
Abstract
Background:
There is increasing need for nonspecialty physicians to deliver palliative care (PC) services to meet patient needs, but many physicians feel inadequately prepared.
Objective:
We aimed to improve the PC skills of resident physicians through a learner-centered, just-in-time coaching intervention.
Design:
Our quality improvement initiative consisted of two didactics and brief thrice-weekly coaching sessions that focused on real-time PC questions. Upper level internal medicine residents participated during an inpatient hospitalist rotation.
Measurements:
Residents completed pre/postrotation surveys of their preparedness in discussing PC topics. Electronic medical record data of documentation of goals-of-care (GOC) discussions and Physician Orders for Life-Sustaining Treatment (POLST) completion in at-risk hospitalized patients (age >65 with two or more hospitalizations in the past six months, or age >90) were obtained and compared with before hospitalization. These data were also compared with data from patients on the same resident hospitalist service during the six-month period before the intervention began.
Results:
During the 14-month intervention period, 42 residents cared for 232 at-risk patients. Among at-risk patients, 12.9% had a documented GOC discussion before hospitalization, which rose to 57.3% before discharge. Among at-risk patients preintervention, these rates were 5.2% and 25.0%, respectively. Residents reported their preparedness increased across many elements of GOC discussions and rated coaching sessions as useful and relevant to their training. Rates of POLST completion did not differ between preintervention and intervention groups.
Conclusions:
Brief coaching sessions can integrate PC education into a busy clinical service, improve residents' primary PC skills, and improve GOC documentation.
Introduction
The role of palliative care (PC) in hospitalized patients has expanded as data confirm its role in improving symptom control and patient-centered care. 1 Despite this, the demand for PC services, including assistance in managing uncontrolled symptoms, discussing goals of care (GOC), and providing emotional support to patients and families, far exceeds the supply of specialty clinicians able to deliver PC services. This has led to unmet PC needs in hospitalized patients.2–5 There is increasing awareness of the need for all clinicians to develop primary PC skills. 5
An important part of PC is to discuss patients' GOC. Such conversations are essential to ensure that their treatment plans align with their values, 6 and have been associated with improved patient and family outcomes.7,8 However, often these discussions occur late in the illness course during acute hospital care, 9 are brief, and do not focus on patient-specific goals and clinical situations. 10 Resident physicians frequently are responsible for initiating GOC discussions and facilitating end-of-life (EOL) care, but frequently feel uncomfortable or inadequately prepared to deliver PC services or conduct GOC conversations with their patients.11–13
Educators have devised numerous teaching strategies to improve resident physicians' PC skills, including formal lectures, online modules, small group discussions, and role play, with a multimodality approach generally regarded as the most effective.14,15 However, competing clinical demands, duty hour restrictions, and difficulty in applying formal didactics to real-life conversations may limit the effectiveness of these interventions.
Recently, medical educators have developed innovative educational methods to promote behavior change. Adult learning theory is based on the principles that education should be immediately relevant, experiential, problem-based, and integrated with the demands of daily life.16–18 One such educational method is just-in-time teaching, which optimizes active learning through a focus on real-time questions, misconceptions, and issues. 19
We sought to apply principles of adult learning and just-in-time teaching to primary PC education among internal medicine residents. Our team developed a new curriculum using a learner-centered, just-in-time coaching intervention aimed to improve PC skills of residents. In particular, we evaluated whether this novel educational intervention could increase residents' preparedness in discussing PC topics and completion of GOC discussions with at-risk hospitalized patients.
Methods
Study setting
This prospective quality improvement (QI) study involved upper level (postgraduate year (PGY) 2 and 3) internal medicine residents at a large urban medical center. This medical center had an average of 2448 admissions and 111 inpatient deaths per month during the 2018 calendar year. Most of these admissions were covered by Medicare (54.5%); other forms of patient insurance included Medicaid (18.5%), commercial insurance (22.1%), and self-pay or other (5.0%).
