
Abstract
Abstract
Background:
The C-reactive protein/albumin (CRP/Alb) ratio has been reported as a prognostic factor of survival for patients with a variety of cancers. However, its prognostic impact for advanced cancer patients receiving palliative care remains presently unknown.
Objective:
The present study assessed the prognostic value of the CRP/Alb ratio, and compared this with that of the Glasgow Prognostic Score (GPS) and Palliative Prognostic Index (PPI) in a cohort of advanced cancer patients receiving palliative therapy.
Methods:
The medical records of 262 eligible patients who died of advanced cancer from February 1, 2013 to December 30, 2017 in the palliative care unit of the Fudan University Shanghai Cancer Center were retrospectively reviewed for the analysis.
Results:
The present results revealed that a CRP/Alb ratio ≥1.31 (hazard ratio [HR], 2.33 [1.78–3.05], p < 0.001) can predict poor prognosis through univariate analysis. In addition, the multivariate analysis revealed that CRP/Alb (HR, 2.09 [1.54–2.84], p < 0.001), GPS (HR, 1.81 [1.07–3.07], p < 0.001), and PPI (HR, 3.35 [2.25–4.99], p < 0.001) were all independent prognosis factors. To compare the discriminatory performance of the CRP/Alb ratio with that of other established prognostic indexes in palliative care settings, the c-statistics, integrated discriminatory improvement index, net reclassification index, and receiver operating characteristic curves were generated, and it was demonstrated that the CRP/Alb ratio (c-statistics, 0.64 [0.61–0.68]) was able to discriminate advanced cancer patients with different survivals, with analogous discriminatory ability as GPS (c-statistics, 0.63 [0.59–0.66]) and PPI (c-statistics, 0.64 [0.60–0.68]). Notably, the combination of multiple prognostic indexes exerted higher discriminatory ability, compared with any single predictive index (c-statistics, 0.69 [0.66–0.73], p < 0.001).
Conclusions:
The present study suggests that the CRP/Alb ratio is a promising prognostic factor in predicting cancer patient survival in palliative care settings. Incorporating both objective parameters and the subjective index may improve the prediction accuracy of prognosis.
Introduction
Patients with advanced cancer can be informed of the predicted survival time through accurate prognostic information, helping them prepare for their impending death, especially for patients who are unable to tolerate aggressive treatment.1–3 This information is also critical for clinicians to advise appropriate medical interventions. However, the clinicians' predictions of survival remain inaccurate due to various factors, including their education and training, seniority and experience, and the level of acquaintance with patients, all of which can affect their estimation.4,5 Due to a limited lifespan, established prognostic indicators such as age, tumor-node-metastasis (TNM) stage, and tumor marker levels are not appropriate for advanced cancer patients receiving palliative care. Therefore, accurate prognostic tools are urgently needed for predicting the survival of advanced cancer patients receiving palliative therapy.
C-reactive protein (CRP) is an acute phase protein, and its increase in serum is correlated to a worsening inflammatory status and the progression of cancer. 6 Importantly, CRP has been considered a prognostic marker for cancer patients in palliative care settings. 7 A decrease in albumin (Alb) level is correlated to a chronic inflammatory state and poor nutritional status.8–12 Recently, the CRP/Alb ratio has been reported as a prognostic factor of survival in patients with lung cancer, pancreatic cancer, nasopharyngeal cancer, esophageal cancer, oral cancer, colorectal cancer, and hepatocellular carcinoma.13–26 However, previous studies focused on patients with solid cancers receiving surgery, chemotherapy, or radiotherapy, of which the proportion of advanced cancers was low, thereby excluding the advanced cancer patients in a variety of palliative settings. The prognostic value of the CRP/Alb ratio for advanced cancer patients receiving palliative care remains presently unknown.
Previous studies have identified several prognostic tools for predicting survival in terminally ill patients with advanced cancers, such as the Glasgow Prognostic Score (GPS),27–32 Palliative Prognostic Index (PPI),33–38 and Palliative Prognostic Score (PPS).39–43 However, the prognostic values of these tools have not been directly compared, to date. These prognostic tools vary in complexity, subjectivity, and their clinical utility. Further researches comparing these tools in a cohort of patients are necessary to determine the optimal prognostic tools.
