
Abstract
Abstract
Background:
Care teams are increasingly expected to attend to the needs of patient's personal caregivers (e.g., family members). Improving communication among oncologists, patients with advanced cancer, and their personal caregivers might enhance caregivers' experiences of end-of-life (EoL) cancer care and bereavement outcomes.
Objective:
To explore the effects of the Values and Options in Cancer Care intervention on caregivers' experiences of EoL care and bereavement outcomes.
Design
: We developed a brief behavioral intervention to improve communication among oncologists, patients with advanced cancer, and their personal caregivers. The intervention was designed to help patients/caregivers ask questions, express concerns, and help oncologists respond effectively. We randomly assigned oncologists (and their patients/caregivers) to the intervention or usual care.
Setting/Subjects:
Medical oncologists in NY and CA; patients/personal caregivers with advanced cancer.
Measurements:
Two months after the patient's death, caregivers completed three instruments assessing their experiences of EoL care. Seven months after the patient's death, caregivers completed the Prolonged Grief Disorder-13 (PG-13; primary prespecified outcome), the Purpose-in-Life scale, and scales assessing mental health function, depression, and anxiety.
Results
: The intervention did not significantly improve caregivers' scores on the PG-13 (p = 0.21), mental health function, depression, or anxiety, but it did improve purpose-in-life scores (p = 0.018). Cohen's d (95% confidence interval) for all three experiences of EoL care outcomes were promising, ranging from 0.22 (−0.19 to 0.63) to 0.39 (−0.07 to 0.86) although none was statistically significant.
Conclusion:
Preliminary findings show promise that scalable interventions in cancer care settings may improve caregiver experiences with cancer care and some bereavement outcomes.
Introduction
As more is learned about the burdens and adverse health consequences of cancer caregiving, oncology care teams are increasingly expected to attend to caregivers' needs.1,2 Most interventions have been designed to help caregivers while patients are alive, 3 but caregivers continue to experience a range of difficulties after the patient's death, including regret about treatment decisions, symptoms of prolonged grief (e.g., bitterness, anger), and elevated risk for physical illness and death.4–6 Recent data suggest that it might be feasible to mitigate or prevent some poor bereavement outcomes by improving communication among oncologists, patients, and caregivers. Worse bereavement outcomes are now known to be more common when physician–patient communication about prognosis was lacking or ineffective7,8; when caregivers made treatment-decisions with inadequate support, 9 were unprepared for the death, 10 or believed that oncologists were negligent 11 ; and when patients experienced very poor quality of life, 7 did not enroll in hospice, or enrolled too late to benefit.10,12
Interventions to improve communication at the point-of-care may plausibly improve caregivers' experiences with cancer care and promote positive bereavement outcomes. 13 Communication interventions offered in inpatient, outpatient, supportive, palliative, or hospice care settings can be construed as preventive 14 if they aim, in part, to improve the dying experience and caregiver outcomes following the patient's death. Although many interventions conducted in outpatient cancer care have improved caregiver outcomes while the patient was alive,3,15,16 significant preventive effects on bereavement outcomes in cancer caregivers have never been reported. Outside of cancer care, successful preventive interventions have been offered in inpatient units, in intensive care units (ICUs), and in outpatient nephrology care.17–19 Other interventions offered in medical settings have not improved bereavement outcomes.16,20–22
The Values and Options in Cancer Care (VOICE) intervention was offered to oncologists, patients with a diagnosis of incurable solid nonhematologic cancers, and their caregivers. 23 Given the logistical burdens of cancer treatments on patients and families,1,2 and time pressure on clinicians, 24 there is a need for scalable preventive interventions that require minimal investment in time and resources by patients, personal caregivers, and oncologists. 25 The VOICE intervention aimed to improve patient and caregiver outcomes by helping them articulate their questions and concerns, and helping oncologists respond effectively. 26 As reported previously, the VOICE intervention improved communication between oncologists and patients/caregivers,23,27 but it did not significantly affect patient-reported quality of life or health care utilization before death. Nonetheless, the intervention could plausibly improve bereavement outcomes and lead caregivers to feel more satisfied with their experience of cancer care by helping them feel more supported in the caregiving role and better prepared for the patient's death.28,29 In this article, we report the effects of the VOICE intervention on caregiver-reported experiences of end-of-life (EoL) cancer care and caregiver psychological outcomes seven months after the death of the patient.
