
Abstract
Background:
In 2018, >75,000 children were newly affected by the diagnosis of advanced cancer in a parent. Unfortunately, few programs exist to help parents and their children manage the impact of advanced disease together as a family. The Enhancing Connections-Palliative Care (EC-PC) parenting program was developed in response to this gap.
Objective:
(1) Assess the feasibility of the EC-PC parenting program (recruitment, enrollment, and retention); (2) test the short-term impact of the program on changes in parent and child outcomes; and (3) explore the relationship between parents' physical and psychological symptoms with program outcomes.
Design:
Quasi-experimental two-group design employing both within- and between-subjects analyses to examine change over time and change relative to historical controls. Parents participated in five telephone-delivered and fully manualized behavioral intervention sessions at two-week intervals, delivered by trained nurses. Behavioral assessments were obtained at baseline and at three months on parents' depressed mood, anxiety, parenting skills, parenting self-efficacy, and symptom distress as well as children's behavioral-emotional adjustment (internalizing, externalizing, and anxiety/depression).
Subjects:
Parents diagnosed with advanced or metastatic cancer and receiving noncurative treatment were eligible for the trial provided they had one or more children aged 5–17 living at home, were able to read, write, and speak English, and were not enrolled in a hospice program.
Results:
Of those enrolled, 62% completed all intervention sessions and post-intervention assessments. Within-group analyses showed significant improvements in parents' self-efficacy in helping their children manage pressures from the parent's cancer; parents' skills to elicit children's cancer-related concerns; and parents' skills to help their children cope with the cancer. Between-group analyses revealed comparable improvements with historical controls on parents' anxiety, depressed mood, self-efficacy, parenting skills, and children's behavioral-emotional adjustment.
Conclusion:
The EC-PC parenting program shows promise in significantly improving parents' skills and confidence in supporting their child about the cancer. Further testing of the program is warranted.
Introduction
In 2018, an estimated 381,777 children were impacted by a new diagnosis of cancer in a parent, and an estimated 20% of parents were diagnosed with advanced disease.1,2 This scenario, of a parent dying of cancer while raising a dependent child, is an exceptionally difficult situation marked by significantly higher levels of worry and anxiety in cancer patients with children than those without. 3 These parents must cope with the disease, treatment-related symptoms, and their own emotional concerns as well as the distress the cancer might be causing their child.3–5 Although the majority of parents report wanting information and services to support their children, it is rare that they receive them. 6
The child's experience with a parent with advanced cancer is also complex and difficult. Children raised by parents with advanced cancer have significantly elevated levels of distress and depression compared with the general population,7,8 reaching or exceeding clinical levels of anxiety8,9; depression8–11 ; and often have adjustment problems on standardized measures of behavioral-emotional functioning.8,10,11 These children are known to harbor fears about their parent getting worse7,12,13 or dying from the disease, leaving the child alone or raised by someone else.7,12,14 These fears likely crescendo in the days before a parent dies, as a child anticipates the coming loss.9,15–17 Moreover, several studies of cancer-bereaved youth have shown significant long-term consequences on the child, including twice the risk of self-injury compared with nonbereaved peers and higher levels of post-traumatic stress symptoms compared with pediatric cancer survivors.17,18
Although children may be confused, sad, angry, or uncertain about the outcomes of the cancer, these emotions are frequently held back from the ill parent to not burden the parent. 7 In a recent interview study, children expressed the desire to talk with their parent about the cancer but struggled with how to have those conversations, particularly when the topic centered on the emotional experience of cancer rather than its biology. 7 Relatedly, 33% of parents with advanced cancer report difficulty with illness-related communication with their children, 16 struggle with how to initiate conversations, what to tell children about the cancer, or how often to bring it up.19,20 Parents also report difficulty in distinguishing between behaviors that might represent normal development (defiance, anger, and melancholy) and behavior caused by the parent's cancer. 19
Despite the magnitude of parents' and children's distress, only 10 intervention studies with parents with advanced cancer have been conducted since 1983, most of which involved qualitative data to evaluate outcomes, 21 only one of which was a randomized trial by Kissane et al. 22 All 10 studies measured outcomes in the parent but none in the child. Furthermore, most studies involved therapy, not psychoeducation, and required the presence of multiple family members.22,23 Such therapist-driven or conjoint therapy models are difficult to sustain and in the absence of assessed outcomes in the child, we do not know their effect on the child.
