
Abstract
Abstract
Background:
People with heart failure (HF) have high morbidity and mortality and may benefit from palliative care (PC).
Objective:
To pilot a randomized, clinical trial of a PC intervention for people with HF.
Design:
Participants were randomized to usual care (UC) or intervention (UC plus specialty PC) between January 2012 and December 2013. The initial PC consultation was conducted in-hospital, with six additional contacts from the PC team over six months.
Setting/Subjects:
The study was undertaken in a large, urban, academic medical center with patients (n = 30) with New York Heart Association HF Class II–IV.
Measurements:
Patients completed a survey at baseline, three and six months, assessing pain, dyspnea, depression, and quality of life (QoL).
Results:
Although there were significant improvements in mean scores from baseline to six months for pain (4.3 vs. 2.4, p = 0.05), dyspnea (3.9 vs. 2.2, p = 0.03), and QoL (59.2 vs. 42.7, p = 0.001), there were no differences between study groups over time. On average, participants in the intervention group received 5 out of 6 contacts and were satisfied with the intervention.
Conclusions:
The intervention was well accepted by patients, safe, and feasible. Our findings suggest that PC interventions for people with HF should match the PC needs of the patient. Given the trajectory of HF, studies may need to recruit outpatients and follow patients for a longer period to fully evaluate the impact of PC interventions. Clinical trials Identifier: NCT01461681.
Introduction
Randomized clinical trials have demonstrated that patients receiving palliative care (PC) in conjunction with guideline-driven heart failure (HF) therapies achieve significant improvements in quality of life (QoL) and spiritual well-being, reductions in symptom burden, and greater completion of advance care planning documentation, when compared with patients receiving usual HF treatment.1,2 Despite these successful trials, there is a paucity of studies describing feasibility of PC interventions for patients with HF that can be invaluable for clinicians and researchers wishing to replicate studies and implement services. 3 We conducted a pilot randomized clinical trial to examine the feasibility of recruitment, randomization, retention, assessment procedures, and implementation of an interdisciplinary PC intervention (Symptom Management Service–HF [SMS–HF]) alongside standard cardiology care among patients with HF.
Methods
Study design
