
Abstract
Background:
Older adults frequently report a preference to “trial” intubation and mechanical ventilation (MV) if faced with life-threatening respiratory failure. Understanding the anticipated outcome of unplanned MV is key to structuring a time-limited trial of treatment.
Objective:
To characterize the time-to-death (TTD) among adults 65 years of age and older, who undergo emergency intubation and MV.
Design:
Retrospective cohort study.
Setting/Subjects:
All patients 65 years of age and older, who underwent emergency department (ED) intubation from 2008 to 2015, from 417 hospitals were included.
Measurements:
The primary outcome was TTD after emergency intubation.
Results:
We identified 41,463 ED encounters. The median TTD was three days (interquartile range, IQR, 1–8). There was a statistically significant change in the median TTD by age decile, with the shortest TTD, two days, in the oldest age group (p < 0.001). TTD was shortest among those with myocardial infarction (one day, IQR 4) and sepsis (two days, IQR 5). Bivariate analysis comparing TTD by Charleston Comorbidity Index (CCI) revealed a trend of increasing TTD with increasing CCI score among decedents. Patients with a CCI of 0 had a median TTD of one day (IQR 4), whereas the median TTD among those with a CCI >4 was four days (IQR 9).
Conclusions:
In a large, nationally representative cohort of older adults undergoing ED intubation, the median time from intubation to death was short; however, the length of time between intubation and death varied considerably by principal diagnosis. This information will help guide providers' prognostication after emergency intubation and enhance serious illness conversations by informing expectations.
Tweet:
Thirty-five percent of older adults die after ED intubation—most only survive two or three days after intubation.
Introduction
Nearly 70%
Understanding the anticipated prognosis is key to providing expectations to families after emergency intubation of older adults. Specifically, having an estimate of the length of time in which a patient is at higher risk of death after emergency intubation and death can help providers guide family expectations. However, data regarding the outcomes after emergency intubation among older adults are limited to studies focused on specific clinical conditions such as dementia3,8 or cancer, 9 and utilize data that are now 10–20 years old.3,8 No study has focused on the time-to-death (TTD) among the estimated 30% of older adults undergoing emergency intubation, who do not survive hospitalization.
The objective of this study is to further characterize TTD among adults older than 65, who undergo emergency intubation and MV. This information will help guide providers' prognostication after emergency intubation and enhance serious illness conversations by informing expectations.
Methods
Data for this investigation came from the Vizient Clinical Data Base/Resource Manager™ (CDB/RM™), an individual-level administrative database from a consortium of 117 academic medical centers and over 300 affiliated hospitals across the United States. 10 Using data from 2008 to 2015, we identified all emergency department (ED) encounters of patients 65 years of age and older, who required ED intubation, determined by procedure codes for intubation (CPT 31500). Patients were included in the analysis whether they died in the ED or were admitted to the hospital. Encounters with principal hospital diagnosis code(s) for trauma and cardiac arrest were excluded, given that the natural history of these disease processes is often determined by powerful confounders, such as the use of targeted temperature management, which we would not be able to measure in this administrative database.11,12 Patients receiving out-of-hospital intubation were also excluded.
Data included patient demographic information, procedure codes, diagnosis codes, length of stay (LOS), and in-hospital mortality. Our primary outcome was TTD after ED intubation measured in median number of days and interquartile ranges (IQR). Encounters with missing data for the outcome (death) were excluded from the analysis. A priori predictor variables for the primary outcome included the following: age, principal hospital diagnosis, and Charlson Comorbidity Index (CCI) score. Bivariate associations between each variable and the primary outcome were analyzed using chi-square analysis. The Strobe Guidelines for reporting cohort studies were followed. 13 This study was approved by the hospital's institutional review board.
Results
We identified 41,463 ED encounters of patients 65 years of age or older, who underwent nontraumatic ED intubation. There were no missing data on the primary outcome (in-hospital death). There were 6427 patients with missing data for the principal diagnosis, leaving a total of 35,036 patients for that analysis. Just over half of the patients were female (54%). The majority were >75 years of age (54%) and white (64%). Nearly half of patients were 65–74 years of age and only 7% were >90 years of age. Overall hospital mortality was 35%; however, for those older than 90, mortality was 50% (Table 1).