The present study aimed to identify a novel prognostic tool that can be quickly and easily applied in clinical practice for a more accurate prediction of survival of terminally ill patients. Furthermore, the present retrospective study evaluated the prognostic value of the CRP/Alb ratio and compared this with that of the GPS and PPI in a cohort of advanced cancer patients receiving palliative therapy in our palliative care unit.
Materials and Methods
Patients
The medical records of 442 patients who died of advanced cancer from February 1, 2013 to December 30, 2017 in the palliative care unit of the Fudan University Shanghai Cancer Center were retrospectively reviewed. The eligibility criteria for the present study were as follows: (1) patients with histologically proven malignant tumors; (2) patients with available data on CRP and Alb. Patients who died of non–cancer-related reasons were excluded. A written informed consent was obtained from each patient, and all patients agreed to store and use their information in the hospital database. Furthermore, clinicopathologic information and laboratory test results were retrospectively collected.
Scoring of GPS and PPI
The GPS score was determined through the CRP and Alb values: a score of 0 means both CRP ≤10 mg/L and Alb ≥35 g/L; a score of 1 means either CRP >10 mg/L or Alb <35 g/L; a score 2 means both CRP >10 mg/L and Alb <35 g/L. 44 The PPS was determined through six subjective parameters, and the performance status included ambulation and activity levels.45,46 The PPI score categorized survival as follows: risk group 1 (PPI score ≤4), risk group 2 (PPI score = 5), and risk group 3 (PPI score >6). Furthermore, this consisted of five subjective parameters: PPS, oral intake, edema, dyspnea at rest, and delirium (Supplementary Table S1). 36
Statistics
Based on the type of data, chi-squared test or Mann-Whitney U test was used to evaluate the differences in baseline and clinicopathological parameters between groups. Overall survival (OS) indicated the time interval from the date the patients were transferred to our palliative care unit to their death. The optimum cutoff for the CRP/Alb ratio was determined by analyzing the receiver operating characteristic (ROC) curve. Spearman's correlation was used to assess the relationship between CRP/Alb ratio and survival time in the cohort of patients. The Kaplan–Meier method was used to plot the OS curves, and log-rank test was employed to compare the differences. Univariate and multivariate analyses were performed with a Cox regression. The Cox proportional-hazards model was applied to calculate the hazard ratio (HR) and 95% confidence interval (CI). The backward stepwise method was used for the multivariable analysis of selected variables with significantly (a significance level of 0.1) prognostic values in the univariate analysis. To evaluate the discriminatory ability of different scoring methods, Harrell's c-statistic and Akaike Information Criterion (AIC) 47 were used, the ROC curves were generated, and areas under the curve (AUC) were measured and compared. The survIDINRI package implements the integrated discriminatory improvement index (IDI) and the net reclassification index (NRI) for comparing competing risk prediction models. These statistical analyses were carried out using the SAS 9.4 software (SAS Institute, Cary, NC). A p value <0.05 was considered statistically significant.
Results
Clinical characteristics of patients
Initially, the medical records of 442 advanced cancer patients receiving palliative therapy were retrospectively reviewed. Among these, 272 patients with available CRP and Alb data were included in the present study. After a careful examination of the pathological diagnosis data, 10 patients with clinically suspected cancer, but without a pathological diagnosis, were excluded. This resulted in a total of 262 eligible patients for analysis in the present study. The baseline characteristics of these patients, in terms of demography, pathology, tumor progression, and biochemistry assay results, are listed in Table 1. The age of these patients ranged between 14 and 87 years, with a median of 64 years. Half (131/262) of the patients were male. Per TNM staging, most of the patients were stage IV (93.13%), while the minority of patients were stage III (3.82%). A total of 57 patients had multiple cancer metastases (>3 sites; Table 1).
Baseline Characteristics of the 262 Advanced Cancer Patients Receiving Palliative Therapy
Alb, albumin; CRP, C-reactive protein; GPS, Glasgow Prognostic Score; KPS, Karnofsky Performance Status; PPI, Palliative Prognostic Index; TNM, tumor-node-metastasis.