Methods
Overview
VOICE was a pragmatic, 30 cluster randomized controlled trial conducted in Western NY and Northern CA. Methodological details are published elsewhere.23,26 Oncologists were randomly assigned to an intervention or control condition. Oncologists assigned to the intervention participated in individualized communication training using standardized patient-instructors; their patients (with caregivers, if available) participated in one in-person coaching session and up to three follow-up telephone calls with their assigned coach. Oncologists (and their patients/caregivers) randomized to the control received usual care. The VOICE trial was funded by two grants. The primary outcome variable, funded by the first grant, was quality of communication. We received funding to explore 31 caregiver bereavement outcomes after funding for the primary outcome was received. IRB approval was obtained from all study sites; oncologists, patients, and caregivers provided written informed consent. VOICE is registered with ClinicalTrials.gov (NCT01485627).
Participants
Medical oncologists in community-based cancer clinics, academic medical centers, and community hospitals were eligible. By design, patients with caregivers were oversampled to achieve recruitment goals for this companion study of caregivers. Patients and caregivers were recruited, consented, and enrolled based on the arm to which their oncologist was assigned. For each enrolled oncologist, we attempted to enroll seven patients, at least five of whom would enroll with a caregiver.
Inclusion criteria were minimal in this pragmatic trial. 30 We sought to enroll a sample of patients who would survive for a median of 9–12 months. Patients of enrolled oncologists were eligible if they were ≥21 years old, able to understand English and provide consent. Patients either had a stage 4 nonhematologic cancer or a stage 3 cancer; the latter were eligible if their oncologist reported they “would not be surprised” 32 if the patient were to die within 12 months. Inpatients and patients in hospice were excluded.
Research assistants asked enrolled patients to identify “a family member, partner, friend, or someone else who is involved with your health care issues, for example, someone who you talk to about personal issues, including medical decisions or who comes to doctor appointments with you. This person may also help with routine day-to-day activities, like transportation or paperwork.” Research assistants received permission from patients to contact caregivers. Eligible caregivers were aged ≥21, able to understand English and provide consent. All enrolled participants received compensation.
Cluster randomization and blinding
The unit of randomization was the physician. Randomization was stratified by study site (NY or CA) and oncologist subspecialty (>50% breast cancer patients versus other). Within strata, oncologists were randomly assigned 1:1 to the intervention or control arms. Only the study statisticians were aware of the random number sequences and treatment assignment. Patients and caregivers were blinded to assignment until completion of measures at study entry. Research assistants were not blinded.
Interventions
Given the logistical burdens of cancer treatments on patients and families,1,2,25 the intervention was designed to minimize additional in-person appointments. The patient/caregiver coaching intervention often coincided with the oncology visit, and thus minimized burden 25 on participants' schedules. Patients of oncologists assigned to the intervention received up to one-hour of coaching before seeing the oncologist. Most enrolled caregivers (>90%) also attended the coaching session. Coaches (a trained registered nurse or social worker) gave each patient and caregiver a booklet (My Cancer Care) that was adapted from an established question prompt list developed in collaboration with colleagues in Australia.27,33 My Cancer Care was designed to empower patients and caregivers to ask questions and express their preferences regarding cancer care. The booklet provided concrete examples of questions and concerns about diagnosis, prognosis, treatment options, symptom management, care transitions, and so on.
Coaches guided participants through My Cancer Care and helped participants identify up to three questions/concerns, request clarification, and express desire to participate in discussions about their care. Patients and caregivers had the option of participating in three follow-up coaching calls coinciding with subsequent oncologist visits. These unstructured supportive calls varied in length (5–45 minutes) and were designed to reinforce prior coaching sessions and help participants identify new questions/concerns. A minority of enrolled caregivers (>40%) participated in at least one follow-up call.
