
Abstract
Abstract
Background:
Despite the importance patients place on religion and spirituality, many patients with advanced diseases report that their religious and spiritual needs are not met by their health care team, and many nonchaplain clinicians feel unprepared to address religious and spiritual issues in their practice.
Objectives:
The purpose of this study was to assess the efficacy of a one-day workshop on spiritual care for nonchaplain clinicians who provide care to elderly long-term care patients.
Methods:
Clinician participants (N = 68) were given a pre-survey at the beginning of the workshop, a post-survey at the conclusion of the workshop, and a three-month follow-up survey to evaluate their comfort in engaging in spiritual issues before and after the workshop. An average ability score of 13 items in the survey was calculated as well as an average comfort score, which was an average of three items in the survey. Ability scores and comfort scores were analyzed using a pairwise t-test, comparing pre- versus post-workshop and post- versus three-month scores.
Results:
Overall average scores for clinicians' self-reported perceived ability in engaging in issues around spirituality with patients and their families increased from before the workshop to the post-workshop and three months later. Participants' self-perceived comfort increased from before the workshop to immediately following the workshop.
Discussion:
This study suggests that a spiritual care training program targeted toward geriatric clinicians has the potential to provide clinicians with the tools, skills, and support they need to approach basic spiritual care with their patients and family members.
Introduction
Religion and spirituality are considered to be important aspects of many Americans' lives and particularly for individuals who are older. By 2035, people aged 65 and older will account for more than 20% of the U.S. population. 1 About two-thirds of adults age 65 and older report that religion is very important to them, with an additional 20% of adults over 65 who consider religion to be somewhat important. 2 Studies of religion, aging, and health examine a variety of aspects of religion that affect older individuals' physical and mental health, such as religious participation, 3 religious meaning, 4 and religious coping. 5 These different dimensions of religion demonstrate the positive effects religion has on the overall health and quality of life of older cohorts in the US.6,7
In times of older age and illness, and more specifically in the setting of the nursing home, religion and spirituality have been shown to provide older patients and their families with a source of strength, hope, coping, and a sense of meaning in their life.4,8 Koenig et al. found that 59% of nursing home residents in their sample used religion as a method for coping to deal with health and social issues. Religion and spirituality also play a role in how patients and families make medical decisions and provide both patients and families with a sense of peace and comfort when a patient is at the end of life. 9
Despite the importance patients and their families place in religion and spirituality, many patients with advanced diseases report feeling that their religious and spiritual needs are not met in their religious and spiritual communities or by members of their health care team.10,11 Chaplains often provide this care, but there are not enough of them to meet the demand in the geriatric and palliative care contexts. In addition, many nonchaplain clinicians feel unprepared to address religious and spiritual issues in their clinical practice. 12 Studies demonstrate that nurses and physicians do wish to provide spiritual care to their patients, yet there are barriers to doing so, particularly at the end of life, including a lack of time and a lack of training regarding spiritual care. 13
Educational workshops and training programs that provide clinicians who are not chaplains or students training to be clinicians with the tools and resources to address spiritual issues with patients and their families can be effective strategies for improving clinicians' knowledge about providing spiritual care,14,15,16 level of confidence, 17 comfort,18,19 and ability to provide general spiritual care.18,20 A few studies evaluated the effects of the spiritual care training on patient outcomes, including improvement in health care professionals' attention to patients' spiritual and existential needs 21 and increases in quality of life for patients who were cared for by staff who received training in spiritual care. 22 Daudt et al. report that their spiritual care education program prompted a process of culture change within their hospice, including changes in practices of their organization. 23 The above studies have used a variety of modes for teaching about spiritual care such as lectures, case studies, self-reflective exercises, and simulations over the course of different lengths of time, including 30-minute training sessions, one-day workshops, and a multimonth-long fellowship.
Robinson et al. found that their one-day training program for pediatric interprofessional practitioners was effective in terms of 15 core spiritual care skills. 16 These skills increased for participants immediately following the training as well as three months later from baseline. The workshop was particularly effective for those with lower levels of perceived spirituality. Another study reported on the effects of Clinical Pastoral Education (CPE), a five-month-long fellowship program for health care providers, on clinicians' provision of spiritual care. It found that practitioners who participated in the program experienced an increase in self-perceived ability, comfort in using religious and spiritual language, and confidence in providing spiritual care. 20 Other pedagogies included the use of simulation, which proved effective for learning about spiritual care. 19
Because of the significance of religion and spirituality particularly to older groups of patients, addressing religious and spiritual issues is important for clinicians who provide care for this cohort of patients. The purpose of this study was to assess the efficacy of a one-day workshop on spiritual care for nonchaplain clinicians who work in two different facilities that provide care to seniors. This study was adopted for geriatric care providers and modeled after that of Robinson et al. (2016)'s study, which focused on a spiritual generalist training for pediatric nonchaplain clinicians. The workshop was designed to educate nonchaplain clinicians who care for older patients on how to conduct a spiritual screening, to respond to spiritual concerns of patients and their families, and to give them tools to provide basic spiritual care to the patients and families to whom they provide care. The aim of this study was to assess the delivery of this spiritual care workshop to clinicians who serve a senior population of residents in a nonhospital setting.