Given these gaps, our study team designed a five-session fully manualized phone-delivered behavioral intervention program for parents diagnosed with advanced cancer, the Enhancing Connections-Palliative Care (EC-PC) program (Table 1). This program was adapted from a cancer parenting program previously tested for efficacy in a six-state phase III randomized controlled trial with parents with early-stage breast cancer. 24 The EC-PC program is not a therapy-based model but derives from theories of parenting and parent–child communication.24,25 The goal of this study is to report the feasibility and short-term impact of the EC-PC program.
Description of Enhancing Connections-Palliative Care Intervention Sessions and Rationale
Materials and Methods
Study protocol
After institutional review board (IRB) approval, parents were recruited from a National Cancer Institute (NCI)-designated comprehensive cancer center through passive letter and self- or provider referral between December 2016 and February 2018. Parents were eligible if they were diagnosed with advanced or metastatic disease receiving noncurative treatment, had one or more children aged 5–17 living at home, were able to read, write, and speak English, and were not enrolled in hospice. After obtaining signed informed consent and baseline measures, parents received the program (EC-PC) from a trained nurse.
The EC-PC involved five telephone-delivered sessions at two-week intervals (Table 1). Each session began with a brief didactic text that framed the session and the value of the skill for the parent. Sessions incorporated written and interactional assignments between the parent and nurse and at-home skill-building assignments between the parent and child. All in-session and at-home assignments focused on skill- and efficacy-building exercises in communicating and supporting the child and helping the ill parent manage their own anxiety. Each intervention session was digitally recorded and monitored for dosage and fidelity using session-specific performance criteria. At the end of the fifth intervention session, parents completed the same questionnaires as those obtained at baseline.
Study measures
Depressed mood
Parental depressed mood was measured by the Center for Epidemiological Studies-Depression Scale,26–28 a 20-item self-report measure of the recent occurrence of symptoms of depression. The internal consistency reliability in three samples from the general population ranged between 0.84 and 0.8526 and was 0.85 or higher in more recent studies with cancer patients27,28; the validity of the measure is well established.29–31
Anxiety
Parent anxiety was measured by the state component of the Spielberger State-Trait Anxiety Inventory, a 20-item self-report questionnaire of the respondent's feelings of apprehension, tension, nervousness, and worry at the present moment.32–34 The internal consistency reliability in the prior EC trial was 0.96. 24
Parenting self-efficacy
Parenting self-efficacy was measured by a nine-item self-reported measure, the Help Child Scale.25,35 Items reflect the parent's confidence to talk with the child about the child's cancer-related concerns; for example, “I can assist my child to talk out his/her worries about my cancer.” The internal consistency reliability in the EC trial was 0.97. 24
Parenting quality
Parenting quality was measured by the four-item Disclosure of Negative Feelings Subscale of the Family-Peer Relationship Scale, the parent's report of the degree to which the child discloses her/his feelings with the parent.36,37 Example items include, “How likely is it that the child will share if s/he is feeling mad or angry?” The internal consistency reliability of this scale was 0.89 in the EC trial. 24
Parenting skills
