
Abstract
Abstract
Background:
Dyspnea is one of the most common symptoms in patients with advanced disease and terminal illness, associated with poorer quality of life. The efficacy of fan therapy to palliate dyspnea is inconsistent and unclear.
Objective:
The aim of this meta-analysis was to evaluate the efficacy of fan therapy for the relief of dyspnea in adults with advanced disease and terminal illness.
Design:
The CENTRAL, MEDLINE, EMBASE, CINAHL, and PsycINFO were searched to retrieve all randomized controlled trials examining the benefits of fan therapy for the relief of dyspnea in patients at the advanced stages of illness. Risk of bias was assessed according to the Cochrane Collaboration standard scheme.
Results:
Five studies involving 198 adults were identified. Fan therapy was associated with a significant relief of breathlessness intensity immediately after intervention (mean differences [MDs], −1.01; 95% confidence interval [CI], −1.57 to −0.45; p < 0.001) and 10 minutes after intervention (MDs, −0.90; 95% CI, −1.53 to −0.27; p = 0.005). Long-term application of fan therapy for at least one month was not related to changes of dyspnea severity (MDs, 0.10; 95% CI, −1.14 to 1.35; p = 0.870). However, significant heterogeneity and low quality of the included trials limit applicability of the results in general practice. No difference was found in activity performance, respiratory rate and SpO2, changes in other symptom intensities, and adverse events.
Conclusion:
Current trials provided low-quality evidence for a significant short-term effect after fan therapy in the relief of dyspnea and no beneficial effect in the long-term application in adults with advanced disease and terminal illness.
Introduction
Dyspnea is one of the most common symptoms in patients with advanced disease and terminal illness, characterized by subjective experience of breathing difficulty and discomfort.1,2 It is not only associated with psychological changes, 2 but also related to poorer quality of life, unscheduled hospital attendance, and admission. 3 Dyspnea is induced by various factories and the underlying genesis involves several neural pathways and excessive stimulation of the respiratory center.2,4 The prevalence of dyspnea is increasing as the management of advanced disease has improved. Management of symptom is often multimodal, with a combination of the causally directed management of breathlessness and pharmacological/nonpharmacological interventions.5,6 Particularly for patients receiving palliative care, nonpharmacological was able to improve patients' personal initiative and participation, therefore improving their quality of life. 6
Fan therapy, with advantages of low cost, portability, minimal potential side effects, and easiness to operate by the patients, independent of any clinician or setting, is thought to palliate dyspnea.7–11 Nevertheless, there is a gap of meta-analysis to address the effectiveness of fan therapy in breathlessness, and recent studies were inconclusive of this strategy.12,13 Accordingly, this review was conducted to evaluate the efficacy of fan therapy for the relief of dyspnea in people with advanced disease and terminal illness.
Methods
Literature search
We electronically searched the CENTRAL in the Cochrane Library, MEDLINE, EMBASE, CINAHL and PsycINFO. The key words included “dyspnea,” “breathless,” “breathlessness,” “shortness of breath,” “fan,” “wind,” and “air movement.” Details of search strategies were attached as Supplementary Data S1. A manual search was performed to identify potentially eligible studies according to the references from the articles for full review. The searches were last updated in January 2019.
Eligibility criteria
The inclusion criteria for our analysis were as follows: (i) studies enrolled adult participants (≥18 years old); (ii) randomized controlled trials (RCTs), as well as crossover studies in which patients were randomized based on the order of treatment; (iii) studies enrolled participants with breathlessness caused by advanced disease or incurable terminal illness; and (iv) studies assessing the benefits of fan therapy for breathlessness compared with no fan or placebo. The exclusion criteria were meeting abstracts, duplicate reports of a study, and data unavailable.
Selection process
After excluding the duplicate records, two independent authors reviewed the titles and abstracts of all the items to exclude irrelevant studies. And then a detailed review of the full-text was performed to select trials according to the eligibility criteria. Any discrepancy was resolved by discussion with a third author.
Data extraction
Two independent authors extracted data from the full-text article of each included study (Table 1). Crossover studies were treated as parallel studies by extracting data from the first period only to avoid the reported carry-over effect. 11 The primary outcomes were the changes of breathlessness intensity on any validated scale and activity performance. The secondary outcomes included (i) changes in facial surface temperature, respiratory rate, and SpO2; (ii) changes in other symptom intensities, including well-being, tiredness, lack of appetite, pain, anxiety, depression, and nausea; and (iii) adverse events.
Basic Characteristics of the Included Studies
NA, not available; NRS, numerical rating scale; VAS, visual analog scale; AKPS, Australia-modified Karnofsky Performance Status.