Methods
Three workshops were held at Hebrew SeniorLife in January and February 2018, and three-month follow-up surveys were administered in April and May 2018. Clinicians were notified of the Spiritual Generalist workshops through e-mail invitations and flyers. Participation in the first two workshops was voluntary. The third session was provided for Hebrew SeniorLife's multidisciplinary committee of culture change liaisons. Participants were given a presurvey at the beginning of the workshop, which asked them about their ability and comfort level in engaging in spiritual issues with patients and families, as well as their knowledge of spiritual resources at Hebrew SeniorLife. We administered a post-survey at the conclusion of the workshop as well as a three-month follow-up survey through email to assess change over time with ability, comfort level, and knowledge of spiritual issues.
The study was reviewed by the IRB at Hebrew SeniorLife and Brandeis University and was considered exempt. Clinicians received a letter in their workshop folder notifying them of the research study, which outlined the purpose of the surveys and stated that their participation in the research aspects of the workshop was voluntary.
Spiritual generalist workshop
The Spiritual Generalist workshop was modeled after a similar workshop held at Boston Children's Hospital through the Program to Enhance Relational and Communication Skills (PERCS) of the Institute for Professionalism and Ethical Practice.16,24 This day-long workshop covered four main topical areas: describing the foundations of becoming a spiritual generalist, familiarizing oneself with spiritual screening, recognizing and addressing spiritual distress, and collaborating and identifying resources with chaplaincy services at the sites. The workshop included didactic use of PowerPoint presentations to describe religion/spirituality and differences between religious and secular language; brief video to illustrate the rationale and use of the FICA instrument; live simulations with professional actors and debriefing opportunities; slideshow to depict the spiritual resources within the institutions; and navigation of the institution's website to familiarize participants with the chaplaincy department and spiritual resources. The use of simulations has been noted to be effective in teaching communication skills to interprofessional clinicians 25 and spiritual care skills. 19
Measures
We used a modified version of the instrument used by Robinson et al. (2016), originally developed by Puchalski, to assess ability in providing spiritual care (personal communication). The average ability score is an average score of 13 items in the survey. These questions ask about respondents' abilities as a spiritual generalist, each in a five-point Likert scale (1 = Not at all able, 5 = Highly able). The average comfort score is an average of three items in the survey. These questions evaluate respondents' confidence and comfort in providing spiritual care, each in a five-point scale with 1 being the least and 5 being the most. In addition, the survey included questions about the frequency with which the clinician engages patients or families around spiritual needs as well as the frequency the spiritual generalist interacts with a chaplain, each measured on the same frequency scale (1 = Never, 9 = Every day). The familiarity with accessing chaplaincy resources available to the spiritual generalist and their patients and families is measured on a four-point Likert scale (1 = Not familiar at all, 4 = Very familiar).
Statistical analysis
Descriptive statistics were conducted to describe the participants' demographic characteristics. Ability scores and comfort scores were analyzed using a pairwise t-test, comparing pre- versus post-workshop and post versus three-month scores. Statistical analysis was conducted using Stata (version 15.1).
Findings
Participants were on average 47.3 (SD = 12.4) years old, with more than 15 years of experience. More than half (62.12%) were Caucasian not of Hispanic origin, and the majority (96.92%) were female. Clinicians who participated in the workshops were from a variety of disciplines and included nurses, social workers, chaplains, personal care assistants, occupational therapists, and music therapists (Table 1 for more details).
Demographics of Workshop Participants
Other includes activities assistant, coordinator, manager, physician, resident services, and wellness coach transition liaison
While the training was designed for nonchaplain clinicians, three chaplains participated in the workshop.
A total of 68 clinicians participated in the Spiritual Generalist workshop, and 44 (64.7%) completed the three-month follow-up survey. There was no selection bias for those who did not complete the three-month follow-up survey. Table 2 presents the demographic characteristics and outcome variables for those who did and did not complete the three-month survey.