Baseline Characteristics
p-Value based on Kruskal-Wallis testing.
The median TTD was three days (IQR 1–8). The median TTD was three days among those 65–74 years of age (IQR 1–8), 75–79 years of age (IQR 1–8), and 85–89 years of age (IQR 1–7). The median TTD was two days among those 80–84 years of age (IQR 1–7) and those >90 years of age (IQR 1–6). These differences were statistically significant, showing a trend of shortest TTD in the oldest age group (p < 0.001) (Table 2).
Length of Stay Among Decedents and Survivors
p-Value based on Kruskal-Wallis testing.
LOS for decedents is time-to-death.
LOS for survivors is time-to-discharge.
IQR, interquartile range; LOS, length of stay.
When evaluating TTD by primary hospital diagnosis, TTD was shortest among those with myocardial infarction (one day, IQR 1–4), cerebrovascular accident (two days, IQR 1–5), and cardiac dysrhythmia (two days, IQR 1–4). The two most common diagnoses, sepsis (43%) and respiratory failure (22%), had a TTD of three and four days, respectively (Table 2). Patients with principal diagnosis of seizure had the longest median TTD (nine days, IQR 5–13). Among survivors of ED intubation, hospital stays were over a week long (nine days, IQR 5–15).
Overall, the probability of dying diminishes with each day of survival (Fig. 1). For instance, nearly 90% of those with an LOS of only one day are decedents, whereas among those with an LOS of eight days, only 18% are decedents. Paradoxically, bivariate analysis comparing TTD by Charleston Comorbidity Index (CCI), revealed a trend of increasing TTD with increasing CCI score. Patients with a CCI of 0 had a median TTD of one day (IQR 1–5), whereas the median TTD among those with a CCI of 1–2 was two days (IQR 1–7), versus three days (IQR 1–8) among those with CCI of 3–4 and four days (IQR 1–10) among those with CCI of >4. A similar trend was seen among hospital survivors: those with higher CCI scores had longer median hospital LOS (Table 2).
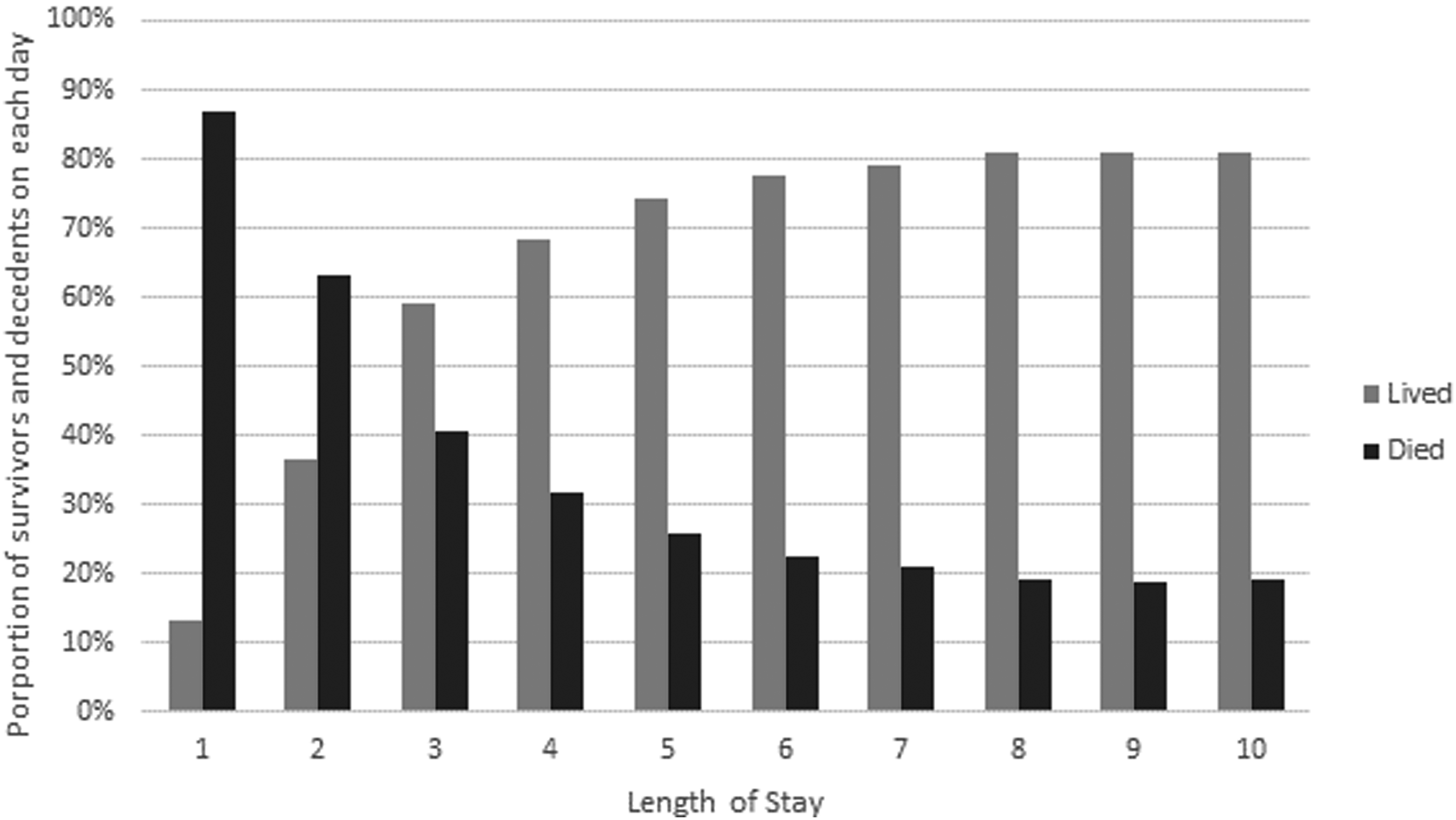
Survival outcomes each day after hospital presentation.
Discussion
In a large, nationally representative cohort of older adults undergoing emergent intubation and invasive MV, the median time from intubation to death was short; however, the length of time between intubation and death varied considerably depending on the principal diagnosis. Death after ED intubation is most likely to occur within the first several days, particularly among those with primary cardiopulmonary diagnosis, CVA, or sepsis, after which point, the probability of death is significantly lower. This information can help to shape family expectations after ED intubation.
