
Abstract
Background:
Specialized home-based palliative care (HPC) services aim at reducing the number of visits to emergency departments (EDs) and hospitalizations at end of life. In addition, it offers patients the possibility to die at home.
Objective:
To investigate whether the last years' expansion of palliative care in Stockholm County, Sweden, reduced the health care resource use and/or increased the number of patients who died at home.
Design:
This is a population-based study of all registered 2780 patients referred to HPC in 2015 in the Stockholm region. The majority of the patients (2087) had cancer, but 693 patients had chronic medical illness, most often cardiovascular and pulmonary diseases.
Results:
HPC reduced visits to the ED and hospital admissions by 51% and 41%, respectively. The number of hospital admissions to the departments of oncology, medicine, and surgery was reduced, whereas admissions to palliative care units increased. For the 1773 patients alive after 90 days with HPC, the number of days spent in hospital reduced from 19,628 before HPC to 13,743 (30%) days with HPC. The most common place of death was at a specialized palliative care unit (48%), whereas 36% died at home.
Conclusions:
HPC reduced emergency health care resource use for the majority of patients, despite patients having progressing disease. To improve the quality of end-of-life care, we need to make early integration of palliative care available for a larger number of patients. In addition, we have to improve care pathways, especially for patients with gastrointestinal and lung cancer, who continued to be frequently admitted to hospital.
Introduction
In Sweden, there has been an increase in the number of specialized home palliative care (HPC) services, as a result of the past decades of changed health care system with reduced number of hospital beds and increased facilities of outpatient care also for patients in late palliative phases. 1 In Sweden, HPC started in the 1970s, focusing on malignant diseases. The majority of patients receiving HPC are still patients with advanced cancer. However, patients with congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), and neurological chronic conditions, such as amyotrophic lateral sclerosis and multiple sclerosis, are increasingly palliated at home. Specialized home-based palliative care teams in Sweden consist of doctors, nurses, assistant nurses, physiotherapists, nutritionists, and counsellors who care for patients in their homes, around the clock, and work separately from the primary care. Many organizations that offer care by HPC teams have their own specialized palliative ward, not equivalent to a hospice that is uncommon in Sweden, but a ward where patients can receive end-of-life care until death like at a hospice or stay for shorter periods for symptom relief. According to literature, patients prefer to receive advanced care at home, especially near the end of life and, if possible, many wish to die in their home.2–4 Furthermore, a Cochrane review showed an increased proportion of deaths at home with HPC. 5
How to measure cost-effectiveness and quality of HPC is an ongoing debate. Multiple visits to the emergency department (ED), hospital admissions, and death in an acute care institution have all been suggested as indicators of poor quality of care for patients with advanced cancer.6,7 According to a recently published review, there was no strong evidence for reduced need of emergency care for patients receiving palliative care, regardless of whether they received palliative care at home, in hospital, or at an outpatient clinic. 8 In contrast, others report HPC for terminally ill cancer patients to increase the number of patients dying at home, in addition to reducing both the number of patient visits to the ED and the number of hospital admissions.3,5,9,10 Furthermore, according to several studies, HPC increased patients' satisfaction, significantly reduced patients' symptom burden, and reduced costs compared with standard care.3,9,11–13
Our primary aim was to explore the impact of past years integration and expansion of HPC services in the Stockholm area in relation to palliative patients' use of emergency care, in-house care at an emergency hospital, and place of death.
Materials and Methods
We included all patients (n = 2780) cared for by HPC from January 2015 to December 2015 in the Stockholm County Council with a total of 2.2 million citizens; ∼23% of the Swedish population lives in Stockholm. 14 Cancer was the most common diagnosis (n = 2087), whereas 693 patients had other chronic medical conditions such as CHF, COPD, and neurological disorders.
Through record linkage using the patients' personal identification numbers, we collected data of all health care use registered in patient administrative systems for these patients during 90 days with HPC compared with 90 days before HPC. Health care data before and during HPC were analyzed for the total study cohort, but also separately for patients alive after 90 days, n = 1773. Outpatient care was summarized as number of visits to a doctor. For survival estimations shown in Figure 1, we calculated the number of days from the start of HPC until death or the latest mid-July 2016. We used a period longer than 90 days for survival estimations to make sure the trends in survival analysis based on age, gender, diagnosis, and income and education remained the same over a longer period of time. The longer time period until mid-July 2016 was also used for the analysis of place of death.