Quality assessments
The methodological quality in each trial was independently assessed by two authors on the basis of the Cochrane Collaboration standard scheme, including selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and any other potential sources of bias. All of the included trials were evaluated for each type of bias as high risk, low risk, or unclear risk. Any disagreement was resolved by consensus with a third author.
Statistical analysis
All calculations were performed using Review Manager 5.3 (Cochrane, London, United Kingdom). The results of continuous outcomes were presented as mean differences (MDs) with 95% confidence intervals (CIs). Heterogeneity was evaluated using the chi-square test with a 10% level of statistical significance (p < 0.1) and I2 > 50%. 14 Data were pooled using a fixed-effect model and if a marked heterogeneity was present, a random-effects model was used and sensitivity analysis was performed to help assess the contributions of a single study to the pooled results and to take into account the robustness of results. The funnel plots were not constructed because of the limited number of studies included in this review. 15
Results
Literature search
A total of 506 potentially relevant studies were identified by the search strategy: 41 in MEDLINE, 109 in EMBASE, 155 in Cochrane CENTRAL, 101 in CINAHL, 98 in PsycINFO, and 2 by handsearching the references of related literature. After adjusting for duplicates and screening the titles and abstracts, 24 studies remained. A further discard was conducted based on the full-text review, and five studies8,11–13,16 were finally included (Fig. 1). More detailed characteristics of the excluded studies are shown in Supplementary Table S1.

A flow diagram of the retrieved, screened, and included studies.
Study characteristics
The trials included in this meta-analysis were published between 2010 and 2018. Three of the included trials were multicentered conducted in Germany, Australia, and United Kingdom,8,12,13 and the other two were single-centered performed in China and Japan.11,16 A total of 198 participants were included, with 110 in the fan therapy group and 88 in the control group. Men comprised half (50.6%) of the study population. Two studies recruited only participants with advanced cancer,11,16 and the other three studies were composed of participants with breathlessness from any malignant or nonmalignant cause, including chronic obstructive pulmonary disease, asthma, heart disease, and so on.8,12,13 Participants in the intervention group received a fan to blow air to face for five minutes and the breathlessness was evaluated shortly after intervention in three trials,8,11,16 or received daily/occasional fan therapy to face for months and the long-term efficiency on ameliorating dyspnea was assessed in two trials.12,13 The control groups were given fan to leg,8,11 or no fan, 13 as well as being accompanied by their caregivers 16 or wristband. 12 The instruments used to measure breathlessness were the Numerical Rating Scale (NRS)/Visual Analog Scale (VAS), and the modified Borg scale. The details of the five trials are presented in Table 1.
Quality assessment
The risk of bias assessments of each study are presented in Figures 2 and 3. All of the included trials were randomized design, and four studies described the randomization procedures.8,11–13 Three of five trials reported allocation concealment methods, including password-protected computer and sealed opaque envelopes.8,12,13 One and two studies did not report the specific method for randomization and allocation concealment, respectively. Owing to the nature of the intervention, blinding of the participants is almost impossible. One study stated that the patients were not blinded 13 ; one study stated that the statistical analysis was conducted blinded, but the investigators were not blinded 8 ; one study demonstrated the single-blinded design without any detail 16 ; whereas two studies did not address this issue.11,12 Two studies reported no missing data,11,16 while one study did not report reason for attrition. 8 We judged two studies at high risk of attrition bias because of substantial withdrawal proportion (48.6%) or unequal proportion of dropouts.12,13 Moreover, one study had high risk of bias of selective reporting. 12 More detailed risk of bias is listed in Supplementary Table S2.