We found that, among hospital decedents, age had little impact on median TTD. This finding is in keeping with previous studies, which have shown that, while age is a factor in intensive care unit (ICU) survival, it is not the primary determinant of mortality. 14 Interestingly, the extent of comorbid illness had a paradoxical relationship with TTD, whereby hospital decedents with higher CCI actually survived longer. Given the limitations of this administrative dataset, it remains unclear what is driving this phenomenon. It is unlikely that higher CCI actually confers a survival benefit. 15 It is possible that the paradoxical relationship between TTD and CCI is reflective of an unmeasured confounder of survival time among decedents, rather than an actual survival benefit conferred by increased CCI. 16 “Reversals” of association between risk factors and mortality have been well documented in other index-event cohort studies, and found to be attributable to collider bias and conditioning.17,18 This hypothesis is supported by the fact that overall increased CCI was associated with higher mortality. Another possible confounder may be a stronger preference for aggressive care among a small subset of patients with extensive comorbid disease burden. Further studies are required to evaluate this relationship.
There are several limitations to this study. First, use of a retrospective database limits our ability to understand the relationship between death and the decision to withdraw life-sustaining treatment (LST) and death. However, we know from previous studies that the majority of deaths in the ICU occur after the decision to withhold or withdraw LST, rather than a failure of LST itself.19–21 Thus, it is important for clinicians to understand this limitation when making inferences about prognosis. The natural history of respiratory failure treated with intubation and MV is necessarily different among hospital survivors and decedents. Future studies must explore these relationships further. Finally, this study is based on administrative data. As with all claims database research, our findings are vulnerable to misclassification bias due to coding inaccuracies and omissions.17,18,22
Conclusion
For older adults with serious illness, the decision to initiate MV is often fraught with uncertainty. The median time from intubation to death was short (three days); however, the length of time between intubation and death varied considerably depending on the principal diagnosis. Improved understanding of prognosis in the initial days after emergency intubation may help clinicians to mobilize additional support such as palliative care and provide families with more accurate anticipatory guidance.
Footnotes
Author Disclosure Statement
No conflicts have been disclosed.
Poster Presentation at American College of Emergency Physicians, National Assembly, 2018.