Oncologists assigned to the VOICE intervention received a 15-minute educational DVD made by the research team on best practices in communication in the setting of advanced cancer, along with a laminated card highlighting those practices. They also received two 60-minute sessions of in-person individualized training with two experienced actors who portrayed a patient with stage 4 colon cancer and his wife. Following the first session, these standardized patient instructors listened to two audio-recordings per oncologist and provided oncologists with written feedback.
The oncologist training was designed to complement the coaching provided to patients/caregivers. Oncologists were trained to engage patients and caregivers as active participants in the consultation; respond to their emotions, concerns, and questions; inform them about prognosis and treatment choices; and frame information in a balanced manner (e.g., provide best case/worst case scenarios).
Oncologists assigned to the control arm, patients, and caregivers received no specialized training, but oncologists could choose to receive VOICE communication training after completing study activities. Patients in the control arm received a NCI publication, Coping with Advanced Cancer (NIH Publication No. 14-0856).
Timing of assessments and outcome measures
Timing of assessments
After a prerandomization phase that established oncologists' baseline communication patterns (12/11–7/12), patients and caregivers were enrolled (8/12–6/14). Before being informed of their randomization arm, patients and caregivers completed an assessment battery that included demographic characteristics and an assessment of depressive symptoms, the PHQ-8. 34 Patient vital status was tracked until December 2016. Prespecified caregiver bereavement outcomes were assessed two months and seven months after the patient's death; these assessments were conducted either in-person or by phone and were completed by July 2017. The interval between enrollment of the first caregiver and the final postmortem interview was thus nearly five years. We chose to assess our main outcome, symptoms of prolonged grief disorder, seven months after the patient's death because prior research suggests that uncomplicated grief typically improves within six months. 5
Psychological outcomes (seven months postmortem)
The primary prespecified outcome was the severity of prolonged grief symptoms, as measured by 10 items (alpha = 0.82) from the Prolonged Grief Disorder-13 (PG-13). 5 The PG-13 includes items such as “Do you feel emotionally numb since your loss?” Well-established measures were used to assess the other prespecified secondary outcome, overall mental health function (SF-12 Mental), 35 as well as three other outcomes, sense of purpose (Purpose in Life scale, alpha = 0.93), anxiety (GAD-7, alpha = 0.91), and depression (PHQ-9, alpha = 0.83).36–38
Experiences of care (two months postmortem)
We explored the effects of the intervention on caregiver-reported experiences of EoL care. Research assistants orally administered the six-item (alpha = 0.66) Caregiver Evaluation of the Quality of End-of-Life Care (CEQUEL), the eight-item (alpha = 0.87) Modified Decision Regret Scale (MDRS), and four items (alpha = 0.93) from the Human Connection Scale (HCS).39–41 The CEQUEL captured the caregiver's subjective impression of the quality of EoL care with items such as “Was the (patient's) life prolonged by medical interventions longer than you would have wished?” The MDRS assessed regret after cancer care decisions with items such as “The decision-making process was potentially harmful.” The HCS assessed the caregiver's experience of the relationship with the oncologist (e.g., “How much did you feel the doctor cared about you?”) and reflects their overall satisfaction with the oncologist.
Statistical analyses and power
Between-group comparisons were conducted using Wald-type tests from mixed-effects linear regression models specified to account for the nesting of patients/caregivers within oncologists. For all regression analyses, study site was included as a covariate to account for site-stratified randomization. Caregiver age, gender, level of education, and whether or not the caregiver was living with the patient were covaried to adjust for the effects of these demographic variables on caregivers' subjectively reported experiences. All statistical inferences were based on two-sided tests with p < 0.05 considered statistically significant. Analyses were conducted in version 9.4 of the SAS System.
Effect size (Cohen's d) was calculated as the ratio of the change in least-squared means to the pooled standard deviation (SD). The parent trial was powered to detect a significant effect on patient–caregiver–clinician communication (which was observed 19 ); this study had 0.8 power to detect an effect size of 0.45 for the primary outcome, PG-13, assuming an intraclass correlation of 0.05. Effect sizes ≥|0.2| (often considered “small” 42 ) were construed as promising in this exploratory 31 study.