The CRP/Alb ratios drastically varied among these patients, which ranged within 0.01–12.73, with a median of 1.80. Spearman's correlation showed that the increase in CRP/Alb ratio is inversely proportional to survival time in the cohort of patients (Spearman's ρ = −0.4163, p = 0.0000). Through an ROC analysis, the optimal cutoff value of the CRP/Alb ratio was determined to be 1.31. Then, the potential correlation between the CRP/Alb ratio (<1.31 and ≥1.31) and baseline characteristics of patients was analyzed (Table 1). There were no differences in terms of the distribution of age, gender, and site of primary cancer between the two groups, and varied CRP/Alb ratios were identified. In all the patients, the top four sites of primary cancers were the hepatobiliary organs and tissues, colon/rectum, pancreas, and gynecologic tract. Notably, a higher CRP/Alb ratio (≥1.31) was found to be closely associated with a more advanced TNM stage (p = 0.001). Furthermore, a higher CRP/Alb ratio was also associated with more distant metastases, lower Karnofsky Performance Status (KPS; p < 0.001), and a higher CRP value (>10 mg/L).
Next, it was determined whether the CRP/Alb ratio was associated with other established prognostic categories, including those obtained through the methods of GPS, PPI, and plasma CRP concentration. As shown in Table 1, the CRP/Alb ratio was identified to be significantly associated with both GPS and plasma CRP concentration (p < 0.0001). Most patients (n = 133, 50.76%) with a higher CRP/Alb ratio (≥1.31) had a high GPS score of 2, while none of the patients had a GPS score of 0 (p < 0.0001). In addition, all patients in the higher CRP/Alb group (n = 160, 61.07%) had a CRP value >10 mg/L (p < 0.0001). The distribution of PPI scores (1, 2, and 3) had no significant difference in terms of the high (≥1.31) and low (<1.31) CRP/Alb ratios (p > 0.05). Therefore, the CRP/Alb ratio is closely associated with the GPS score and CRP value, but not closely associated with the subjective index PPI.
Survival analysis
The median survival time of patients receiving palliative care in our unit was 22 days (95% CI, 17–28). Some patients of the whole cohort survived for as long as 360 days, but most patients (95.42%) died within 180 days (Table 2). The median survival period for patients with a CRP/Alb ratio <1.31 and ≥1.31 was 45 days (95% CI, 29–57) and 16 days (95% CI, 14–20), respectively. The median survival period for the patients in PPI risk groups of 1, 2, and 3 was 36 days (95% CI, 27–45), 17 days (95% CI, 14–27), and 8 days (95% CI, 5–12), respectively. The median survival period for patients with GPS scores of 0, 1, and 2 was 130 days (95% CI, 67–166), 36 days (95% CI, 23–45), and 16 days (95% CI, 14–21), respectively. The median survival period for the patients with serum CRP concentrations ≤10 and >10 mg/L was 103 days (95% CI, 47–143) and 18 days (95% CI, 16–24), respectively (Table 2).
Survival Rates Based on C-Reactive Protein (CRP)/Albumin, Glasgow Prognostic Score, Palliative Prognostic Index and CRP Categories
Prognostic analysis
The Kaplan–Meier survival curves of patients in categories based on the CRP/Alb ratio, CRP concentration (≤10/>10 mg/L), GPS and PPI, respectively, are presented in Figure 1. Compared with patients with a lower CRP/Alb ratio (<1.31), the patients with a higher CRP/Alb ratio (≥1.31) demonstrated a significantly worse median survival (p < 0.001; Fig. 1), while a CRP/Alb ratio ≥1.31 (HR, 2.33 [1.78–3.05], p < 0.001) was found to be a poor prognostic marker in the univariate analysis (Table 3). In addition, parameters including CRP (HR, 2.33 [1.78–3.05], p < 0.001), GPS (HR, 2.97 [1.87–4.73], p < 0.001), and PPI (HR, 3.68 [2.55–5.30], p < 0.001), as well as oral intake (HR, 1.62 [1.23–2.12], p = 0.001) and edema (HR, 1.39 [1.08–1.79], p < 0.05) were all prognostic in the univariate survival analysis (Table 3). However, no statistically significant differences were identified in other parameters, such as age, gender, dyspnea, delirium, Alb, and PPS (p > 0.05).