Parenting skills were measured by the 14-item parent-reported Parenting Skills Checklist that reflects the interactional behaviors parents use to assist their child to disclose, discuss, and cope with the parent's cancer. The measure consists of two subscales: Elicitation, for example, “I draw out my child's concerns about the cancer,” and Connecting and Coping, for example, “I work with my child to help my child manage the child's stress related to my cancer.” The internal consistency reliabilities for these two subscales were 0.74 and 0.90, respectively, in the EC trial. 24
Symptom distress
Symptom distress was measured by the Condensed Memorial Symptom Assessment Scale, a 14-item self-report scale that measures physical and psychological symptoms patients could experience from their illness. The Physical Symptom Scale reads, “How much did this symptom bother or distress you over the past 7 days?” Items include “lack of appetite” and “dry mouth.” The Psychological Symptom Scale reads, “How frequently did these symptoms occur during the last week?” and includes items such as “feeling sad.” Internal consistency reliabilities were 0.82 and 0.72, respectively, for the two scales. 38
Child behavioral-emotional adjustment
The child's behavioral-emotional adjustment was measured by the internalizing and externalizing score and the anxious/depressed mood subscale of the Child Behavioral Checklist (CBCL), a parent-reported scale of a broad range of behavior problems in children ages 5–18.39,40 The externalizing score assesses a child's aggressive, antisocial, and undercontrolled behavior; the internalizing score measures the child's fearful, inhibited, and overcontrolled behavior. The anxious/depressed subscale consists of 13 items and includes, “Cries a lot,” “Nervous, high-strung, or tense,” “Worries,” and “Too fearful or anxious.” The internal consistency reliabilities were 0.90 for the internalizing score 0.94 for the externalizing score. 39
Study analysis
The study involved within- and between-group analyses. In the within-group analysis, participants' scores at baseline were compared with their post-intervention scores at three months using a two-tailed t-test for dependent samples with a Bonferroni correction for multiple comparisons. In the between-group analysis, scores were compared with those obtained from the experimental group of the original EC program 24 using linear mixed models.41,42
Results
The sample for the within-group analysis consisted of 26 parents: 21 diagnosed mothers, 5 diagnosed fathers, and 26 school age children: 11 males and 15 females, Table 2. The majority of parents, 14 (53.8%), were diagnosed with breast cancer; 5 (19.2%) with colorectal cancer; 2 (7.7%) with sarcoma; 1 (3.8%) with head and neck cancer, and 4 (15.4%) with other types of cancer. The majority 22 (84.6%) received chemotherapy or radiation and most 24 (92.3%) reported symptoms or side effects in the recent six months. The average time since diagnosis was 48.9 (SD 45.0, median 47.4) months. Fifty percent of the parents (13/26) scored in the clinically elevated range at baseline on depressed mood or anxiety.
Enhancing Connections-Palliative Care Demographic and Diagnosis Summary
Feasibility results for within-group analyses
For the within-group design, 148 referrals were made to the study, of which 129 met eligibility criteria. Our minimum target for recruitment was 26%; in this study 61 (47%) were recruited (Figure 1). See Figure 2 for reasons 31% of eligible patients declined participation. Our minimum enrollment goal was 25% of those recruited. In this study 42 (69%) were enrolled (consented and completed baseline measures). Of those enrolled, 26 (62%) completed all five intervention sessions and post-test measures.