The PC team at this medical center, which sees an average of six to eight new consults per day, is composed of two full-time PC physicians, two advanced practice providers, and two to three social workers. Meanwhile, medical residents receive didactics in PC in various contexts, including noon conferences, ambulatory lectures, and elective PC rotations. Residents' assigned hospitalist rotation was chosen for our project because of the medical complexity of the patient population, which has longer length of stays and more comorbidities than other hospital units. During residents' hospitalist rotation block, each of three medical residents independently cared for eight patients on a single floor under the supervision of a hospital medicine attending. The objective of this rotation is to prepare residents for independent practice postresidency by managing medically challenging patients on their own with guidance and formative feedback from an attending. The QI intervention occurred over a span of 15 rotation blocks, from June 24, 2017, through August 26, 2018, excluding a 10-day period during the winter holiday season. Most rotation blocks were four weeks long (one two-week rotation and two five-week rotations).
Intervention
The intervention was composed of two parts. The first part consisted of two brief (15–20 minutes), interactive didactic sessions that provided an overview of a GOC communication roadmap and instruction on appropriate documentation of GOC conversations. The second part involved informal thrice-weekly coaching sessions on all domains of PC. All sessions were led by a PC physician with several years of clinical experience (A.T., R.M.A., or J.C.). The GOC communication roadmap, described in detail elsewhere, provides a framework for negotiating complex conversations and promoting shared decision making with patients. 20 The second structured educational session reviewed how to appropriately record GOC discussions within the electronic medical record (EMR). The didactic sessions occurred early during each four-week block, generally within the first two weeks.
The coaching sessions were designed to be informal, flexible, and brief (between 10 and 20 minutes), and centered on building primary PC skills through topics chosen by the learners based on patients for whom they were currently caring. During these learner-driven coaching sessions, residents were encouraged to bring up PC questions related to contemporary patient care, including advance care planning, GOC, pain, other symptoms, and disposition. PC providers discussed these real-time issues and promoted residents' self-efficacy in primary PC without need for a formal PC consult, although residents were not prohibited from doing this if they felt it was necessary. All didactics and coaching took place in the residents' work room adjacent to the patient care unit. After each coaching session, the PC physician logged details about the session into an electronic database, including the number of residents coached, session length, and specific types of questions or topics residents raised.
Measures
We collected demographic information from residents and measured residents' self-perceived preparedness in having GOC discussions with pre- and postrotation surveys. A 5-point scale was used for each survey item (from 1—not well prepared to 5—very well prepared). The postrotation survey also included items addressing residents' perception of the usefulness of the didactics and coaching, rated on a 5-point scale (from 1—poor to 5—excellent). The survey was e-mailed to residents to complete electronically at the beginning and end of each rotation. A follow-up e-mail was sent two weeks following each rotation to encourage completion of surveys.
We measured the frequency of documentation of GOC discussions in “at-risk” patients during hospitalization compared with the frequency of documentation of GOC discussions in these patients prehospitalization. At-risk patients were defined as patients older than 65 years with at least two hospitalizations in the past six months, or patients older than 90. GOC discussions were documented in a GOC template available as an embedded section in the history and physical note and progress notes as well as available as a stand-alone note. The GOC template included “clickable” segments on clinicians and family members in attendance and topics discussed (e.g., disease information, prognosis, patient values, and preferences), as well as a free text space in which details of the discussion could be recorded. Data collected from the EMR also included patient demographics (age, sex, race, admitting diagnosis), code status documentation (cardiopulmonary resuscitation [CPR] yes, CPR no, comfort measures only [CMO], or assessment needed), and formal PC consults (yes/no). From those patients with a limited code status (CPR no or CMO), a record of Physician Order for Life-Sustaining Treatment (POLST) completion (yes/no) was obtained. These EMR data during the intervention period were also compared with data of at-risk patients on the same resident hospitalist service during a six-month period preintervention (January 1, 2017, through June 23, 2017). Physician outcomes were not measured during the preintervention period.
Data analysis
Wilcoxon–Mann–Whitney U tests were performed to analyze pre/post changes in residents' level of preparedness. All tests were two-tailed, and a p-value of 0.05 was considered significant. Paired t-testing was unable to be performed due to inability to match pre- and postrotation survey responses for the first three rotation blocks.