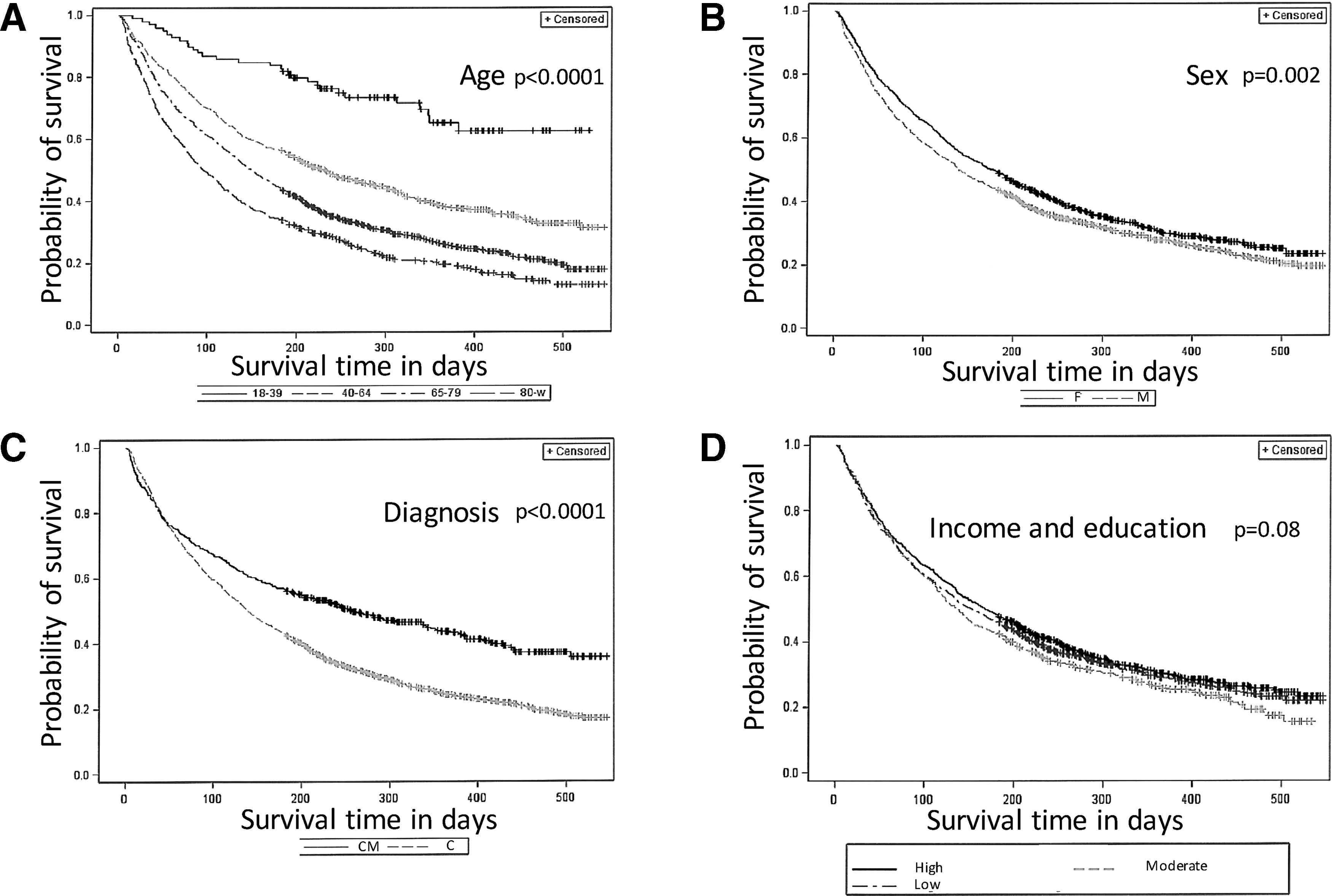
Survival estimates in the total population of 2780 patients in relation to
Results
The population of Stockholm County Council contains ∼50% men and 50% women, which is in concordance with our study cohort. With regard to age, the study cohort included older patients. No differences in the distribution of people/patients with high, moderate, and low income and education were found between our study cohort (high 43%, moderate 18%, and low 39%) and the general population in Stockholm (high 45%, moderate 18%, and low 36%). The HPC population cohort (n = 2780) consists mainly of people ≥65 years, and there are approximately as many men as women, regardless of the diagnosis (chronic medical illness or cancer). During the first and second months with HPC, 15% and 12% of the patients died, respectively, each month, and a further 9% died during the third month. Patient characteristics are summarized in Table 1.