Results
The CONSORT (Fig. 1) depicts the flow of participants from recruitment to study termination. Of the 204 caregivers enrolled in the trial, 127 (62.2%) became bereaved during the study period, 103 of whom (81.1%) provided data at the two-month and/or seven-month postmortem assessment. Table 1 provides descriptive data. At study entry, 9.8% of caregivers enrolled in the trial scored ≥10 on the PHQ-8; the mean PHQ-8 (SD) was 3.4 (3.4).
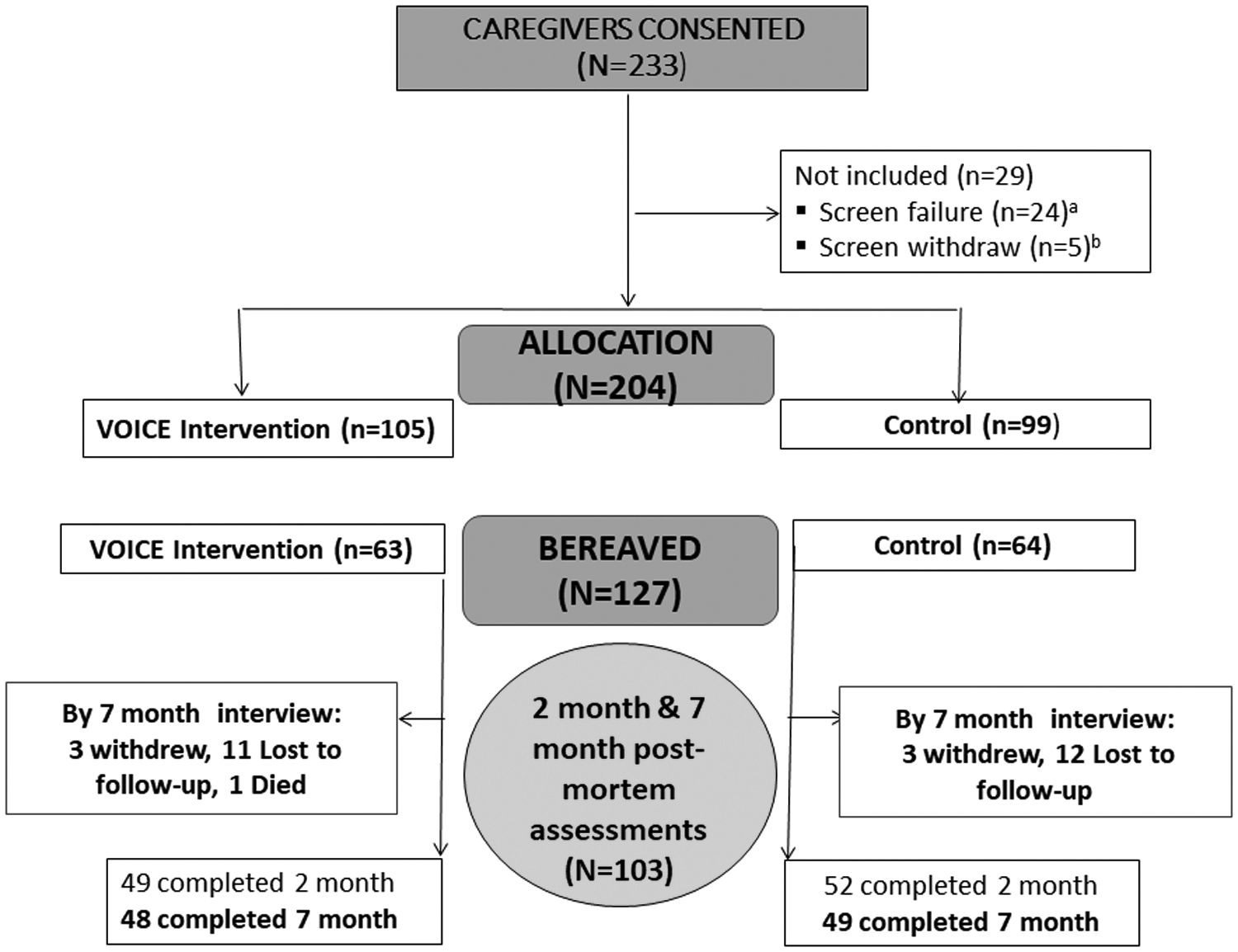
CONSORT diagrams depicting the flow of oncologists (n = 38) and patients (n = 265) were published elsewhere. 23 Most caregivers were patients' spouses or in a committed relationship; the remainder were patients' children and friends, neighbors, or other relatives. Patients were not required to enroll in the trial with a caregiver. Postmortem assessments were completed two months (n = 101) and seven months (n = 97) after the death. A total of 103 caregivers provided data at two months postmortem and/or seven months. aPatient became ineligible after consent, but before completing initial assessment. bPatient consented but withdrew before completing the initial assessment. VOICE, Values and Options in Cancer Care.