Patients with NYHA Class II–IV HF were randomized to either the SMS–HF group or usual care (UC). Surveys were administered at baseline, and at three- and six-month follow-up (Fig. 1).
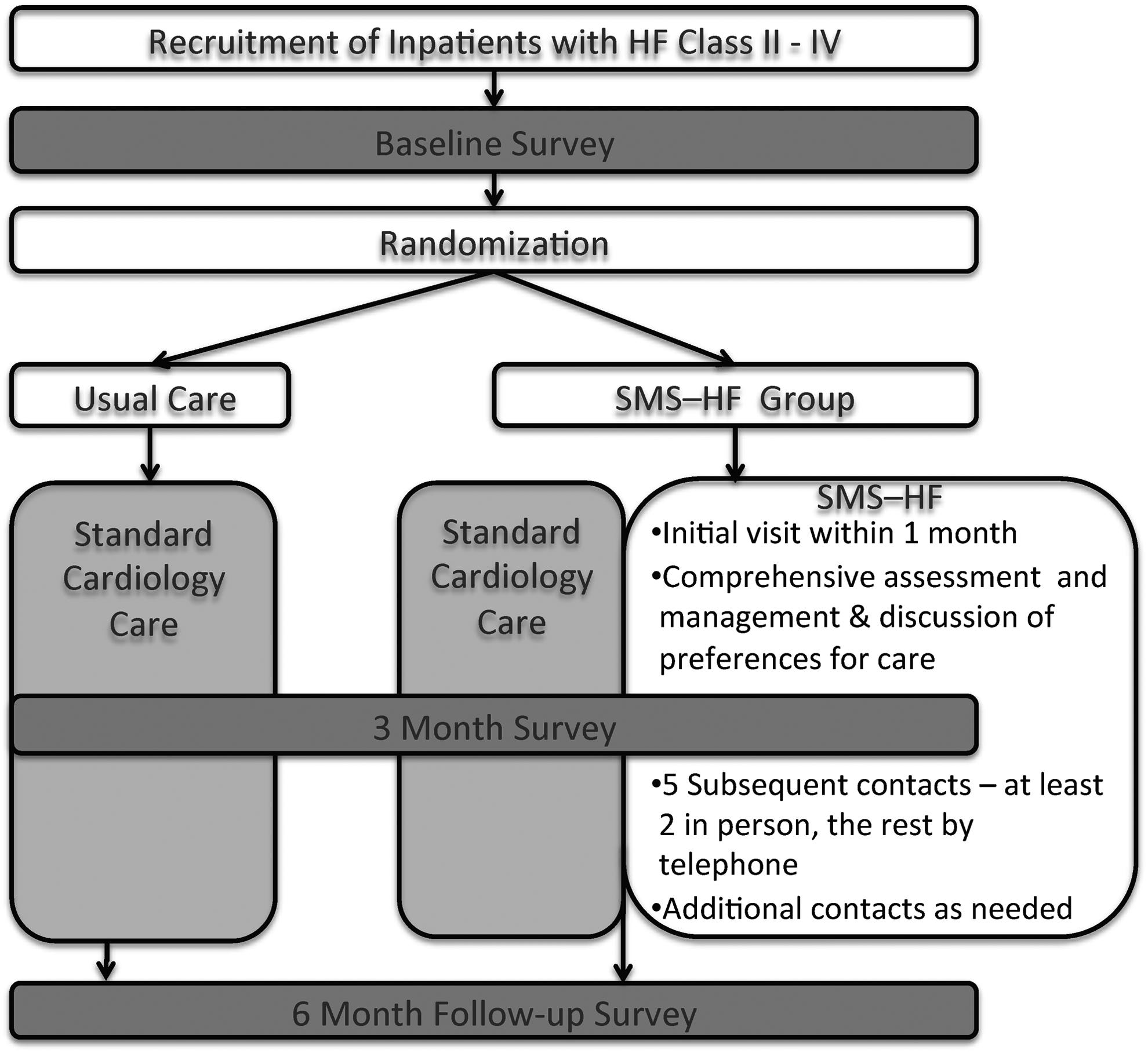
Study design.
Study setting
The study was undertaken between January 2012 and December 2013 in a large, academic medical center.
Participants
The inclusion/exclusion criteria for this study are outlined in Table 1.
Inclusion and Exclusion Criteria
HF, heart failure; PC, palliative care; SPMSQ, short portable mental status questionnaire.
Recruitment
We recruited inpatients with actively managed HF during the past six months. Patients were screened each day by conducting a review of new inpatient admissions to the medicine and cardiology services. The research coordinator contacted the patient's attending physician before approaching the patient to obtain informed consent. Once patients passed the short portable mental status questionnaire (SPMSQ), 4 they were randomized and completed the baseline survey. The study was approved by the UCSF Institutional Review Board (Study No. 11–06859) and registered with clinicaltrials.gov (Identifier: NCT01461681).
Intervention
Patients received intensive PC consultations provided by an interdisciplinary PC team (nurse practitioner, physician, social worker, and chaplain). The SMS–HF team provided direct care to the patient, prescribing medications for symptoms, discussing advance care planning, completing appropriate documentation, and providing psychosocial and spiritual support. 5 The first PC consultation occurred during hospitalization. Follow-up consultations included a one-week, in-person follow-up assessment and five monthly consultations, either in person (minimum 2) or teleconference. Additional contacts with the SMS–HF team were scheduled as needed. Patients who were re-admitted to the same hospital were followed by the inpatient PC team. We used electronic health record (EHR) templates to document in-person and telephone care, communicating recommendations to the cardiology team. We developed and used standardized, evidence-based protocols for symptom management.
Usual care
The patients randomized to UC received guideline-driven HF treatment.
Procedure
Study data were collected by using patient surveys and by review of the EHR.
Patient survey
The baseline survey was completed during hospital admission and took 30–35 minutes to complete. The follow-up surveys were mailed to all participants. Patients who did not return the survey after two weeks were contacted by telephone and declared nonresponsive after 5 attempts.