Characteristics of the 2780 Patients in the Stockholm County Council Admitted to Home Palliative Care Service from January 2015 to December 2015 in Total, and in Relation to a Diagnosis of Cancer or Chronic Medical Illness
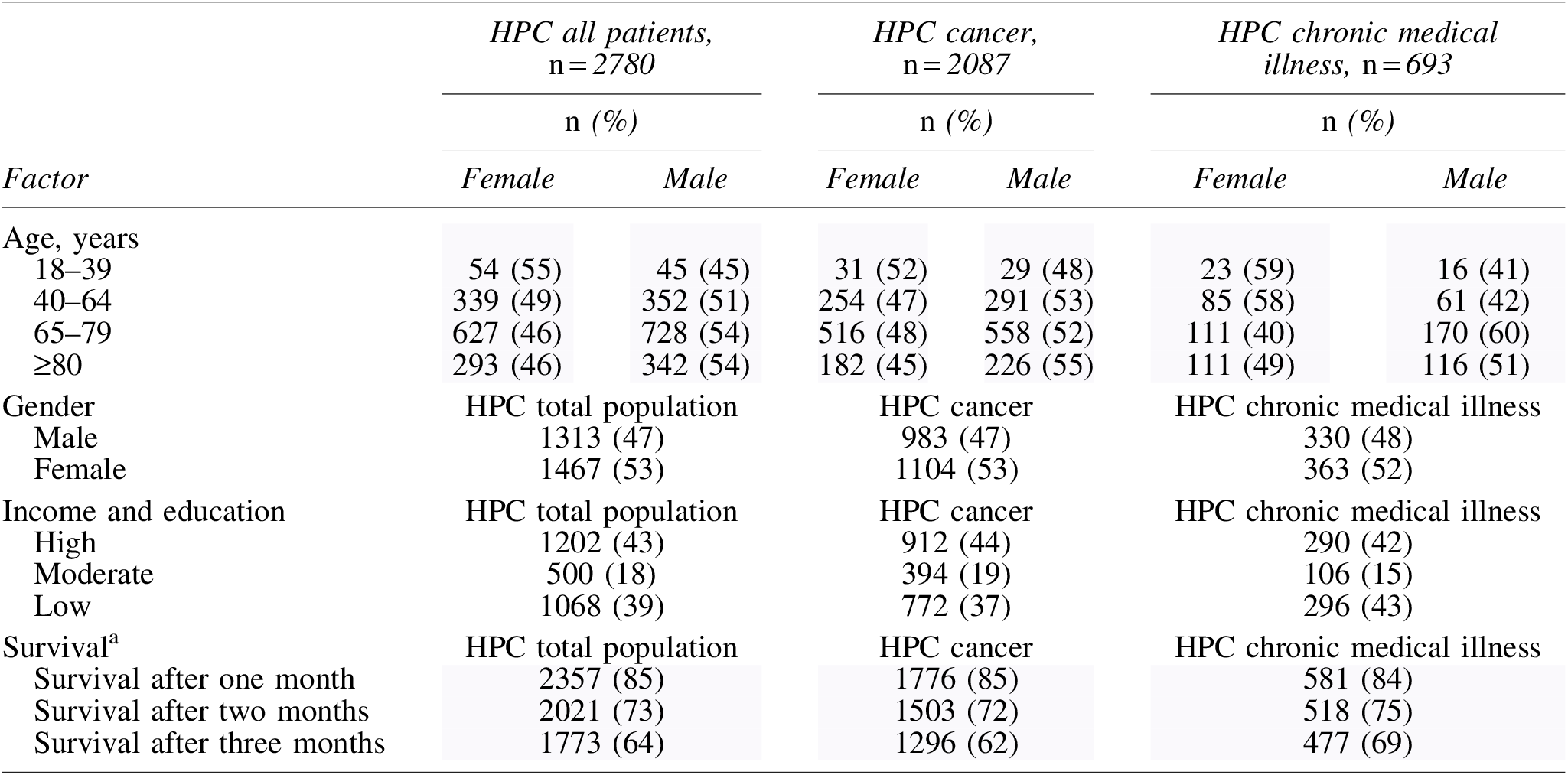
Survival from start of HPC to death or March 31, 2016.
HPC, home palliative care.