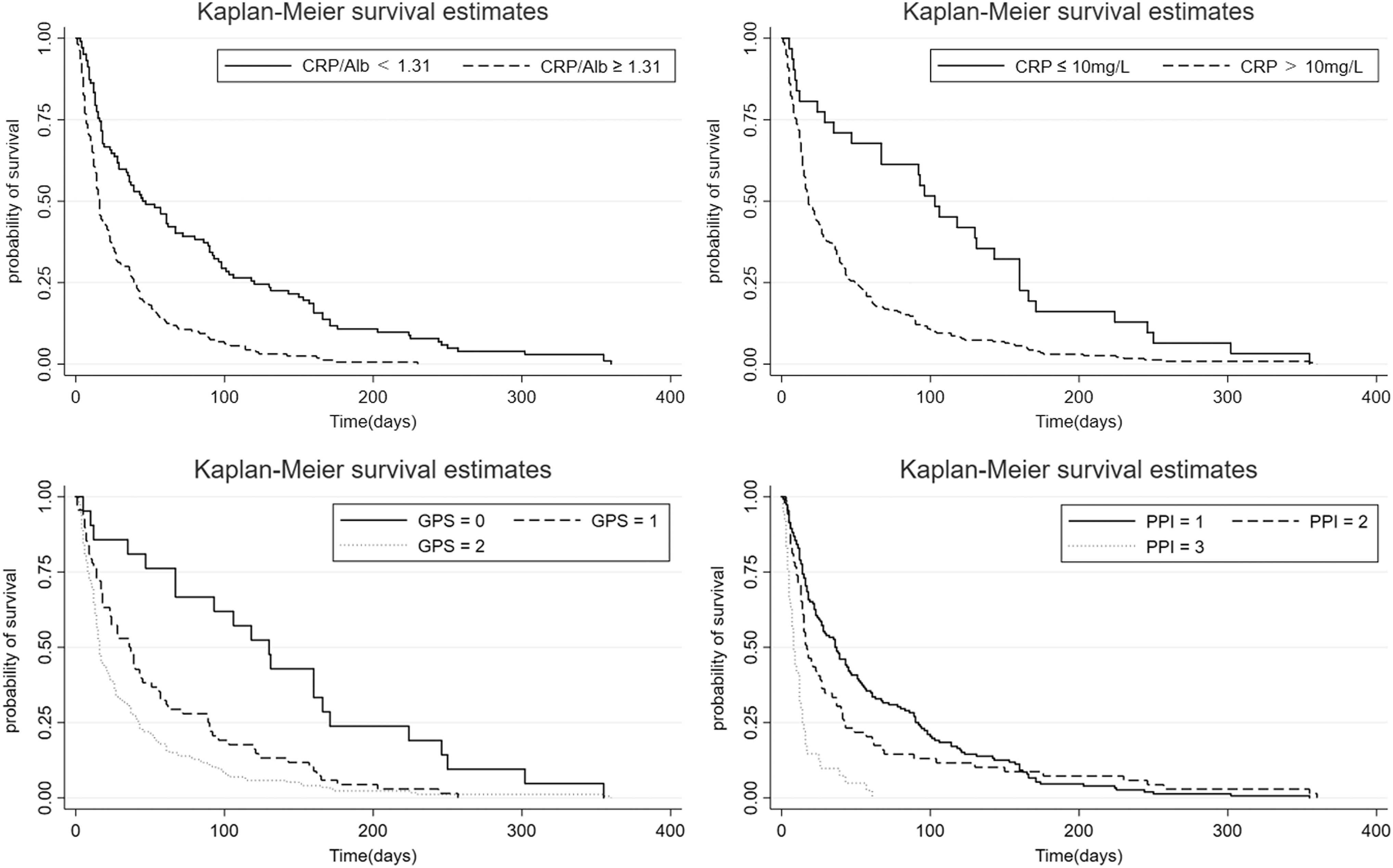
The Kaplan–Meier survival curves show the survival periods of patients in categories, based on the CRP/Alb ratio (up left), CRP concentration (up right), GPS (low left) and PPI (low right), respectively. Alb, albumin; CRP, C-reactive protein; GPS, Glasgow Prognostic Score; PPI, Palliative Prognostic Index.
Univariate Cox Proportional Hazards Regression Analysis of Advanced Cancer Patients Receiving Palliative Care
CI, confidence interval; HR, hazard ratio.