Descriptive Characteristics
Accounted for in multivariable analyses.
Table 2 provides results of multivariable analyses of caregiver experiences of care at the two-month postmortem assessment. Caregivers in the intervention condition reported greater satisfaction with the oncologist (HCS), less decisional regret (MDRS), and a better quality of death (CEQUEL). All effect sizes were promising (>|0.2|), but none was statistically significant.
Psychological Outcomes, Seven Months after Patient Death
Parameter estimates and p-values were derived from mixed-effects linear regression models controlling for study site (NY vs. CA) and caregiver demographics denoted by a superscript in Table 1.
CI, confidence interval; GAD-7, Generalized Anxiety Disorder-7; PG-13, Prolonged Grief Disorder-13; PHQ-9, Patient Health Questionnaire-9; SD, standard deviation; SE, standard error; SF-12, Short-Form 12.
Table 3 provides the results of the multivariable analyses of caregiver psychological outcomes measured at seven months postmortem. The intervention's effect on the main prespecified outcome, PG-13, was not statistically significant (p = 0.21), but the effect size was promising (|d| = 0.26). The intervention was associated with significantly higher scores on purpose in life (p = 0.018).
Experiences of End-of-Life Care, Two Months after Patient Death
Parameter estimates and p-values were derived from mixed-effects linear regression models controlling for study site (NY vs. CA) and caregiver demographics denoted by a superscript in Table 1.
CEQUEL, Caregiver Evaluation of the Quality of End-of-Life Care.
Discussion
Caregiving intervention research began in dementia care in the 1970s and was later extended to cancer care.3,43 It is now appreciated that interventionists must be able to accommodate caregivers' complex lives and overburdened schedules. We demonstrated that a brief intervention that was shown to improve communication between oncologists and patients/caregivers 23 holds promise for improving some caregiver experiences of EoL care and their bereavement adjustment. A preventive intervention implemented in French ICUs improved caregiver outcomes up to three months following patient death. The effect on purpose in life reported here was observed seven months after death and, in some cases, more than three years after exposure to the coaching intervention.
We hasten to add that purpose in life was a secondary outcome; moreover, the intervention effect on our primary outcome, PG-13, was promising (|d| = 0.26) but not statistically significant (p = 0.21). Promising effect sizes were also observed for all three indicators of experiences of care, including the HCS (d = 0.39), MDRS (|d| = 0.30), and CEQUEL (d = 0.22). We used items from the HCS that are quite similar to those used to evaluate the perceived quality of clinician communication, 44 and so, our findings suggest that brief communication interventions might plausibly boost ratings of care on measures such as the Consumer Assessment of Healthcare Providers and Systems (CAHPS) 45 or Press Ganey.