ED visits
For patients, who were alive 90 days after admission to HPC (n = 1773), the number of visits to the ED was reduced from 2188 to 1071 (51%). The number of ED visits per patient varied between 1–32 before HPC compared with 0–10 visits per patient during HPC. The difference before and during HPC was statistically significant for both subgroups (chronic medical illness and cancer; p < 0.001). The number of patients in need of ED visits got reduced by 59% for patients with chronic medical illness and by 46% for cancer patients. In an analysis stratified for diagnosis and gender, women reduced their need for ED more than men (Table 2).
Outpatient Care for 1773 Patients Alive After 90 Days with Home Palliative Care (HPC) at Emergency Department, Specialist Care Outpatient Clinic, and Primary Care during 90 Days before and during HPC
ED, emergency department; HPC, home palliative care.
Outpatient care
Ninety days before HPC, patients had generated 4975 visits to a specialist outpatient clinic compared with 3097 visits during HPC.
A major reduction in specialist care visits during HPC was found for patients with both chronic medical illness and cancer, especially for women (Table 2). The reduced number of visits to primary care was the major change for all palliative patients (Table 2).
Inpatient care
The number of hospital admissions in total markedly reduced during HPC for the departments of oncology, surgery, medicine, and specialized palliative care. The 1773 patients in our study who lived through 90 days with HPC were admitted to hospital 2789 times during the time period before HPC compared with 1649 times during the following 90 days with HPC, a reduction of 41% (Table 3).
Admissions to Hospital Wards at Departments of Oncology, Surgery, Medicine, and Specialized Palliative Care Units 90 Days before and during Home Palliative Care for 1773 Patients Alive after 90 Days with Home Palliative Care
HPC, home palliative care.
Similarly, the days in hospital got reduced by 30%—19,628 days during 90 days before HPC compared with 13,743 days with HPC (Table 4).
Inpatient Care for the Number of Days Spent at Departments of Oncology, Surgery, Medicine, and Specialized Palliative Care Units 90 Days before and during Home Palliative Care Service (HPC) for the 1773 Patients Alive after 90 Days with HPC
Men with chronic medical illness had the major reduction in the number of hospital admissions (56%), but women (43%) having chronic medical illness in addition to men (35%) and women (40%) having cancer also had significantly fewer hospital admissions with HPC (Table 3).
For patients with cancer, the number of inpatient care days at an oncology ward got reduced by 42% for women and by 31% for men. Similarly, days spent in the department of surgery or medicine for cancer patients got reduced by 51%–60% (Table 4). However, the number of patients admitted for inpatient care and days spent at a specialist palliative care unit increased during HPC compared with before (Tables 3 and 4).
Common diagnosis during hospital admissions
The five most common diagnoses for hospital admissions 90 days before the patients were accepted for HPC were tumors, diseases of the circulatory system, respiratory diseases, unspecified symptoms, and diseases of the gastrointestinal tract. During HPC, cancer was still the most common diagnosis for hospital admissions, especially gastrointestinal and lung cancer.
For patients with a chronic disease, who are in need of hospitalization, the most common diagnoses were cardiovascular disease and chronic pulmonary disease.
Survival
From start of HPC to the date of death or 90 days after the last inclusion date, December 31, 2015, the median survival time for the 2780 patients was 154.5 days. Older age (p < 0.0001), male gender (p = 0.002), and cancer diagnosis (p < 0.0001) were associated with shorter survival times compared with younger patients, women, and diagnosis of a chronic medical illness (Fig. 1). Median survival time for men was 139 days; that for women was 176 days. For cancer patients, median survival was 139 days, whereas it was 214 days for patients with chronic medical illness. For a combined factor of income and education (when separated into three groups with low, moderate, or high income and education), there was no difference in survival (p = 0.08).
Place of death
Of the 2780 patients admitted to HPC in 2015, 36% (1007) died during the study period of three months. We analyzed the 2780 patients from January 1, 2015 to March 31, 2016 to generate at least three months of follow-up for all patients. During this period, 386 patients (56%) with chronic medical conditions died, whereas 1555 (75%) of the cancer patients died (Table 5). Regardless of diagnosis, the majority of patients (50%) died at a specialist palliative care unit. Approximately one-third of the patients died at home (36%), whereas 14% died in hospital.
Place of Death for the 1941 Patients in the Cohort of 2780 Patients Receiving Specialized Palliative Care at Home in 2015 in the Stockholm Region
Discussion
Main findings
This is the first large Swedish study of the impact of integrated HPC on health care resource use, survival, and place of death. The number of patient visits to the ED and admissions to hospital significantly reduced during HPC, despite the fact that the patients had progressing diseases. In addition, although days in the specialized palliative care units increased, total overall days of hospitalization were reduced.