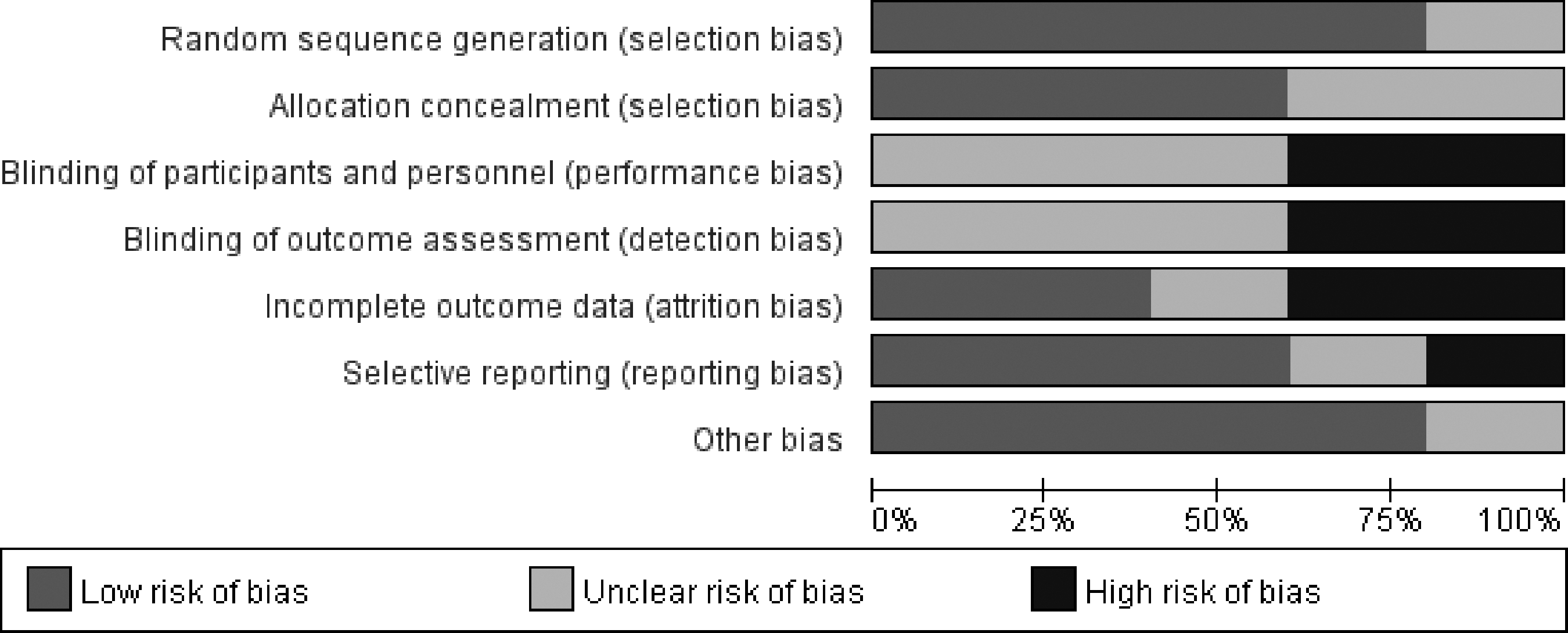
Risk of bias graph: the review authors' judgments about each risk of bias item presented as percentages across all of the included studies.

Risk of bias summary: the review authors' judgments about each risk of bias item for each included study.
Primary outcomes
Five trials (n = 198) compared the efficacy of fan therapy versus a control group on changes of breathlessness intensity. The synthesis of three trials showed that fan therapy was associated with a significant relief of breathlessness intensity immediately after intervention (MDs, −1.01; 95% CI, −1.57 to −0.45; p < 0.001) and 10 minutes after intervention (MDs, −0.90; 95% CI, −1.53 to −0.27; p = 0.005) (Fig. 4). On the contrary, the synthesis of two trials indicated that daily/occasional fan therapy for at least one month was not related to changes of dyspnea severity (MDs, 0.10; 95% CI, −1.14 to 1.35; p = 0.870) (Fig. 5).

Forest plot of the effects of fan therapy versus control on breathlessness intensity immediately after intervention and 10 minutes after intervention.

Forest plot of the effects of daily/occasional fan therapy for at least one month versus control on breathlessness intensity.
Significant heterogeneity (I 2 = 50%, p = 0.080) was present in the primary outcome analysis (Fig. 4). Restricting analysis to studies, in which participants were diagnosed with advanced cancer only, did not change the results of primary outcomes. After exclusion of one study with a high risk bias, 8 fan therapy still resulted in significant relief of dyspnea immediately after intervention (MDs, −1.31; 95% CI, −1.79 to −0.83; p < 0.001) and the I2 changed from 61% to 0%. The putative explanation is that the average of baseline breathlessness severity in Galbraith et al.'s study was lower than the others and a better baseline situation benefits less from fan therapy. 8
One included study evaluated the activity performance, including changes of average steps per day, six-minute walk test, and Australia-modified Karnofsky Performance Status. Johnson et al. compared four weeks' fan therapy (low/high flow rate) to no fan group and found no differences in activity performance between groups. 13
Secondary outcomes
One study examined the changes in facial surface temperature and two studies reported the changes in respiratory rate and SpO2. Kako et al. reported that fan-to-face therapy was associated with a more significant drop in facial surface temperature compared to fan-to-legs group (MDs, −1.44; 95% CI, −2.32 to −0.56; p = 0.001). 11 Both Kako et al. and Wong et al. presented data that changes in respiratory rate, and SpO2 were similar between fan therapy and control groups.11,16
Only one study evaluated the changes in other symptom intensities, including well-being, tiredness, lack of appetite, pain, anxiety, depression, and nausea. Kako et al. compared fan-to-face therapy to fan-to-legs group with a total of 40 patients included and found no difference in other symptoms between the groups. 11
Three out of five studies assessed adverse effects related to fan therapy, and no adverse effects were recorded.8,11,13
Discussion
Summary of results
Very few trials have evaluated the effectiveness of fan therapy for the treatment of dyspnea. This meta-analysis demonstrated low-quality evidence for a significant effect short after fan therapy compared to placebo or no fan in the relief of dyspnea in adults with advanced disease or terminal illness. Also, one study reported that fan-to-face therapy was associated with a more significant drop in facial surface temperature. 11 Potential mechanisms underlie the effect of airflow generated by fan-to-face therapy might be that the stimulation of the trigeminal skin receptors induced the diving response, or the cooling of mucosal receptors on the upper respiratory tract decreased the central respiratory drive.17–19 There is no beneficial effect of long-term use of fan therapy for at least a month to palliate dyspnea. Two possible explanations might contribute to this phenomenon. One is that the severity of breathlessness progressed day by day in people with advanced disease and terminal illness, and the other one is that participants did not use the fan consistently over time for various reasons. The activity performance, changes in other symptom intensities, respiratory rate, and SpO2 were comparable between groups.