Next, a multivariate survival analysis was performed, in which the backward-selected (0.1 significance level) parameters of gender, CRP, oral intake, edema, CRP/Alb, GPS, and PPI were included, while CRP and edema were excluded. In the multivariate analysis, the CRP/Alb ratio (HR, 2.17 [1.60–2.94], p < 0.001) remained an independent prognostic marker. Other independent prognostic markers included GPS (HR, 1.71 [1.01–2.85], p = 0.044), PPI (HR, 3.30 [2.28–4.77], p < 0.001), female gender (HR, 0.76 [0.59–0.97], p = 0.03), and oral intake (HR, 1.33 [1.01–1.74], p = 0.039). Adjusted by gender, age, and oral intake, the present results revealed that the CRP/Alb ratio (HR, 2.09 [1.54–2.84], p < 0.001) had a prognostic value independent of GPS and PPI, while PPI (HR, 3.35 [2.25–4.99], p < 0.001) appeared to be better than the CRP/Alb ratio and GPS (HR, 1.81 [1.07–3.07], p = 0.027) (Table 4).
Multivariate Cox Proportional Hazards Regression Analysis of Advanced Cancer Patients Receiving Palliative Care
Multivariate model with backward selection (significance level, p < 0.1). The variables CRP and edema were eliminated in the final multivariate model, which included gender, oral intake, CRP/Alb, GPS and PPI.
Adjusted by gender, age and oral intake.
ns, not significant.
Performance comparison of CRP/Alb, GPS, and PPI methods
To compare the discriminatory performance of the CRP/Alb ratio with that of other established prognostic indexes in the palliative care setting, Harrell's c-statistic and AIC were generated. The univariate CRP/Alb model had similar c-statistics and AIC values compared with the univariate GPS and PPI models (p > 0.05; Table 5), indicating the analogous discriminatory ability of the CRP/Alb method (c-statistics, 0.60, 95% CI, 0.57–0.64) with other established prognostic indexes. The multiple prognostic indexes (all) with a combination of CRP/Alb, GPS, PPI, age, gender, and oral intake had the highest c-statistics (c-statistics, 0.69, 95% CI, 0.65–0.72, p < 0.001; Table 5) and the lowest AIC value of 2331. In the multivariate models, the CRP/Alb method with a higher c-statistics (c-statistics, 0.64, 95% CI, 0.61–0.68) and lower AIC value of 2358 was statistically better, compared with other indexes, including gender, age, and oral intake (c-statistics, 0.59, 95% CI, 0.55–0.63, p < 0.001; Table 5). The multiple prognostic indexes (all) also showed the best discriminatory ability compared with any single method (c-statistics, 0.69, 95% CI, 0.66–0.73; Table 5). The low c-statistics and similar results of the CRP/Alb, GPS, and PPI models need to be further verified. The CRP/Alb method had the highest NRI of 0.55 compared with any single method at 90 and 180 follow-up durations (Supplementary Table S2). The NRI and IDI of the multiple prognostic indexes (all) method were 0.48 and 0.08 at 180 days of follow-up (p < 0.01; Supplementary Table S2). The CRP/Alb model and multiple prognostic indexes model had higher discriminatory ability compared with other indexes, GPS and PPI models.
Comparison of Discriminatory Performance of the Different Models in Predicting the Survival Time of a Cohort of Advanced Cancer Patients Receiving Palliative Care
Multivariate models including gender, age and oral intake.
Other indexes including gender, age and oral intake.
A combination of all indexes, including CRP/Alb, GPS, PPI, age, gender and oral intake.
AIC, Akaike Information Criterion.
To further compare the discriminatory and calibration performance of these methods, ROC curves indicating the survival status of patients at 30, 90, and 180 days of follow-up were generated. As shown in Figure 2, the CRP/Alb, GPS, and PPI methods demonstrated obviously higher AUC values, compared with other indexes, including gender, age, and oral intake. At 90 days after the initiation of follow-up, the CRP/Alb method (AUC, 0.7983; 95% CI, 0.7339–0.8628) and GPS method (AUC, 0.7983; 95% CI, 0.7285–0.8680) had higher AUC values compared with the PPI method (AUC, 0.7293; 95% CI, 0.6519–0.8067). In addition, the AUC value from the CRP/Alb method (AUC, 0.8473; 95% CI, 0.7626–0.9321) was higher compared with that of the GPS method (AUC, 0.8303; 95% CI, 0.7322–0.9284) and PPI (AUC, 0.7242; 95% CI, 0.6149–0.8335) at 180 days of follow-up (CRP/Alb vs. PPI, p < 0.05). Furthermore, AUC values revealed that multiple prognostic indexes (all) method had a higher discriminatory ability, compared with any single method at all the selected follow-up durations (p < 0.05; Table 6).
