
Abstract
Abstract
Advanced heart failure (HF) is a common condition that leads to significant suffering for patients and their families. Left ventricular assist devices (LVADs) can improve both the quantity and quality of life for those suffering with advanced HF. Palliative care clinicians are being asked with increasing frequency to assist HF teams to manage patients with LVADs in the preimplantation, post-operative, and end-of-life settings, although not all palliative care providers feel comfortable with this technology. Written by specialists in HF, geriatric cardiology, and palliative care, this article seeks to improve palliative care providers' knowledge of LVADs and will prepare palliative care teams to counsel and support LVAD patients and their families from pre-implantation to the end of life.
Introduction
Heart failure (HF) affects millions of patients worldwide. Some patients eventually progress to an advanced phenotype referred to as Stage D HF, defined as “advanced HF with continued HF symptoms requiring aggressive medical therapy.” 1 A subset of these patients may benefit from left ventricular assist devices (LVADs). LVADs are used primarily for two indications: (1) as bridge-to-transplant in patients who may eventually go on to receive a heart transplant or (2) as destination therapy (DT) in patients ineligible for or uninterested in transplantation. While LVADs were initially approved for patients awaiting heart transplantation, LVAD as DT has improved HF-related mortality since 2001, 2 with FDA approval since 2010. The vast majority of patients receiving LVADs in the United States are as DT.
Patients with LVADs frequently have multimorbidity resulting in significant symptom burden, often including LVAD-related complications. Therefore, these patients may benefit greatly from palliative and supportive care. Recognition of these needs led to the requirement by CMS to include palliative care specialists as part of the interdisciplinary LVAD team. 3 Given how complicated the care of patients with LVADs can be, we assembled a group of experts in HF, geriatric cardiology, and palliative care to develop a list of high-yield tips for palliative care clinicians taking care of patients with LVADs, focusing primarily on the DT population.
Tip 1: LVADs Can Change Patients' End-of-Life Experiences as They Approach Death
LVADs increase survival in patients with advanced HF. However, LVADs alter the pathway that patients take as they approach end of life. For patients with advanced HF, death is often due to progressive pump failure or, less commonly, due to a lethal arrhythmia. Over time, the incidence of sudden cardiac death has improved dramatically with medical therapy and implantable cardioverter defibrillators; therefore, progressive pump failure has been the most common mode of death. 4
While worsening HF can still occur in patients with LVAD, their clinical course is commonly impacted by complications of LVAD therapy (Table 1). Almost three-quarters of LVAD patients will have a major LVAD complication within the first year after implantation. These include stroke, gastrointestinal bleeding, right ventricular failure, and LVAD thrombosis and infection. In a cohort of patients with DT-LVAD, four common trajectories were observed: (1) ∼10% of patients experienced early complications within 90 days of LVAD implantation; (2) 20% experienced persistent cardiac or multiorgan complications with recurrent hospitalizations and death; (3) 40% of patient experienced improved quality of life, but suffered a major complication (i.e., stroke or device complication) that lead to an acute death; and (4) 30% experienced improvement in overall functional status, only to be followed later by a terminal decline due to a life-limiting illness or abrupt decline. 5 With these trajectories in mind, palliative care clinicians may be consulted to assist with care of patient with DT-LVAD at a variety of decision points (Fig. 1).