We collected demographic information (age, gender, ethnicity, marital status, income, educational level) and HF severity by using the NYHA Classification. 6 QoL was assessed by using the Minnesota Living with HF Questionnaire (MLHFQ), 7 and the Functional Assessment of Chronic Illness Therapy was assessed with the PC (FACIT-PAL) subscale. 8 Symptom-specific instruments included: the Brief Pain Inventory (BPI), 9 the Hospital Anxiety and Depression Scale (HADS), 10 the Edmonton Symptom Assessment Scale (ESAS), 11 The Brief Fatigue Inventory (BFI), 12 and the BORG scale for dyspnea. 13 Patients also rated their satisfaction with care.
Electronic health records
Assessment of HF etiology, ejection fraction, medications, documentation of advance care planning discussions, and number of readmissions during the six-month assessment period was obtained from the EHR. Advance care planning documentation included: identification of a surrogate decision maker, preferences for resuscitation, and advance care planning documents such as an advance directive or Physician Order for Life Sustaining Treatments (POLST) form.
Randomization
Patients were randomized within blocks of six to minimize potential bias and confounding. 14 A member of the research team with no contact with the study patients conducted a random assignment procedure to prevent any bias in the allocation to groups. 15
Statistical analysis
Descriptive statistics were used to examine the distribution of measures. Chi-square (χ2) analysis and analysis of variance examined bivariate associations. Change in outcome variables (QoL, depression, anxiety, pain severity, and dyspnea) repeated at baseline, three- and six-months, and differences between study groups were assessed by using linear mixed-effects models. This approach adjusts for sources of variation and correlation among repeated measures within a subject. Further, the analysis of repeated measurements ensures subjects with missing data can still be included. Confidence intervals and p-values were calculated for the overall average effects. An alpha of <0.05 determined statistical significance. McNemar tests were undertaken to compare responses to questions regarding patient satisfaction with care at baseline and at the six-month follow-up. The Statistical Package for the Social Sciences (SPSS) for Mac version 23 16 was used for all analysis. The statistician was blinded to group coding.