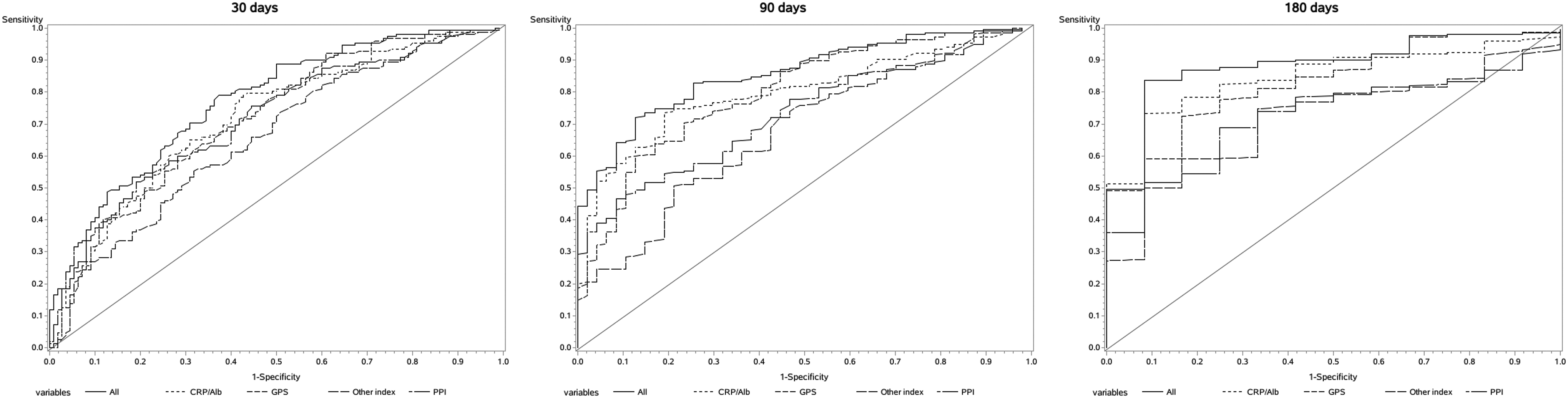
Comparisons of prognostic indexes through plotting the ROC curves at 30, 90 and 180 days of follow-up. The ROC curves show the sensitivity and specificity of the CRP/Alb ratio, GPS, PPI, other indexes (age, gender and oral intake), and all (a combination of all indexes, including CRP/Alb, GPS, PPI, age, gender and oral intake) in predicting the survival status of patients at 30, 90 and 180 days of follow-up. ROC, receiver operating characteristic.
Comparisons of the Area under the Curve of the C-Reactive Protein/Albumin, Glasgow Prognostic Score and Palliative Prognostic Index Methods at Selected Follow-Up Durations
Note: The results were adjusted by age, gender and oral intake.
Other indexes including gender, age and oral intake.
A combination of all indexes, including CRP/Alb, GPS, PPI, age, gender and oral intake.
Represents the statistical differences, when compared with other indexes.
In summary, the methods of CRP/Alb, GPS, and PPI were all able to discriminate patients with different survivals in palliative care settings. It is noteworthy that incorporating multiple prognostic indexes improved the prediction accuracy of prognosis.
Discussion
Some nutrition indexes and inflammation-based parameters derived from the laboratory routine tests, including CRP, GPS, and albumin, have been established to better predict the survival time of patients with advanced cancer. Meanwhile, malnutrition is associated with worse survival in patients, and the evaluation of inflammation can also provide some prognostic value in cancer patients. Recently, the CRP/Alb ratio has been considered a prominent parameter for the identification of seriously ill patients, 48 and has also been proposed to be an independent marker for predicting the 90-day mortality of patients with severe septic. 49 Furthermore, accumulating studies have suggested that the CRP/Alb ratio is also a promising prognostic factor of survival in a variety of cancers.17–19,21,26,50–57 However, as far as we are aware, the clinical implications of the CRP/Alb ratio as a biomarker in patients with advanced cancer in palliative care settings have not been intensively investigated. The present study sought to assess the potential prognostic value of the CRP/Alb ratio and evaluate the possibility of applying this new prognostic tool in clinical practice by comparing this with GPS and PPI tools in the same cohort of advanced cancer patients in our palliative care center. The optimal cutoff of the CRP/Alb ratio broadly varied (0.0271–2) in previous reports. Remarkably, in the present study, the cutoff value of the CRP/Alb ratio was set at 1.31, and this expediently predicted the survival of patients with advanced cancer.