Results
Resident physician demographics
A total of 46 residents were assigned to the hospitalist rotation between June 2017 and August 2018 and cared for a total of 232 at-risk patients. Due to scheduling conflicts, two residents split coverage during the single two-week block, leading to four residents in one block; these two residents were excluded from analysis. Meanwhile two residents completed the rotation twice; only their responses from their first rotation were included in data analysis. Thus, 42 residents were included in our study sample, comprised of 12 female PGY2s, 13 female PGY3s, 8 male PGY2s, and 9 male PGY3s (Table 1). Of 37 (88%) residents who took the prerotation survey, 33 (79%) completed the postrotation survey.
Resident Demographics (n = 42)
Data available for 37 residents.
Coaching sessions and topics brought up by residents
Over the course of 15 rotations, a total of 167 coaching sessions were completed by PC physicians, averaging 16 minutes (SD 8.2 minutes) three times per week. A total of eight coaching sessions were not documented during the first four months of the intervention. The median number of residents who attended each coaching session was 3 (IQR 1), and the overall rate of attendance at the recorded coaching sessions for each rotation block was 83.9%. The question topic most commonly brought up by residents during these sessions centered on communication, including talking with patients, families, or other clinicians (altogether, 68.3% of total question topics raised). Other topics raised related to pain (9.7%), nonpain symptoms (9.2%), disposition (7.1%), and ethics (4.9%) (Fig. 1). Specific questions ranged from addiction/drug-seeking behavior, treatment recommendations, prognostication, artificial nutrition in advanced diseases such as dementia, GOC documentation, advance care planning, and hospice.
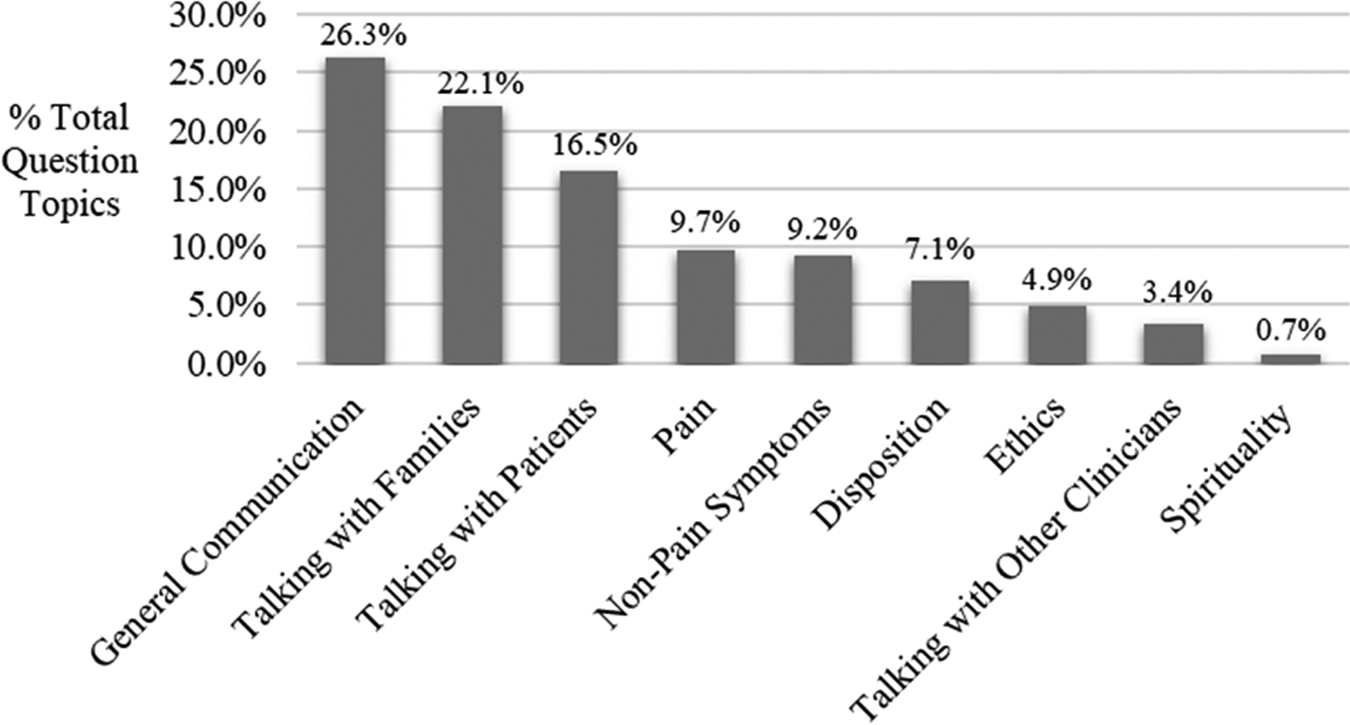
Question topics brought up by residents (n = 411) as reported by palliative care faculty over 167 coaching sessions.