Demographic Characteristics of Participants Who Did and Did Not Complete the Questionnaire at Three Months
Ability questions
There was a significant increase in the average ability score from the presurvey at the beginning of the workshop (3.1) to the post-survey immediately following the workshop (4.5) (Fig. 1).

Average Ability Score for Pre- and Post-Workshop (N = 39 participants). (Note: ***p < 0.001.)
We observed a slight but statistically significant decrease in the average ability score after three months compared with at the end of day of the spiritual generalist workshop training (Fig. 2).

Average Ability Score for Post-Workshop and Three-Month Follow-up (N = 26 participants). (Note: **p < 0.01.)
In terms of each ability item, the trends are consistent. For each item, their ability score increased significantly in the post-survey immediately following the workshop (see Fig. 3).
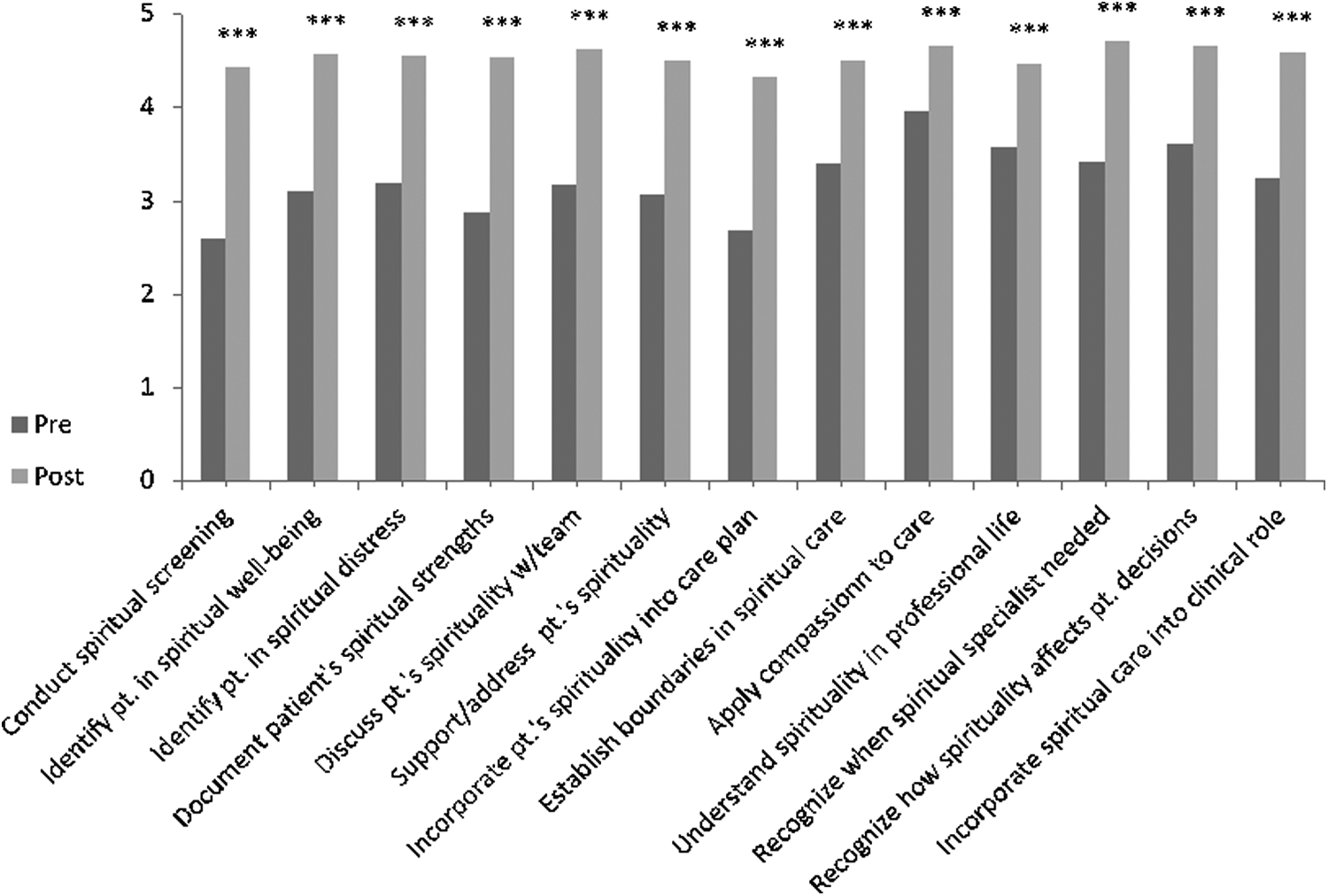
Level of Ability as a Spiritual Generalist (Pre- and Post-Workshop). (Note: ***p < 0.001.)