Observational studies have documented improvements in purpose-in-life following caregiving, 46 but this is the first time that such an effect has been shown in a trial. Even though the VOICE intervention did not explicitly attempt to address existential issues,47,48 it aimed to support caregivers and convey that their contributions to patient care were vital. Kleinman 49 and Lynn 50 have argued that caregiving is a moral act and that caregivers' contributions to society have historically been devalued. Positive, significant effects on sense of purpose in this trial might have resulted from caregivers becoming more meaningfully involved in patients' lives, advocating for their loved ones, and feeling more valued, efficacious, in control, and prepared for the patient's death. Future efforts aimed at enhancing purpose-in-life are warranted,47,51 given its association with improved quality of life, decreased risk for morbidity and mortality, 52 as well as better adherence to preventive service recommendations and lower health care expenditures. 53
To the best of our knowledge, no prior outpatient intervention in cancer care has had a discernible, positive impact on bereavement outcomes. The Educate, Nurture, Advise, Before Life Ends (ENABLE) intervention improved caregiver outcomes while the patient was alive, but did not significantly improve bereavement outcomes.15,16 Caregiver outcomes have not been examined in other promising cancer care interventions.54,55 Three interventions implemented in American ICUs had some salutary effects but no positive effects on bereavement outcomes21,22; unexpectedly, one intervention increased anxiety and posttraumatic stress symptoms in bereaved caregivers. 20 Outside of clinical trials, routinely administered hospice care and palliative care are intended to prevent poor bereavement outcomes, but relevant effectiveness data provide little evidence of benefit. 56 ln sum, most prior interventions have reported no positive effects16,20–22 and a potentially harmful effect 20 on caregiver outcomes. In this context, the current findings, together with a growing evidence base for similar preventive interventions,18,19 are cause for optimism.
Strengthening the intervention, perhaps by adding booster sessions for the oncologists or additional coaching sessions for patients/caregivers, might increase the intervention's effects. A chief barrier to dissemination of many efficacious behavioral interventions is that they place too many time-consuming demands on too many people (patients, caregivers, and clinicians), with little evidence that added investments in resources confer benefits that outweigh harms. The VOICE intervention was designed to minimize time demands and disruptions to all parties—patients, caregivers, and oncologists. Ideally, any increase in intervention dose would be incremental, given the toll of caregiving, the burdens of cancer treatments,1,2 and time pressure on clinicians. 24
Our findings should be interpreted in the context of several qualifiers. First, nonsignificant findings were unsurprising in this exploratory study; the parent trial was designed to examine communication at the point-of-care, not bereavement outcomes years later. Median patient survival was longer than expected (16 vs. 9–12 months) so there were fewer bereaved caregivers than anticipated. Moreover, unlike the enrollment criteria typically used in trials for complicated grief 57 or depression prevention, 58 exclusion criteria were minimal in this pragmatic trial. We reasoned that even caregivers who did not report significant depression at enrollment could benefit from the intervention; we sought to improve a wide array of outcomes, including experiences of care. Caregivers' depression scores were low at study entry, and consistent with another study. 59 (Data on anxiety at intake were unavailable.) Low depression scores at intake made it more difficult to observe significant effects on indicators of distress (a floor effect), but the observed effect size for PG-13 (|0.26|) was comparable to a significant effect observed in another trial. 48 Second, the sample was primarily white and relatively well educated. Third, we cannot test competing mediational hypotheses in this pragmatic trial, do not have data on mechanisms of action (e.g., extent of patient and caregiver participation in the coaching or telephone calls), and do not know whether observed improvements in caregiver purpose in life were discernible before the patient died. 60
In closing, hundreds of intervention studies have been designed to mitigate the toll of caregiving, but few have followed caregivers after the patient's death to determine if the intervention protected against poor bereavement outcomes or conferred other benefits. The preliminary findings reported here are conceptually important because they suggest that bereavement outcomes can be modified with brief interventions mounted in health care settings months if not years before death. Interventions designed to preemptively soften the blow of losing a loved one are not feasible for people bereaved suddenly due to suicide, overdose, and other causes of sudden death, but could be integrated into routine outpatient cancer care. Our findings should encourage further tests of the downstream effects of communication interventions in cancer care settings.
Footnotes
Acknowledgments
The work reported in this study was supported by grants from the National Cancer Institute (R01CA168387, R01CA140419, and R35CA197730).
Author Disclosure Statement
No competing financial interests exist.