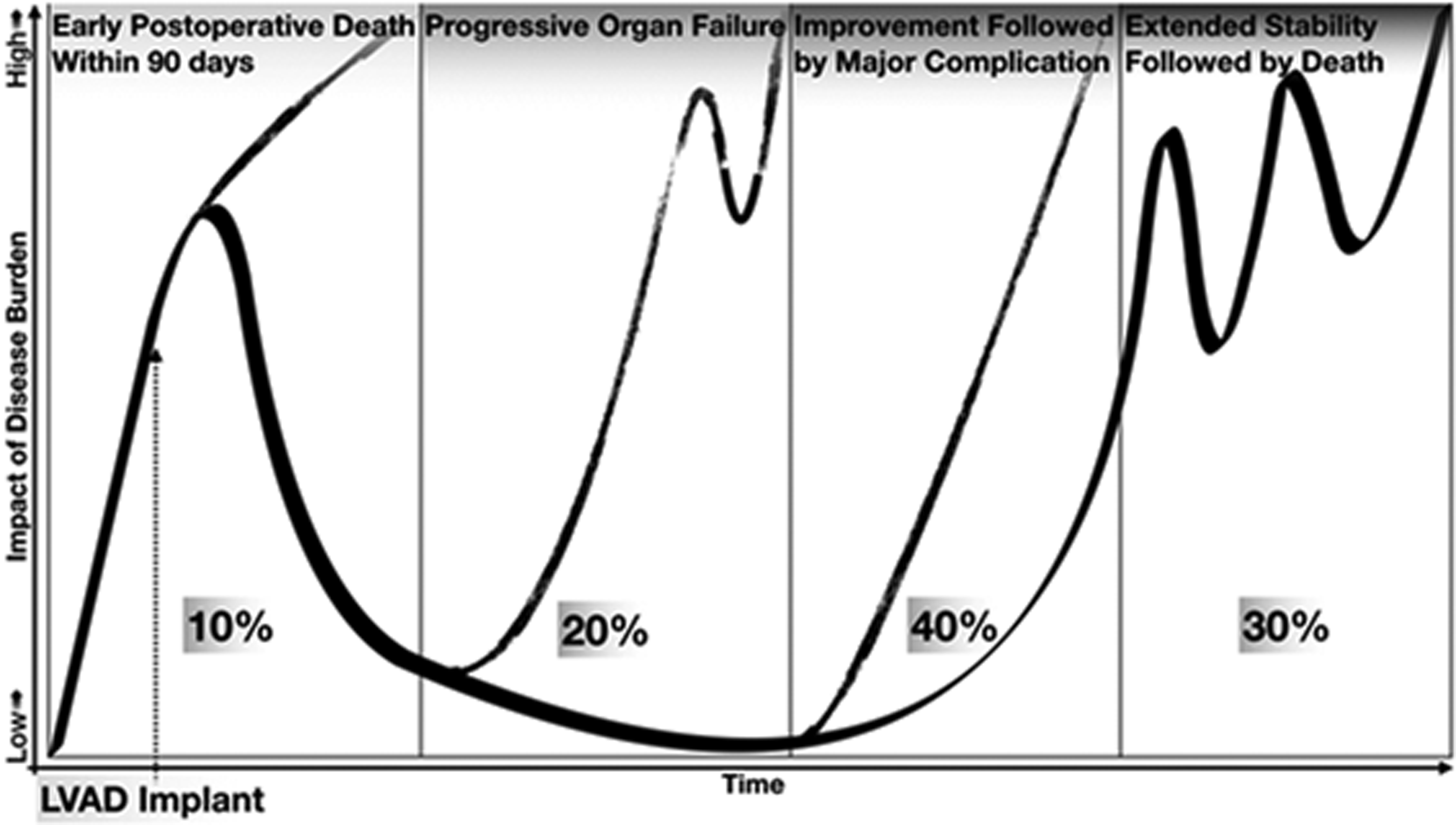
The schematic shows the different trajectories experienced by patients undergoing destination therapy LVAD implantation. Proportions of patients experiencing the categorized outcomes are derived from Dunlay et al. 5 LVAD, left ventricular assist devices.
Survival and Complications Associated with Commercially Available Left Ventricular Assist Device Pumps
Data from ENDURANCE and MOMENTUM 3 trials. Right HF defined as need for right ventricular assist device, or inhaled nitric oxide or inotropes for >1 week.
BTT, bridge-to-transplantation; DT, destination therapy; GIB, gastrointestinal bleeding; HF, heart failure.
Palliative care providers should be familiar with common LVAD complications such as driveline infections and the need for inotropes for persistent right ventricular failure as well as complications, including bleeding and stroke. Palliative care providers are often consulted to discuss quality of life, and the discussion does not routinely move to end-of-life discussions.
Tip 2: Palliative Care Consultation Before LVAD Implantation Can Both Meet Credentialing Requirements and Offer Patients and Families a Clear Opportunity to Define Acceptable and Unacceptable Quality of Life
Many patients with advanced HF and their caregivers can benefit from a consultation with a palliative care clinician; however, the nuances of LVAD-associated implantation and aftercare are particular and complex. Despite DT meaning that the patient will have the device for the remainder of their life, understanding how a patient wants to live and eventually die is important to explore. Understanding “what matters most” to the patient regarding hopes for life and their goals of care with the device is critical, as well as gaining a deeper appreciation of what states of living are unacceptable for the patient. While death is the eventual end for patients with LVAD, it is important to focus on how people will live as fully and able up to that point. Despite the vague mandate for palliative care involvement in LVAD-related care, it is important to consider palliative care more than as just a box to be checked off. However, finding the optimal time to have discussions in the period approaching surgery is difficult as patients have many preimplantation studies that need to be completed, and patients tend to be very sick and struggle to remember details of such discussions at later points.