There was a slight decrease from immediately following the workshop to the three-month follow-up survey (Fig. 4 for details).
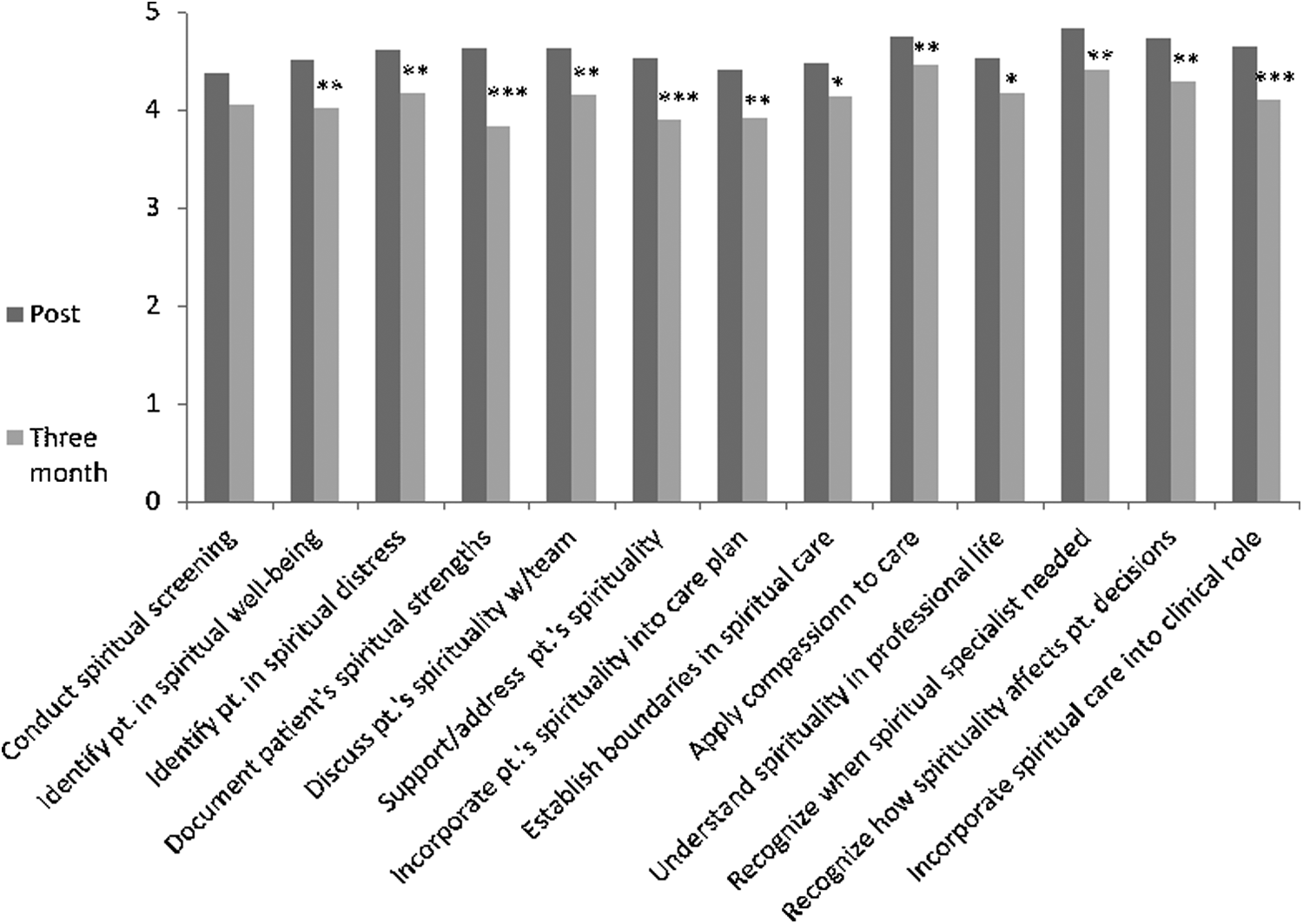
Level of Ability as a Spiritual Generalist (Post-Workshop and at Three-Month Follow-up). (Note: *p < 0.05; **p < 0.01; ***p < 0.001.)
Comfort
We also found that clinicians demonstrated improvements in terms of their comfort and in engaging in spiritual issues with patients and their caregivers. The average comfort score increased from baseline (2.8) to immediately following the workshop (4.2). Analyses at the three-month follow-up time point were not conducted on the comfort score because less than a third of participants completed the questions around comfort at three months (see Fig. 5).