Fan therapy is recommended by clinical guidelines and reviews to palliate dyspnea7,20,21 and it is considered as one of the core components of several breathlessness management programs, such as the Breathlessness Intervention Service or the Breathlessness Support Service.5,22 However, robust evidence to support its effectiveness is limited. This is the first meta-analysis confirming the short-term beneficial effect following fan therapy without changing respiratory parameters, partly in consistence with recently published two reviews,7,21 but querying the efficiency of long-term application of fan therapy as described above.
Overall completeness and applicability of evidence
The 5 included studies involved an average of 40 participants per study and the small sample size limited the strength of the evidence. Participants were from five different countries, representative of populations affected by breathlessness at rest, diagnosed as advanced disease or malignant disease. It is difficult to distinguish patients with different diagnosis and to determine how representative patients in the trials were in regard to baseline symptom severity, frequency, and duration of symptoms, as these were not completely reported. The variability of baseline breathless intensity exists and might contribute to the heterogeneity.
In this review, there were various comparisons in the trials included, some investigating whether fan therapy provided benefit when added to self-management/exercise advice 13 and some exploring whether fan therapy was more effective than placebo.8,11,12,16 Owing to the limited number of studies and participants, all these comparisons were pooled together at specific time points to draw conclusion. The short-term effect was evaluated after fan-to-face for five minutes, so the results may not generalize to fan therapy delivered for a longer duration. Also, whether it was still effective 10 minutes after the end of five minutes' fan therapy was unclear. In addition, the components (e.g., location, duration, flow rate, and frequency) of the long-term use of fan therapy were incompletely described in the two trials.12,13 Incomplete intervention descriptions limit reliable interpretation of the evidence; therefore it is recommended that future trialists report the details of intervention.
A variety of different outcome measures was applied in the five studies, including the Borg, NRS, and VAS. Every included study reported the primary outcome, the changes of breathlessness intensity from baseline. The other outcomes were measured in only a few trials (activity performance in one trial, changes in facial surface temperature and other symptom intensities in one trial, and changes in respiratory rate and SpO2 in two trials), which limit meta-analysis. More than half the trials (60%) measured adverse events, but none was reported, indicating the safety of fan therapy.
The quality of the evidence presented in this review was assessed by GRADE handbook. The benefit of fan therapy, we report in this review, is downgraded to low quality because of two factors. On one hand, the risk of performance and detection bias was unclear or high because of nonreported or nonblinded assessment of self-reported outcomes in these trials, which might be associated with an average of 13% exaggeration of intervention effect. 23 On the other hand, the findings were based on underpowered trials, resulting in possible imprecision of effect estimates. Accordingly, the conclusion that should be drawn with caution and further high-quality trials are warranted.
Strength and limitation
The trials included in this review were RCTs, and for crossover design, only data from the first period were obtained. Besides, this study systematically analyzed the role of fan therapy for different symptoms in adults with advanced disease and terminal illness for the first time. There are also several limitations. First, although a comprehensive search strategy and manual search were conducted, there may be relevant published or unpublished studies missed. Second, the findings were based on small samples, with insufficient statistical power to detect the truth. Third, the high variability in participants' characteristics, interventions, control groups, and outcome measurements lead to limited applicability of the results clinically. Finally, publication bias may exist due to potential invisibility of studies with negative results.
Conclusion
In conclusion, current trials provided low-quality evidence for a significant short-term effect after fan therapy in the relief of dyspnea and no beneficial effect in the long-term application in adults with advanced disease and terminal illness. Further well-designed, high-quality RCTs are needed.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.