Results
Patient characteristics
Overall, 1757 patients were screened for eligibility between March 2012 and March 2013, of whom 117 were eligible and 39 were enrolled (33% participation rate) (Fig. 2). Patients were randomly assigned to UC (n = 17) or intervention (n = 22). Three patients in UC and six patients in the intervention group dropped out. A total of 30 patients (14 patients UC and 16 intervention) completed follow-up surveys.
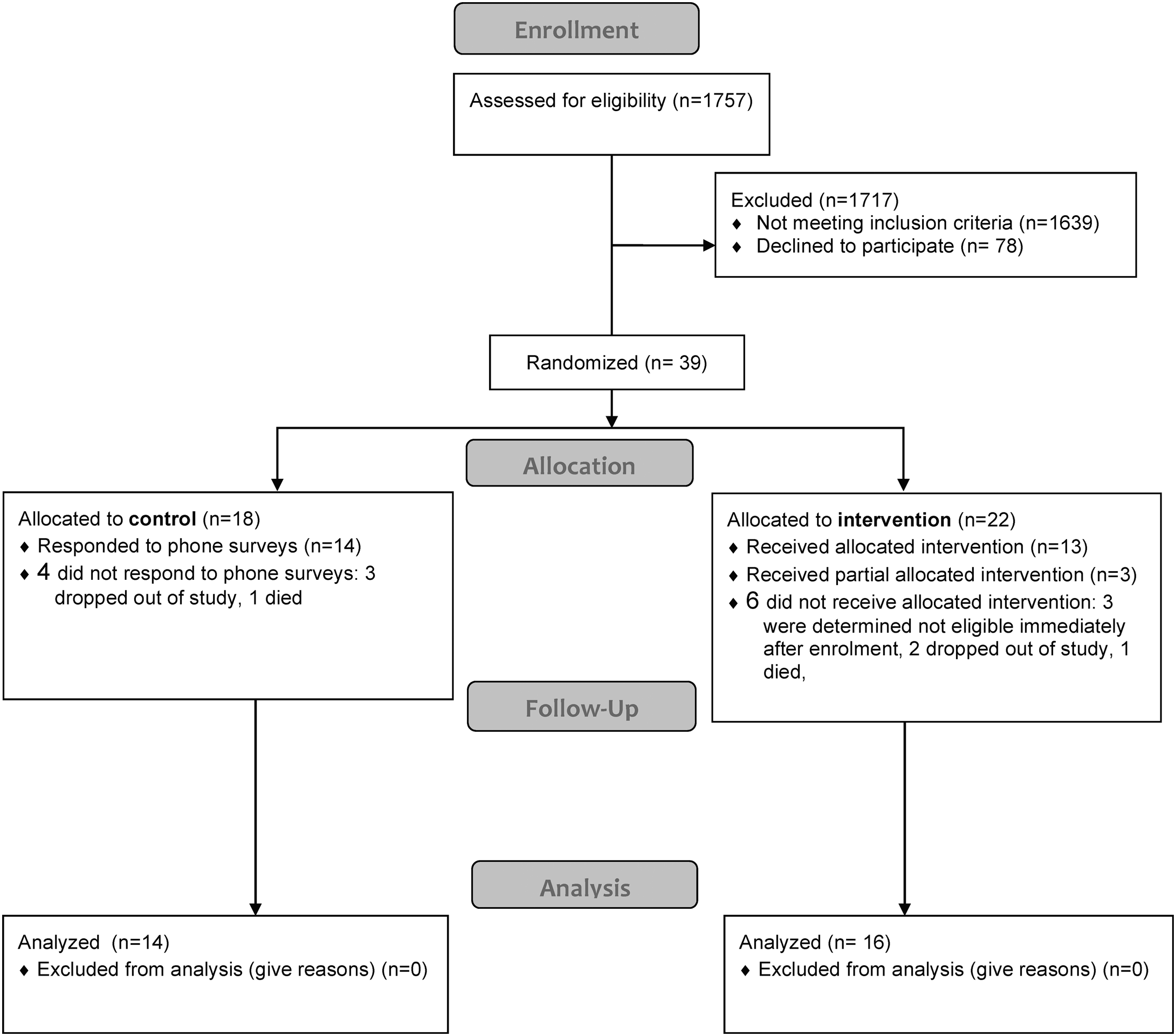
Consort flow diagram.
Patients were 65 years of age, 16 were men, 13 were white, with self-reported NYHA Class I (n = 7), II (n = 9), III (n = 11), or IV (n = 3). Patients had been living with HF for nine years, and 10 had a mean ejection fraction >50%. The intervention group had significantly more women than the UC group (69%, n = 11 vs. 28%, n = 4; p = 0.03) (Table 2).
Participant Characteristics
SD, standard deviation.
Prescribed medications and guideline-driven heart-related therapies
There were no differences between the two study groups in terms of guideline-driven HF therapies received or medications for other conditions (Table 3).
Medications (Prescription and Over the Counter) Included in the Medication List of Patients
CRT, cardiac resynchronization therapy devices; NSAIDs, non-steroidal anti-inflammatory drugs.
Clinical outcomes
At baseline, there were no differences between the UC or intervention groups for heart-related QoL (p = 0.9), QoL (p = 0.2), depression (p = 0.4), anxiety (p = 0.4), pain severity (p = 0.7), and dyspnea (p = 0.4).
Patients in both groups reported improvements in all outcomes except depression across the three assessment periods: heart-related QoL (p = 0.001), QoL (p = 0.03), anxiety (p = 0.003), severe pain (p = 0.05), dyspnea (p = 0.03), and depression (p = 0.15) (Table 4). There were no differences between the two groups over the course of the study.
Change in Symptom Scores from Baseline, Three-Month, and Six-Month Assessment between Usual Care and Intervention Groups
Examines the overall means between the two interventions.
Examines the interaction between the “Intervention Group” by “Month.”