Our data are in agreement with other studies reporting approximately 40%–50% reduction in emergency care in addition to fewer and shorter hospital stays for patients with HPC versus standard care.15–17 The results may be explained by a reduction in symptom burden for patients during HPC, as previously reported in a Cochrane review. 5
Patients with gastrointestinal and lung cancer continued to be frequently admitted to hospital in our study. For this group of patients especially, we need to further investigate the cause of hospital referrals to improve palliative care. A possible explanation is that a few patients with a rapidly worsening disease are often too difficult to palliate at home, whereas the majority are well cared for at home without need for ED visits nor hospital admissions.
Delgado-Guay et al. 18 showed that nearly one of four ED visits by cancer patients, who receive outpatient palliative care, could probably be avoided. There are several possible explanations to why a patient with HPC is in need for transport to hospital. For example, complex pain interventions such as insertion of an intrathecal catheter, surgery of fractures, and sometimes confusion and anxiety require hospital care. The patients' well-being and safety at home with HPC often require support from family and friends, as well as from community services. 19 HPC can be hard on the family, as it substantially limits privacy and time to rest.
Home-based specialized palliative care teams work with a holistic perspective round the clock, which include the best palliation of both physical and psychological symptoms in addition to planning of end-of-life care with patients and relatives. The care teams also interact with patients, for example, oncologist or cardiologist at the hospital, for optimized integration of disease-specific care and palliative care. Other members of the patients' family may also receive counseling if they want to, which also include help to apply for financial support if needed. Altogether, better symptom relief and easier access to guidance, counseling, and assessments may explain the reduced need of emergency care and hospital admissions during HPC in our data. However, one limitation with our study is that we have no control group, why we cannot exclude the possibility that patients with progressing disease use less emergency care even if they do not have access to specialized palliative care at home.
Some say HPC is cost-effective9,20 and some say it is not. 8 The costs of community services and lost salary for relatives/friends would approximately double the cost of HPC.21,22 Other studies have estimated an overall reduction in health care cost, including costs for visits by HPC. 15
In 2007, Brumley et al. 9 reported lower costs and higher satisfaction with HPC compared with traditional care. In this randomized study, patients suffered from chronic heart failure, COPD, and cancer. They showed more than a 50% reduction in costs for health care ($213/day vs. $95/day) due to 56% fewer visits to the ED and decreased time in hospital wards. 9 However, HPC is differently organized internationally, why studies of cost-effectiveness are difficult to apply from one country to another. In Stockholm, ∼6 per 10,000 over the age of 55 years have access to HPC, according to a 2011 report. 23
Another limitation with this study is that it is a retrospective study and only covers HPC in the Stockholm region, not the whole country. In addition, we have no knowledge of the patients' desired place of death.
Dying at home is often suggested to be a hallmark of good palliative care. However, the hallmark for good quality of care should preferably be the capacity to meet the patient's choice with regard to the place of death, rather than the actual place of death. We know from previous studies that one of the major prognostic factors for dying at home is not living alone. 24 Other factors of importance for place of death are physician home visits, but also socioeconomic factors.25,26 Despite HPC, a minority in our cohort of 2780 patients died at home, which is in concordance with recently published data of place of death for cancer patients in Sweden. 26
In Sweden, health care is mainly financed by taxes, which is why we expect health care outcomes and resource use not to be associated with sociodemographic factors. However, inequalities related to social support27,28 and education level have been found for colorectal cancer and chronic medical conditions.27–29 We found no differences in survival related to a combined factor of income and education. However, patients of older age and male gender had shorter survival times in our population.
Despite the number of HPC services increased in the past years in Sweden, public awareness of palliative care remains limited. 30 More information to patients, carers, and people in general should be provided in addition to more research to improve end-of-life care.
Conclusions
HPC improved the quality of care for this population-based cohort in a late palliative phase, with reduced need for emergency care and hospital admissions. The majority of patients under HPC die at a specialized palliative ward and not at home. More research into the factors with possible impact on the desired place of death in addition to studies of prognostic factors relating to a continuous need for emergency care and hospitalization during HPC is needed.
Footnotes
Acknowledgments
We thank Fredrik Sandlund, the former head of ASIH Stockholm Södra, who supported the project from start, and Erica Brostedt for linguistic revision.
Author Disclosure Statement
The two authors have no conflict of interest to declare. We received no particular funding for this project, and we have full control over all the data, which may be made available for review upon request.