Survey data pre- and postrotation
Residents reported that their level of preparedness increased across many GOC topics (Table 2). The greatest increases were in eliciting how patients would like their surrogates to approach decisions (change +0.84, p < 0.01), eliciting patients' fears about the EOL (+0.77, p < 0.01), helping patients ask care providers questions (+0.75, p < 0.01), helping patients complete advance directives (+0.72, p < 0.01), and helping patients talk with their families about the future (+0.70, p < 0.01).
Change in Residents' Preparedness in Addressing Palliative Care Topics Pre- and Postrotation
Residents' level of preparedness was measured on a 1–5 scale (1—not well prepared to 5—very well prepared).
Overall, residents rated the intervention highly: the topic content was relevant to their internal medicine training (mean 4.4 ± 0.5), the PC training was important for development of individual clinical skills (4.4 ± 0.6), and informal coaching with PC faculty was useful (4.6 ± 0.7). Residents rated the usefulness of didactic sessions somewhat lower (4.0 ± 0.8).
GOC documentation during the intervention period: Prehospitalization versus before discharge
Among at-risk patients cared for by residents during the intervention period, 12.9% had a documented GOC discussion before hospitalization, which rose to 57.3% before discharge. This increase persisted across all months of the intervention (Fig. 2).
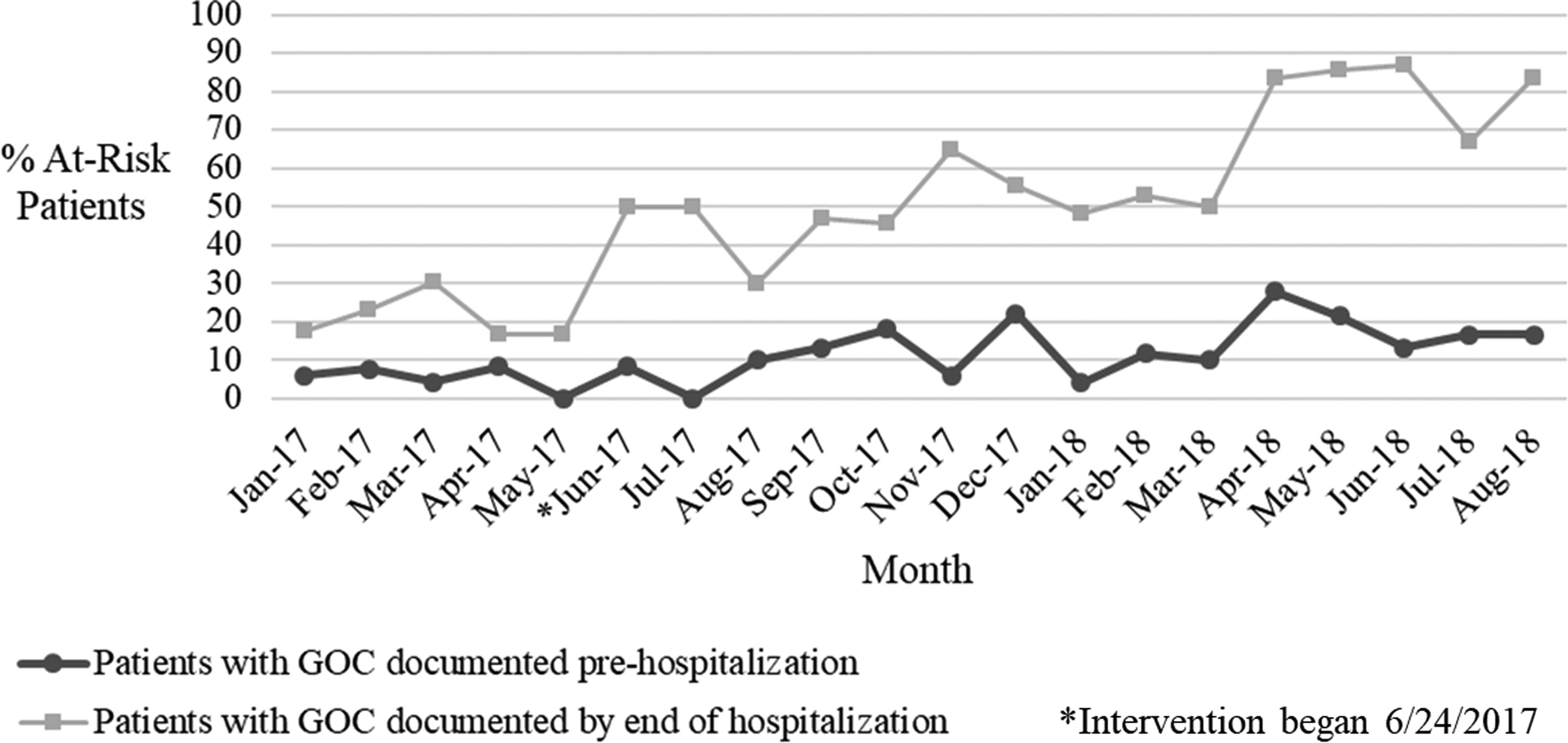
Prehospital versus predischarge percentage of at-risk patients with documented GOC discussions. GOC, goals of care.
Comparison with the preintervention period
Among at-risk hospitalized patients cared for by residents during the six months preintervention, 5.2% had a documented GOC discussion before hospitalization, which increased to 25.0% before hospital discharge (Fig. 2). As above, this percentage of predischarge GOC documentation increased to 57.3% during the intervention period. Among at-risk patients, 34.4% (33 of 96 patients) and 37.1% (86 of 232 patients) had a documented limited code status (CRR no or CMO) preintervention and post-intervention, respectively. Of these patients with limited code status, the percentage of those with a completed POLST did not differ between pre- and post-intervention, at 42.4% versus 39.5%, respectively (14 of 33 patients vs. 34 of 86 patients, respectively). Rates of formal PC consultations for at-risk patients were similar during the preintervention and intervention periods (14.6% vs. 13.4%, respectively).