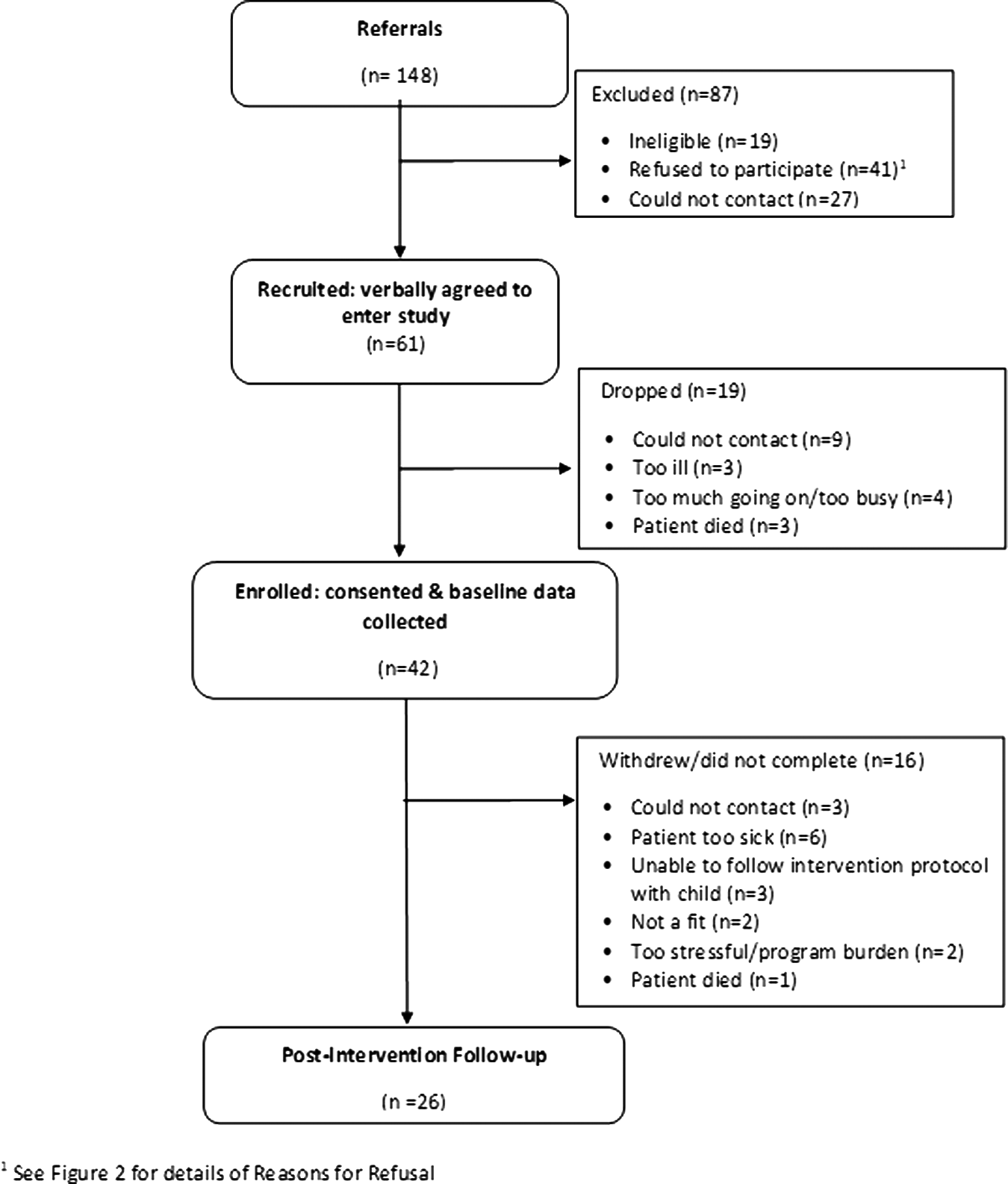
Flowchart of EC-PC participants.