Higher score reflects a poorer QoL.
95% CI, 95% confidence interval; FACIT-PAL, Functional Assessment of Chronic Illness Therapy with the PC; MLHFQ, Minnesota Living with HF Questionnaire; QoL, quality of life.
Intervention adherence
The 16 patients involved in the intervention received on average 5 of the 6 components of the intervention (range: 1–6, Table 5). Nine patients received additional consultations (range: 1–4).
Components of the Intervention Received by Patients on the Symptom Management Service–Heart Failure Group (0 = No, 1 = Yes)
In person.
Hospital consultation.
Discontinued participation.
AD, advance directives; POLST, Physician Order for Life Sustaining Treatments.
Spiritual assessment and advance care planning documentation
All patients in the intervention group received a spiritual assessment. At the completion of the study, eight (50.0%) intervention group patients had advance care planning documentation and one completed a POLST form (Table 5). In contrast, only three (21.4%) patients receiving UC had advance care planning (ACP) documentation. However, this difference between the study groups was not significant (χ2 = 0.2, p = 0.15).
Satisfaction with care
Patient satisfaction with the care they received was documented at the initial assessment as well as during three- and six-month follow-up assessments. We found no difference in satisfaction with care between the two study groups at any of these three assessment periods.
Discussion
Patients hospitalized with HF had mild-to-moderate symptoms at baseline and were able to report symptoms and QoL throughout the six-month assessment period regardless of study group. Although it was time consuming for patients to complete the surveys and engage with the PC team, the intervention was acceptable to patients and feasible.
This trial provided additional information to inform future studies and service development, especially given PC workforce shortages. For example, some patients who were documented to have NYHA HF Class II at time of screening reported only NYHA HF Class I at initial assessment and many improved significantly by discharge and may not have needed an intensive, six-month PC intervention. Although patients had poorer QoL and symptom scores at baseline, most participants reported improvements. It is important to target the right patients for a specialty PC intervention that is tailored to their needs. We developed a standardized intervention that was comprehensive and intensive, which may not have been necessary for all patients. Matching PC interventions to patient need, including primary PC, might be more appropriate. Though more challenging to implement, given the trajectory of HF, a longer follow-up period may be needed to fully evaluate the impact of the PC intervention. Our six-month follow-up, which was practical for our pilot study, seemed too short to assess the full impact of advance care planning, long-term symptom management, and psychosocial and spiritual support.
Our survey relied on self-report, resulting in potential error associated with poor recall. 17 We attempted to mitigate poor recall by assessing the cognitive capabilities of each patient. As a result, many of the sickest patients who might have been more likely to benefit were excluded. Future studies may consider getting consent and assessing outcomes from surrogates or using outcome measures based on observation rather than patient report. Our survey was long, which may have increased responder burden, particularly for sicker patients. Reducing the number of items or using short-form instruments may mitigate this burden. Given the small number of participants, there was an imbalance of randomization. There were more women and a greater proportion of patients were on ACE-I/ARB and pain medications in the intervention group. Future studies may need to use block randomization to ensure equal allocation across these characteristics and adjust for these between-group differences in multivariate modeling.
Specialty PC has limited availability. Therefore, it is important to find the “sweet spot” where specialty PC significantly improves patient care and to know where PC needs can be met by the patient's other clinicians and system-wide interventions as for advance care planning. The importance of providing PC for patients with HF is becoming increasingly recognized as an invaluable resource and proven in clinical trials. 18 Feasibility studies such as the one described in this article can inform future studies and guide clinical service implementation.
Footnotes
Acknowledgments
The authors would like to thank the National Palliative Care Research Center and the Alafi Family Foundation for funding this study. They thank the patients, primary care physicians, cardiologists, and nurses for their involvement and for allowing them to recruit patients. They would also like to thank the specialist PC team for their commitment to this project. This study was registered with ![]() (Identifier: NCT01461681). Funding was provided by the National Palliative Care Research Center.
(Identifier: NCT01461681). Funding was provided by the National Palliative Care Research Center.
Author Disclosure Statement
No competing financial interests exist.