Discussion
In this quality improvement initiative, we found that brief, learner-centered, just-in-time coaching sessions with PC faculty improved upper level internal medicine residents' preparedness in discussing GOC and increased GOC documentation in hospitalized, chronically ill patients.
While other studies have focused on the effect of educational interventions on perceived competence and self-efficacy,15,21 this study is one of few assessing changes in clinician behavior. To our knowledge, our study is the first to provide evidence for how a coaching intervention focused on building PC skills in resident physicians may lead to changes in clinician behavior. Coaching, a resource in which individuals with expertise and experience within a relevant field provide feedback to facilitate the development of new behaviors, insights, and approaches, 22 has garnered expanding interest in clinical education. 23 Within PC, a pilot study of in-person peer coaching showed potential for supporting clinicians in building primary PC skills in the inpatient setting. 24 Overall, however, studies evaluating the effectiveness of coaching interventions in medical education have been limited. 22
Documentation of GOC discussions in patients who were especially likely to benefit from such discussions based on age, comorbidities, and frequent hospitalizations, rose substantially, from 12.9% prehospitalization to 57.3% by the end of their hospital stay. While ideally documented GOC conversations should reach 100%, our results reflect positive movement toward making sure that patients' care is consistent with their wishes. 6 In an era in which a clear, easily accessible record of prior GOC discussions is a crucial step in delivering care concordant with patients' values, 25 our intervention of short, just-in-time coaching sessions empowered residents to conduct and document GOC conversations with chronically ill patients and thereby improve communication among providers.