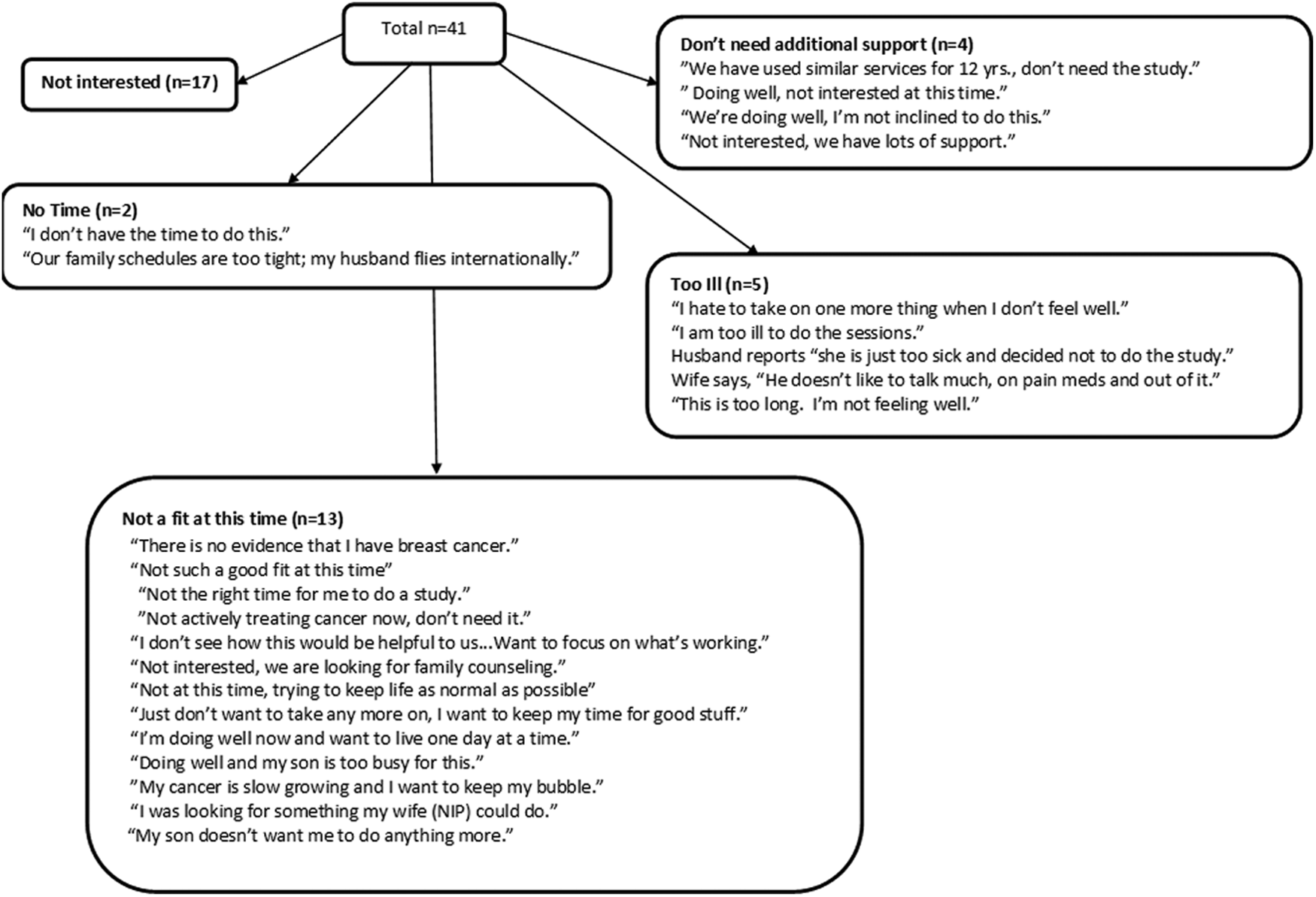
Reasons for participants' refusals to enroll in EC-PC.
After enrollment, one to four patients withdrew at the end of each intervention session for reasons listed in Figure 1. An analysis of recruitment by type of cancer revealed that 52% were mothers with breast cancer, 50% were parents with sarcoma, 39% were parents with thoracic, head, or neck cancer, and 31% were parents with gastrointestinal (GI) cancer.
Sessions ranged from a median of 21 (session 5) to 52.5 minutes (session 4). Median minutes for other sessions were session 1, 35 minutes; session 2, 33 minutes; and session 5, 21 minutes.
Within-group analyses
Before conducting the within-group analyses, parents who completed baseline data but withdrew from the study (Fig. 1) were compared with baseline measures of the retained sample on demographic, treatment data, and all outcome measures. Parents who withdrew were comparable with the retained study sample on all these measures.
To assess short-term impact, baseline scores were compared with participants' post-intervention scores at three months (Table 3). Results showed significant improvements in parents' self-efficacy in helping their child manage the pressures of the parent's cancer on the child (p < 0.006; Cohen's d = 0.85); in parents' skills in eliciting their child's cancer-related concerns (p < 0.006; Cohen's d = 0.59); and in parents' skills in connecting with and helping their child cope with the parent's cancer (p < 0.006; Cohen's d = 0.68). Even when differences between baseline and post-intervention scores were not statistically significant, all scores improved.