Level of Comfort as a Spiritual Generalist (Pre- and Post-Workshop). (Note: ***p < 0.001.)
These trends were consistent for questions relating to the level of confidence as a spiritual generalist in one's role and comfort in providing spiritual care to a patient or family member of a similar religious or spiritual background. Interestingly, there was an overall improvement from baseline to the post-workshop survey in the level of comfort in providing spiritual care to a patient or family member of a different religious or spiritual background.
Level of engagement of spiritual care with patients and families
There was no difference in the frequency clinicians engaged patients and families around spiritual needs and resources from the post-workshop to the three-month follow-up (n = 37, p = 0.59).
Discussion
The overall increases in the learners' perceived average ability score from baseline to the post-workshop survey and the three-month follow-up survey demonstrate the effectiveness of the spiritual generalist workshop for improving clinicians' ability in engaging in discussions around spirituality with patients and their caregivers. The increase in the average comfort score also increased from before the workshop to immediately following the workshop. In addition, there was an increased improvement from baseline to immediately following the workshop in clinicians' comfort level in providing spiritual care to patients and family members of a religious or spiritual background different from their own. While most of these findings suggest a significant improvement from before the workshop to immediately following the workshop with a slight decrease at three months, we acknowledge that the time since the workshop may account for the slight decrease in improvement from the post-survey to the three-month survey. It is also possible that during the three months since the workshop, participants experienced the complexity of engaging in spiritual issues directly with patients and caregivers in real life.
The findings from this study are consistent with those of Robinson et al. (2016) who found a similar trend in overall improvement in the total ability score (as compared with the average ability score used in this analysis) from before the spiritual generalist workshop to immediately after, with a slight decrease from the post-workshop at three months, for pediatric clinicians. Building on the work of Robinson et al., this study demonstrates that a spiritual generalist workshop can also be beneficial for clinicians who provide care for older patients in a geriatric setting. The results from this study also confirm previous findings from other studies that assess the effectiveness of a workshop in general spirituality for clinicians in improvements in the ability to provide general spiritual care,18,20 level of confidence, 17 and comfort.18,19
Because of the importance of religion and spirituality to older Americans, it is especially important for geriatric clinicians to be able to engage in issues around spirituality in providing care to these patients and their family members or caregivers. Studies, however, find that patients would like their health care providers to provide spiritual support, yet clinicians feel uncomfortable or unprepared to provide do so. 12 Furthermore, there is an increasing need for the integration of spirituality into medicine. 26 The results from our study suggest that a one-day workshop that trains clinicians on how to support or address general spiritual issues for patients and their families can be an effective way to mitigate some of these challenges in providing care. Additionally, as spiritual care generalists, clinicians learned how to conduct spiritual screening, recognize spiritual distress, and when and how to refer to chaplains (spiritual specialists), suggesting an improvement in the overall process of referral and spiritual care.
This study was conducted at one geriatric health care institution in the Northeast United States, and therefore the findings may not be generalizable to all geriatric or other facilities. Only one physician participated in the workshop. Most participants were also older (average age of 47) with significant levels of experience. Most of the participants were female (96%), reflecting the reality of female caregivers for the elderly in the workforce and is therefore representative of who provides direct care for elderly patients. In addition, some clinicians were delayed in filling out the three-month post-follow-up survey, and several reminders were sent so some clinicians completed the three-month post-follow-up survey up to five months following the workshop. Because of missing data in the three-month follow-up survey, we only conducted a pairwise comparison t-test for the presurvey and post-survey for the average comfort score. Despite the limitations of the study, we believe that our findings demonstrate an overall improvement in ability and comfort for clinicians in providing basic spiritual care to patients and their families. Future research may consider the effects of the spiritual generalist workshop on care delivery processes and how senior patients and family members themselves perceive the workshop to influence the quality and availability of spiritual care provided to them by their health care providers.
Conclusion
This study demonstrated the feasibility and effectiveness of a one-day training workshop for geriatric clinicians across disciplines in basic spiritual care. Clinicians reported improvements in their ability to provide a generalist-level spiritual care and their comfort and confidence levels in engaging in issues around spirituality with patients and their family members. A spiritual care training program targeted toward clinicians who care for an older adult population, therefore, has the potential to provide clinicians with the tools, skills, and support they need to approach generalist-level spiritual care with their patients and their family members.
Footnotes
Funding Statement
This project was funded by the Macy Foundation.
Author Disclosure Statement
The authors declared no potential conflicts of interest.