In the subset of at-risk patients with limited code status, POLST form completion did not differ in the time periods of pre- and post-intervention. The overall number of patients who had a POLST at discharge was disappointing, remaining at far less than 50%. Given the intervention's success in improving GOC documentation and resident confidence level, this finding is surprising. However, the didactic sessions focused on conducting and documenting the GOC conversation, without specific emphasis on POLST unless residents asked about it. Nonetheless, as orders for life-sustaining treatment are likely to improve EOL care and minimize in-hospital death more than completion of simply advance directives, 26 this is an area we will consider for another QI intervention.
In addition to increased GOC documentation, residents reported a significant increase in level of preparedness across many elements of GOC discussions, including eliciting patients' thoughts about the future, discussing surrogate decision making, and making treatment recommendations based on patients' values. Given the acute shortage of PC trained providers as well as concern about further fragmentation of care if PC specialists are charged with providing the bulk of psychosocial support, primary PC skills are crucial for resident physicians to develop.2,3,5 Increased preparedness in navigating often emotionally laden, complex GOC conversations is an important step toward acquisition of these skills. Moreover, the time burden imposed on both the resident participants and the PC attendings who conducted the informal coaching sessions was modest (∼45–50 minutes a week), making this intervention a feasible, potentially sustainable approach to improving residents' primary PC skills. In addition, participants' continued expressions of interest in and gratitude for PC education made this intervention particularly enjoyable for PC faculty.
Notably, 73% of our residents reported having prior PC training, potentially reflecting a group more highly skilled in PC than most. This may have led to a smaller change in behavior than in a group of less skilled residents. In such a group of residents with less PC skills at baseline, the intervention may have had an even more pronounced effect on pre/post change in GOC documentation as well as on resident preparedness.
Interestingly, but perhaps unsurprisingly, our residents preferred the just-in-time coaching sessions to the two short didactics, even when the didactic sessions were informal and interactive. We also obtained informal feedback from a focus group of residents who confirmed that they preferred case-specific role play and troubleshooting over formal didactic sessions. Residents' high rating of the coaching sessions, as well as nonparticipants' expression of interest in expanding this intervention to other inpatient physician services at our hospital, reflects success of this educational approach. Their preference for coaching is consistent with adult learning theory.16,17 Based on resident focus group feedback, we made changes to the curriculum for the next Plan-Do-Study-Act cycle during the following academic year, including informal didactic sessions on prognostication and hospice disposition options while continuing thrice-weekly coaching sessions. It may also be useful for future research to incorporate predischarge patient surveys to further evaluate the effect of the intervention on residents' PC skills and behaviors.
A strength of this study is its inclusion of objective data from the EMR looking at patient outcomes. Several limitations exist. First, residents' improvement in PC skills relied on self-report; residents' PC skills and communication were not directly observed or formally assessed. In addition, the scale used had not previously been validated in prior studies. It is unknown whether or not the self-reported increase in self-preparedness is a clinically meaningful change. Individual pre/post-intervention trends are also unknown as paired t-testing was unable to be performed. Also, we did not evaluate the impact of the intervention over a longitudinal period, so we do not know if improvements will be sustainable and translate into improved patient-centered outcomes. Like most educational interventions, 15 we used a pre/post design without a control group; although our team had attempted this initially, there were many barriers in selecting a comparable physician sample. Finally, although we found an improvement in documentation of GOC conversations, we were unable to evaluate the quality of these discussions, including whether patient-specific values were discussed and whether patient/clinician understanding was concordant.8,27
In conclusion, brief, just-in-time, learner-centered coaching sessions comprise a novel educational strategy that can improve resident physicians' primary PC skills and lead to improved GOC documentation. This educational intervention offers a potential solution in the development of an effective PC curriculum14,15 that ultimately could contribute to a more sustainable model of how PC is delivered.
Footnotes
Acknowledgments
The authors thank Megan Glance and the Wolff Center for assistance in patient data extraction and analysis.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Disclosure Statement
No competing financial interests exist.