Results from Within-Group Analysis of Mothers' and Children's Outcomes (n = 26)
Paired t-test, two-tailed; p-values were adjusted by a Bonferroni correction for multiple comparisons.
CES-D, Center for Epidemiological Studies-Depression Scale; SD, standard deviation; STAI, Spielberger State-Trait Anxiety Inventory.
Between-group analyses
Before conducting between-group analyses comparing EC-PC with outcomes from the randomized clinical trial (n = 77), baseline scores for the two independent groups were compared on demographic, treatment, and outcome variables. Five variables were significantly different and were included as covariates in the final mixed model analyses: child age, months since diagnosis, and scores on the Cancer Self-Efficacy Help Child subscale and Parenting Skills Checklist (Elicitation and Connecting and Coping) (Table 4).
Linear Mixed Model Analyses Comparing Enhancing Connections-Palliative Care (n = 26) to EC-R01 (n = 77), Adjusted for Covariates
Comparison of EC-PC to EC R01.
Comparison of outcomes between EC-PC and ECR01.
CASE, Cancer Self-Efficacy Help Child subscale; EC-PC, Enhancing Connections-Palliative Care; FPRQ, Family-Peer Relationship Scale; SE, standard error.
Between-group analyses, adjusted for covariates, showed that improvements on the EC-PC were comparable with improvements on all outcomes in the original trial. Specifically, the cancer parenting program in both studies resulted in comparable improvements on parental anxiety, parental depressed mood, parenting self-efficacy in helping the child, both subscales of the Parenting Skills Checklist, and on the child's behavioral-emotional adjustment (internalizing, externalizing, and anxious/depressed scores of the CBCL).
Relationship between symptom distress and outcomes
Distressful symptoms can potentially affect a parent's ability to carry out the EC-PC program. Exploratory analyses examined the relationship between parents' symptom distress, attrition, and outcomes. There was no significant relationship between parents' symptom distress and attrition. Although patients who withdrew had higher scores at baseline on symptoms than study completers, differences were not statistically significant. Scatter grams were used to examine whether changes in symptoms over time were related to changes in outcomes over time (Figs. 3 and 4). The pattern was the same for all analyses: changes in parents' symptoms never significantly covaried with changes in any of the outcomes.
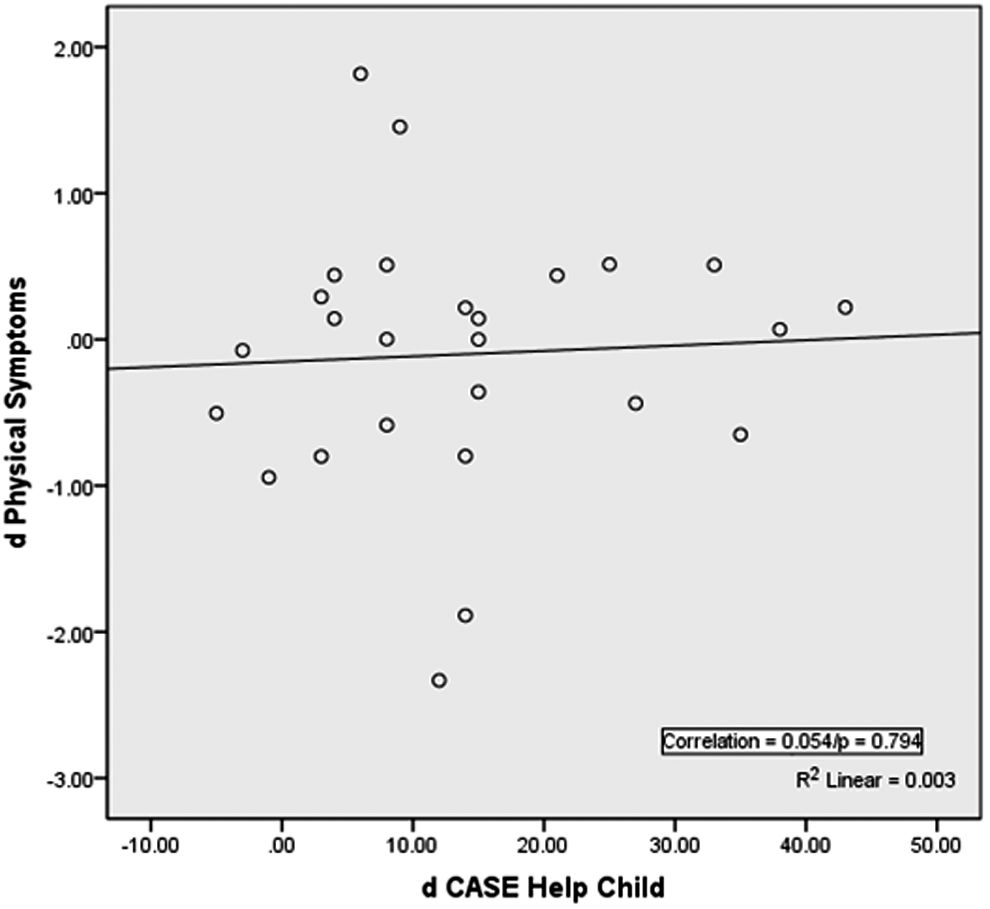
Change in physical symptoms by change in Cancer Self-Efficacy Help Child subscale.
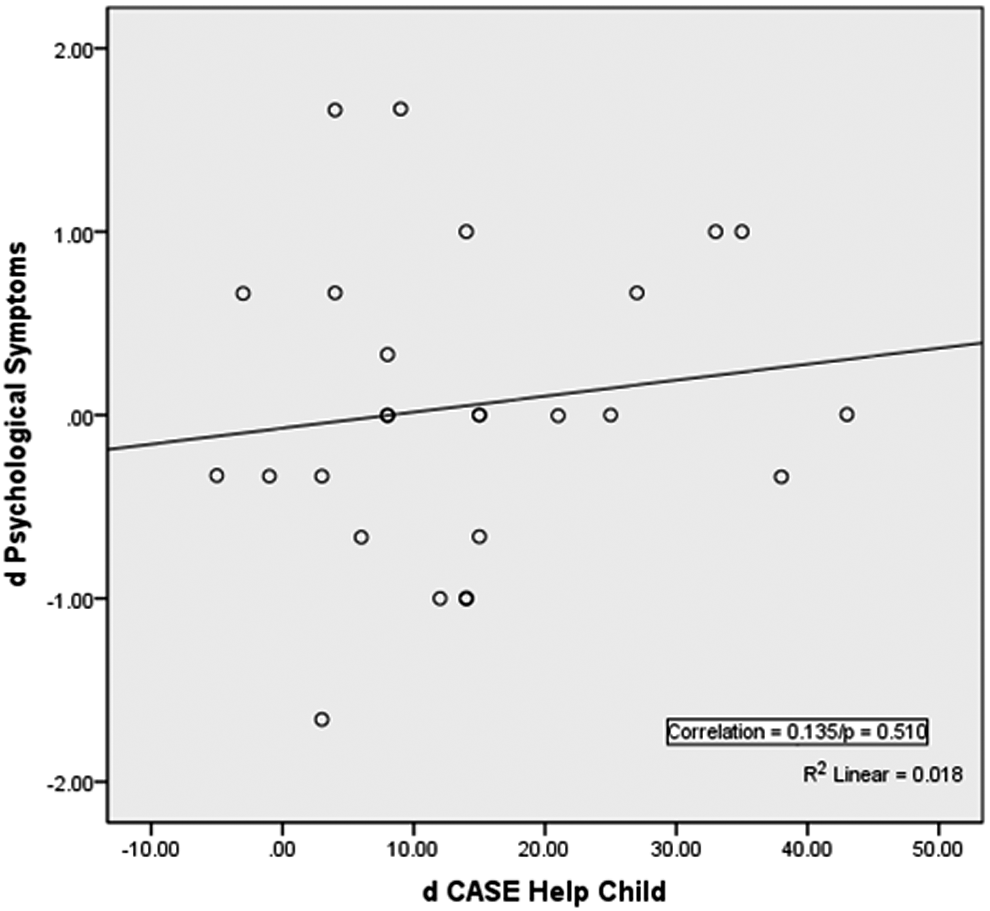
Change in psychological symptoms by change in Cancer Self-Efficacy Help Child subscale.