Palliative care providers should understand that the goal of a palliative care consultation can vary from providing quality-of-life support to helping patients and family members cope with the ultimate finitude of all patients with DT-LVAD. However, providers need to approach the preimplantation consult as a targeted advance care planning intervention, not a discussion about code status or focusing on comfort care only. Families often do not know “what the loved one wants” and facilitating some discussion about the common scenarios encountered can arm patients and surrogates for future discussion. At a minimum, health care power of attorney documents should be completed preoperatively. Living wills may be included, but it should be noted that patients with LVAD often die of complex multimorbidity. They usually do not spend time in a vegetative state, but are often are incapacitated to some degree. Appreciating that a time may come when the “device may be working, but the body is failing” may be helpful to frame the discussion.
Tip 3: Medical Therapy in LVAD Patients Is Very Important Since It Can Reduce Risk of Stroke and Worsening HF Symptoms
While LVADs can provide a dramatic increase in cardiac output, medical management remains crucial in these patients to prevent stroke and other symptoms. 6 Given lack of pulsatile flow, the blood pressure in patients with LVADs is assessed by the mean arterial pressure. A goal of <90 mm Hg is necessary to reduce risk of stroke, as is systemic anticoagulation, chronically, with warfarin. 7 Many patients with LVAD benefit from treatment with HF medications such as angiotensin-converting enzyme inhibitors and beta blockers. 6 Therefore, many palliative care consults in this population should not focus on stopping nonessential medications to focus only on comfort medications; rather, cardiac medications should be maintained since they tend to improve HF symptoms and quality of life.
Tip 4: To Explain LVADs and Their Natural History, Clinicians Can Adapt Language from Cancer
By and large, patients and their clinicians are much more familiar with diseases such as cancer, and therefore, HF specialists have developed a framework under which the course of LVAD therapy can be explained to patients. Complications of LVAD therapy (e.g., infection, stroke, and bleeding) can be framed as complications of chemotherapy; development of right ventricular failure can be thought of as progression of underlying disease; the development of aortic insufficiency, which can lead to redundant flow, can be framed as mutation of the disease, which may require surgery by oversowing the aortic valve, adjustment in LVAD speed, or implantation of a transcatheter aortic valve; and worsening end-organ dysfunction or development of HF symptoms can be considered failure of therapy. Such language could be used to explain the course of LVAD therapy in ways that patients can grasp and is more comfortable for palliative care clinicians comfortable in the oncology realm, but relatively less confident about cardiovascular diseases.
Tip 5: Patients with LVADs Have Limited Options for Facilities Aside from the Implanting Center Equipped or Credentialed to Manage Their Care
Patients with LVADs often have very limited options with regard to facilities that are willing or able to manage care for someone with an LVAD. In the community, many skilled nursing facilities, outpatient hemodialysis facilities, and inpatient hospice facilities lack staff who are credentialed in and comfortable with caring for LVADs. In the hospital, patients with LVADs are often not able to be adequately cared for in noncardiac ward units, palliative care units, inpatient psychiatric wards, or smaller hospitals that are not comfortable or credentialed to manage LVADs. This limitation in venues of care is an issue that is of particular importance for patients considering LVAD therapy and should be brought up before implantation since many patents would consider being confined to a cardiology floor of a hospital or cardiac intensive care unit for the duration of their lives as an unacceptable quality of life.
Tip 6: Turning Off an LVAD Is Not Assisted Death and Does Not Have to Occur Only in the Hospital
The decision to turn off an LVAD can be weighty for patients, caregivers, and the medical staff, given how quickly patients tend to die after deactivation. Some clinicians may conscientiously object to LVAD deactivation, conflating it with aid-in-dying. 8 However, withdrawal of LVAD support was not found to raise ethical issues that differed from discontinuing ventilator or pacemaker support. 9 In LVAD deactivation, the cause of death is the underlying HF syndrome and not the act of deactivating the device. Although surveys suggest not all clinicians are universally comfortable with LVAD deactivation, the reason for this discomfort is often the context of the deactivation, rather than the procedure itself.10,11 Decisions regarding deactivation are simpler when LVAD patients have a concurrent terminal illness or conditions from which they will not recover. However, when clinicians are at odds as to whether a patient is indeed terminally ill, or when poor quality of life, psychological distress, or existential suffering lead to the decision to deactivate the LVAD, a greater sense of unease is usually found. Indeed, some patients have chosen to disconnect themselves from their LVAD at home, unfortunately without the support of hospice or appropriate symptom management strategies in place.