The clinicopathologic relevance of the CRP/Alb ratio was first evaluated in 262 cancer patients receiving palliative care. It was demonstrated that the high ratio of CRP/Alb was correlated with advanced TNM stage, poor performance status, and more distant metastases, indicating that this ratio is valuable in predicting prognosis. The univariate and multivariate analyses suggest that gender, oral intake, CRP/Alb, GPS, and PPI are independent significant prognosis factors. In addition, both the c-statistics and ROC curves proved that the CRP/Alb ratio had similar prognostic ability as GPS and PPI. However, the CRP/Alb method had the highest NRI compared with any single method. The different results of c-statistics, NRI, IDI, and AUC value may have been caused by different algorithms that we applied. Both the CRP/Alb ratio and GPS were determined by calculating the same parameters—the concentrations of CRP and albumin. The GPS only reflects the abnormalities of CRP and Alb concentrations, while the CRP/Alb ratio further reflects the degree of CRP elevation and Alb decrease in serum. The CRP/Alb value varied from 0.01 to 12.73 in our study, with a median of 1.80. The increase in CRP/Alb ratio is inversely proportional to survival time in the cohort of patients. It provides more information, compared to GPS, for doctors to determine the predicted survival time of patients. The superiority is also reflected by its quick and easy application in clinical practice. The CRP/Alb ratio is entirely objective, since the value is totally based on laboratory test results. On one hand, the CRP/Alb method had higher NRI and IDI values compared with GPS and PPI methods at 90 and 180 days of follow-up. On the other hand, it is hard to distinguish the survival differences for patients with GPS scores of 1 and 2, as well as for patients with PPI scores of 1 and 2. Moreover, the PPI consists of five subjective parameters, such as the PPS, oral intake, edema, dyspnea at rest, and delirium. The incorporation of these subjective parameters might enhance prognostic accuracy, while this might also increase bias, and thereby reduce clinical utility. However, the present study demonstrated that the combinational use of multiple prognostic indexes, including the CRP/Alb, GPS, PPI, age, gender, and oral intake, led to a higher discriminatory ability, compared with any single predictive index. These results suggest that both objective and subjective indexes are necessary for more accurate predictions of patient survival.
The study conducted by Amano et al. 58 demonstrated that the elevated plasma CRP level (>10 mg/L) predicted poor prognosis in patients with advanced cancer, and a positive correlation between CRP levels and badness of prognosis was observed. However, a single index of CRP level could not be applied in the present study. Since 231 of 262 (88.17%) patients had a CRP concentration >10 mg/L, the CRP level alone could not distinguish the differences in survival time for most cancer patients. Moreover, although the univariate analysis revealed that CRP level (>10 mg/L) was one of the factors that indicated poor prognosis in the cohort of patients (HR, 2.33 [1.78–3.05], p < 0.001), the index of CRP level was excluded from the present multivariate analysis using the backward method.
The present study had some limitations. The major limitation of the present study was that the data were retrospectively obtained from a single center, and the data of patients who died outside of the unit were lost. Incomplete follow-up data and different algorithms that we applied led to inconsistent results of c-statistics, NRI, IDI, and AUC values. An independent validation cohort is needed to further verify the prognostic value of the CRP/Alb ratio. In addition, prospective studies with larger sample sizes are needed to further explain the predictive value of the CRP/Alb ratio in patients with advanced cancer. Furthermore, since the optimal cutoff values of this ratio differ among different types of cancers, a meta-analysis is necessary to more accurately determine the prognostic value of the CRP/Alb ratio in advanced cancer.
Conclusions
The present study suggests that the CRP/Alb ratio represents a promising prognostic predictor of survival in palliative care settings. It is noteworthy that incorporating both objective parameters and the subjective index may improve the prediction accuracy of prognosis. Prospective studies with large sample sizes from multiple centers should be conducted to further verify the results of the present study.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.