Discussion
This is the first fully scripted telephone-delivered cancer-related parenting program for child-rearing parents with advanced cancer. Results revealed that the EC-PC was feasible: parents were recruited, enrolled, and retained, were able to engage with the nurse educator during each of the five intervention sessions, and were able to carry out the at-home assignments with their dependent child.
The intervention significantly improved parents' skills and self-confidence in helping the child talk about and better cope with the parent's advanced disease. Parents' depressed mood, anxiety, and parenting quality were not significantly improved in the within-group analysis. We speculate that the everyday reality of noncurable disease precluded changing parents' affect and mood. Although parents' depressed mood was not significantly improved, it is notable, and reassuring, that mood did not appear to be a barrier to their completing the program. Likely the absence of changes in parenting quality was a measurement problem. Future studies need to include a more sensitive measure of parenting quality. Although there was a tendency for the child to be less anxious and depressed, these improvements were not statistically significant, possibly due to the small sample size in the within-group design.
All changes on study outcomes in the between-group analyses were statistically comparable with results obtained in the original EC program. This means two things: EC-PC achieved the same magnitude of improvements for parents and children dealing with advanced cancer as those facing early-stage breast cancer. Second, a telephone-delivered intervention resulted in the same magnitude of change as did in-person delivery.
Consistent with other trials with advanced cancer patients, there were challenges to recruitment and retention. A large number of referred patients were ineligible or could not be contacted, including 27 patients who could not be reached despite four attempts. Figure 1 summarizes reasons 16 patients withdrew after consenting (n = 16), including: not reachable (n = 3) and too sick or died (n = 7). Figure 2 contains reasons patients declined enrollment. Despite these challenges, 68.9% of eligible patients enrolled and 61.9% of enrolled patients completed all five sessions. In this context, the high completion rate is evidence of the value of the program to these parents.
When both the within- and between-group analyses are considered, EC-PC has potential to positively enhance parents' skills and competencies and reduce the emotional burden of parents' advanced cancer on the children. Recall that all changes occurred in five scripted telephone intervention sessions that totaled only 3.3 contact hours within a 10-week period and were not affected by time since diagnosis or patients' symptoms.
Study limitations
Study results should be viewed with caution. Outcome measures in both the within- and between-group analyses were limited to parent-reported data that were potentially affected by self-enhancement, recall, or social desirability bias. Future research should include child-reported responses to the program, including exit interviews. The study sample consisted of primarily well-educated white mothers and results may not reflect outcomes with less well-educated or more diverse parents. Despite these limitations, study findings suggest that the EC-PC warrants further testing with a larger more diverse sample within a randomized controlled trial.
Footnotes
Acknowledgments
We acknowledge the contributions of referring physicians, dedicated site intermediaries at the Seattle Cancer Care Alliance and Taryn Oestreich. We dedicate this article to the families who participated in this study, our greatest teachers.
Funding Information
This research was supported by grants from the National Cancer Institute, NIH under award number R01 CA 78 424 (Lewis, PI), the Seattle Cancer Consortium, Safeway Foundation, and donations to the Thoracic, Head and Neck Oncology Research Program of the Seattle Cancer Care Alliance.
Author Disclosure Statement
No competing financial interests exist.
The content of the article is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health.