Palliative care clinicians should work with HF teams to gain experience in deactivating commonly implanted LVADs, when the need arises. It is important to anticipate symptoms of decreased cardiac output after LVAD withdrawal. Clinicians may consider bolusing medications such as diuretics and opiates to manage dyspnea that may acutely worsen after deactivation. Diminished circulation may delay peak onset of these medications after deactivation, so prospective administration of comfort medications before deactivation is recommended. Patients may survive for a few minutes to a few days after LVAD deactivation, and longer in very rare circumstances based on anatomy and underlying heart function; this variability should be discussed before deactivation.12,13
Palliative care clinicians should also gain proficiency in deactivating alarms for LVADs in patients who are close to dying, given that these alarms can cause significant distress to patients and families. LVAD coordinators are an invaluable resource in helping to navigate this process.
Tip 7: The DECIDE-LVAD Decision Aid Is Essential for Both Clinicians and Patients Considering LVAD Surgery to View Before Implantation
In the preimplantation setting, palliative care commonly participates in preparing patients to better understand LVAD therapy and its tradeoffs. One essential resource is a decision aid developed at the University of Colorado. In the DECIDE-LVAD clinical trial, 248 patients considering LVAD therapy were randomized to the decision aid versus usual care. 14 The decision aid comprises a 26-minute video and an eight-page brochure, which are freely accessible at https://patientdecisionaid.org/lvad. The study concluded that patients in the intervention arm had better decision quality, reflecting greater concordance of medical decision making and patients' stated care preferences, although fewer patients in the intervention arm went on to have LVAD implantation (54% vs. 80%, p < 0.01). The video is an essential education experience and this group recommends all palliative care clinicians view it themselves as well as share it with their patients.
Tip 8: Depression Is Common for Patients with LVADs, and Can Be Severe and Associated with Suicidality
Depression is common in patients with HF and can be more common in patients who receive LVADs. 15 Severe depression with suicidality is a difficult situation, given that patients have ready access to tamper with or deactivate their LVAD. Acute psychiatric treatment is challenging, given that many facilities are not credentialed to care for patient with LVADs or associated comorbidities. Thus, mitigating distress in an anticipatory manner to prevent escalation is key. Palliative care providers often play a role in counseling or recommending pharmacotherapy. Sleep issues, anxiety, and post-traumatic stress reaction are other mental health comorbidities for which palliative care clinicians can add value to improve symptom burden and quality of life.
Tip 9: Many Patients Have Good Clinical Outcomes Associated with LVAD Implantation
Given the practice and referral patterns of specialist palliative care providers, there may be a false notion that all patients with LVADs do clinically poorly, require intensive care, or need additional life-sustaining interventions. However, this is far from the case, and a diverse practice that includes outpatient clinics and embedded clinics with LVAD teams may help deal with systemic bias and outliers. As noted earlier, improved quality of life for a period of time was noted by 70% of decedents at 90 days for one cohort of patients with LVAD, 5 and a larger multicenter study showed that only one-third of patients had poor outcomes, including persistent poor quality of life or death within one year. 16
It is important for palliative care clinicians to realize that the median survival of LVAD patients is improving and that newer LVADs such as the HeartMate 3™ have shown improvement outcomes over prior generations, especially regarding lower pump thrombosis and stroke rates, so the discussions need to be flexible and iterative. 17
Tip 10: Caregiver Support Is Essential for LVAD Patients, and Support for Caregivers Who Face a Significant Burden of Care Is Needed
Caregiver burden is underestimated greatly by those taking care of LVAD patients and large gaps exist in this system. Not only is LVAD care demanding but also many LVAD recipients are elderly with multiple comorbidities, including poor vision, hearing, and touch, which inhibit their ability to hear alarms, reach for them, care for their drivelines, and so on. Most sites require LVAD patients to have dedicated caregivers who help the patient to manage the device and, in particular, the driveline. However, over time, burden eases as patients and their loved ones become more adept at various aspects of the disease and as the clinical condition improves. Therefore, assessing social support in an ongoing manner is a critical aspect of preimplantation discussions and is essential if patients are to have a good outcome. If possible, having multiple caregivers can help lessen risk of burnout versus a single caregiver. In addition, having respite systems in place could be beneficial, but these are not ubiquitous.
Conclusion
LVADs, especially as DT, are being more commonly employed by HF teams when caring for patients with advanced HF. While palliative care providers are often called to see LVAD patients for whom the clinical course has gone poorly, LVADs and other advanced therapies are helping many advanced HF patients live longer, better quality lives. Palliative care clinicians can offer tremendous value to patients considering LVAD, particularly by facilitating discussions between patients and their families about what matters most and exploring what physical states would be unacceptable to patients. Treating troubling physical and psychological symptoms, providing emotional and practical support for caregivers, and lessening the suffering of dying patients are all ways that palliative care teams can improve care for patients with LVADs. While more research into optimal palliative care strategies for patients with LVADs is needed, close partnership between advanced HF and palliative care teams is essential to ensure patient-centered care is available to these very ill patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.