic and stimulant laxatives are recommended to be used.
Lubiprostone
The use of lubiprostone is suggested (2C). We found no RCTs regarding the effects of lubiprostone for constipation in cancer patients. However, we found four RCTs that compared the efficacy of lubiprostone and placebo or senna in noncancer patients with opioid-induced constipation. Three trials compared lubiprostone to placebo in 413, 431, and 124 constipation patients, respectively, and a significantly increased spontaneous bowel movement trend was observed compared to placebo.83–85 In one trial that compared lubiprostone with Senna use in 56 patients, a nonsignificant intergroup difference in constipation symptoms and QOL was reported. 86 Therefore, there is no research on cancer patients and only indirect evidence is available. However, similar improvement of constipation is expected in cancer patients. In contrast, considering the high cost, and taskforce member agreement, lubiprostone use is suggested only when necessary.
Peripherally acting μ-opioid receptor antagonists
Peripherally acting μ-opioid receptor antagonists were excluded because they were not available in Japan at the time of the systematic literature search.
Management of anorexia not induced by chemotherapy or radiotherapy
Corticosteroids
The use of corticosteroids is recommended (1B). We found six RCTs that compared the efficacy of corticosteroids and placebo for cancer-related anorexia. One double-blind RCT of 50 cancer patients compared the efficacy of methylprednisolone and placebo and demonstrated that the anorexia on day 7 improved significantly compared with placebo. 87 Although evaluation methods and periods differed, four of the other five studies also showed significant improvement,88–91 and there was no significant difference in only one trial. 43
The available evidence is almost consistent and shows a significant improvement in anorexia in cancer patients with corticosteroid use compared to placebo. Corticosteroid use is recommended. However, careful attention is necessary because efficacy and safety in patients with long-term administration or poor general condition have not been sufficiently evaluated.
Metoclopramide
The use of metoclopramide is suggested (2D). We found one RCT that compared the efficacy of metoclopramide and placebo and two observational studies. One double-blind RCT of 26 cancer patients with cancer-related dyspepsia compared the efficacy of metoclopramide and placebo. The nausea on day 4 improved significantly compared with the effect of placebo, but there was no difference in anorexia. 25 In one observational study, although nausea improved, there was no improvement in anorexia. 92 In another observational study, appetite improved in 65% of patients after usage. 93 Thus, the evidence is insufficient, but based on agreement among the taskforce members, metoclopramide is suggested to be used.
Rikkunshito, a Japanese herbal medicine
The usefulness of rikkunshito is inconclusive. We found no studies regarding the effects of rikkunshito for anorexia in cancer patients. One observational study evaluated rikkunshito in gastric cancer patients after gastrectomy. Although this study showed an improvement in appetite, the pathophysiology differs from that of cancer-bearing patients with anorexia. 94 Thus, the evidence is insufficient to make a recommendation.
Eicosapentaenoic acid
Eicosapentaenoic acid (EPA) is suggested not to be used (2B). We found one RCT that compared the efficacy of EPA and placebo. In a study comparing the effects of EPA and placebo on anorexia in 518 cancer patients with weight loss, no significant differences were observed. 95 In a review that included patients currently receiving chemotherapy, no significant differences from placebo were noted in terms of anorexia. 96 Therefore, EPA has not been shown to improve anorexia compared to placebo, and with concordance between the results of multiple high-quality studies, EPA is not suggested for use.
Progestogen
The use of progestogen is suggested (2B). We found five RCTs that excluded patients currently receiving chemotherapy, one RCT, one systematic review that included patients receiving chemotherapy on the effect of megestrol (MA; not available in Japan), and four RCTs, including chemotherapy, regarding the effect of medroxyprogesterone acetate.
In the five studies of MA, 240–480 mg significantly improved anorexia compared to placebo, and all the studies provided consistent results. Serious adverse events did not differ between groups.97–101 In a study comparing MA, dexamethasone, and fluoxymesterone, MA and dexamethasone improved appetite more significantly than fluoxymesterone. 102 In a systematic review, including patients currently receiving chemotherapy, the relative ratio of efficacy compared to placebo was 2.57 (95% confidence interval 1.48–4.49); the risk of pulmonary embolism has been shown to increase in the case of higher doses (800 mg). 103 Three of the four trials on medroxyprogesterone acetate showed significant improvement in anorexia.104–107
Available evidence indicates significant improvement of anorexia in cancer patients by progestogen, but in Japan, it has been approved only for breast cancer and endometrial cancer, and its use for other cancers is lacking.
Discussion
To the best of our knowledge, this is the first set of published clinical guidelines for the management of gastrointestinal symptoms in cancer patients that has been established following a formal guideline development process (Table 2). The recommendations of the JSPM gastrointestinal symptom guidelines presented in this study are based on the combination of the best available evidence and expert consensus. It is difficult to conduct high-quality clinical research of symptom control in advanced cancer patients because of the vulnerability of patients, as well as ethical conflicts. In fact, the evidence levels for most of our recommendations were low. Because of the lack of rigorous evidence, recommendation statements based on expert consensus and the best available evidence, such as ours, play an important role in guiding health care providers to the optimal clinical decisions. Despite our best efforts, we could not find sufficient data regarding the effect of treatment on QOL and pharmacoeconomic outcomes. Thus, we discourage the use of individual recommendations in isolation without the consideration of patient preference and the pharmacoeconomic aspect of treatment.
Summary of Recommendations
CART, concentrated ascites reinfusion therapy; EPA, eicosapentaenoic acid; H2RA, H2 receptor antagonist; MBO, malignant bowel obstruction; PEG, percutaneous endoscopic gastrostomy; PPI, proton pump inhibitor; PTEG, percutaneous transesophageal gastro-tubing.
Finally, RCTs comparing placebo or each intervention and clinical studies on the effects of combinations of intervention are necessary for almost all CQs. In particular, the establishment of evidence for cancer patients is required for domperidone and mirtazapine for nausea and vomiting, CART and Denver peritoneovenous shunts for malignant ascites, and rikkunshito for anorexia, all of which could not be concluded. There is also a need to determine the optimal dose, frequency, and administration route (oral, injection, rectal, etc.) and when to recommend each intervention. Furthermore, there is a need to establish the methodology of clinical trials for gastrointestinal symptoms in patients with advanced cancer, especially a consensus on appropriate outcomes to determine the response of interventions. In addition, continuous guideline updates are required to improve the quality of gastrointestinal symptom management in cancer patients.
Footnotes
Acknowledgments
The authors thank the Japanese Society of Gastroenterology, Japanese Society of Clinical Oncology, Japanese Society of Medical Oncology, Japan Primary Care Association, Japanese Society of Cancer Nursing, and Japanese Society for Pharmaceutical Palliative Care and Sciences for their cooperation and advice during the development of these recommendation statements. This work was funded by the Japanese Society for Palliative Medicine.
Author Disclosure Statement
No competing financial interests exist.