
Abstract
It was recently estimated that only 30% of Canadians have reliable access to palliative care services. Allocating funding to improve access to skilled palliative care in rural or remote settings is challenging in an era of increasing demand and competing priorities, underscoring the need for innovative palliative care service delivery that optimizes use of low-cost readily available technology. This study evaluated the use of the FaceTime application on an Apple iPad to improve timely access to physician consultation for home-based palliative care patients living in rural Nova Scotia. Patients enrolled with the Hants Community Palliative Care Program who consented to participate (n = 15) received regular home-based visits from a palliative care nurse who used the FaceTime application to connect with the palliative care physician in Halifax. Participants were then asked to complete a questionnaire evaluating their experience. Results indicated that using FaceTime through cellular data networks is feasible in rural areas of Nova Scotia. All participants reported that both the audio and visual quality allowed them to communicate easily with the doctor, and no consultations were terminated due to network instability. Patients also found the FaceTime encounter highly acceptable with 86% reporting they were “satisfied” or “very satisfied”; 100% stated that their medical concerns were addressed and 100% were willing to use FaceTime again. The results add to the limited literature exploring the application of telehealth in palliative care and demonstrating the utility of low-cost commonly used technology to improve access to palliative care in underserviced areas.
Introduction
Providing consistent access to skilled palliative care in rural settings is a challenge. It is estimated that only 30% of Canadians have reliable access to palliative care services 1 with Canada recently ranked 11th in quality of death and 18th in availability of palliative care services in a widely cited report. 2 The Canadian health care system has been slow to embrace technology that could improve health care services and result in cost savings. 3 One such opportunity is the adoption of widely available mobile video technology to improve access through telehealth consultation. Currently, the Nova Scotia Health Authority maintains an institution-based telehealth consultation system that is inaccessible to those who lack the means or are too ill to travel to access a hospital-based hub. Mobile video technology is better suited to the rural home-hospice environment where accessing in-person consultation is challenging and utilizing institution-based telehealth services is not feasible.
Background
Over the past two decades, there has been a growing evidence base supporting the use of mobile video platforms such as FaceTime across a variety of health care settings.4–14 Reports of use of telehealth in the provision of hospice and palliative care services are more limited. A 2010 review of palliative care telehealth in the United Kingdom reported that the most common applications included out-of-hours telephone support, advice for patients, caregivers and health professionals, interactive case discussions, consultations, and education of health care staff. 15 Mobile phone-based telehealth has been utilized to monitor symptoms in patients living at home with both patients and clinicians reporting positive outcomes. 16 Results from a study examining satisfaction with using video calls to determine whether a home visit was necessary led to wide-scale adoption of video triage as an integral part of providing hospice care to patients living in remote areas of Kansas and Missouri. 17 A larger study evaluating telehospice services as a supplement to traditional home-based care among four different sites showed mixed results. Although ∼60% of patients reported that they felt that telehospice positively influenced their end-of-life care and that they valued the service, they also indicated that it was not the same as in-person visits and nurses also reported a preference for in-person visits. 18
Rationale
The Nova Scotia Health Authority's Central Zone Palliative Care Service is based in Halifax and provides consultative palliative care services to ∼40% of the provincial population. Many patients live in rural settings that lack consistent access to services.
The Hants Community Hospital located in Windsor, Nova Scotia, serves a rural population encompassing the municipalities of West Hants County. Primary and consultative palliative care services are provided at home, in hospital, and in ambulatory settings. Care is coordinated by a palliative care liaison nurse working with community-based primary care nurses, family physicians, and hospitalists to support patients in their setting of choice. The nurse is supported by twice monthly visits from a palliative care physician from the Central Zone Palliative Care Service.
Patients, however, commonly experience changes in status that require urgent reassessment in the interval between scheduled palliative care physician visits. When this occurs, the palliative care nurse provides follow-up at home and contacts the palliative care physician by phone for direction when modification to the treatment plan is required. In our study, we aimed to assess the feasibility of using FaceTime over a mobile cellular data network to provide these patients with improved access to specialist palliative care by enabling the palliative care physician to provide direct assessment and advice through a video-based interaction with the patient, caregivers, and palliative care nurse.
Methods
Design
This was an observational study exploring technical feasibility and patient satisfaction with mobile telehealth services.
Participants
Patients (n = 15) who were enrolled in the Hants Community Palliative Care Program and were receiving ongoing home-based palliative care follow-up by the palliative care liaison nurse and palliative care physician were eligible to participate. Known availability or access to the Internet was not a criterion for patient participation in the study. Patients with significant hearing or visual impairments that precluded interaction by video were excluded.
Materials
Equipment
An Apple iPad Air 2 with Wifi and cellular data connectivity was utilized by the visiting palliative care nurse and the remote palliative care physician to establish a video link with the participants. The Apple FaceTime video platform is a standard feature of iOS devices and is capable of transmitting end-to-end encrypted video over both Wifi and cellular data networks. The Bell Cellular Long-Term Evolution-Advanced (LTE-A) network was used to transmit all interactions.
Intervention
The community palliative care nurse was given an Apple iPad with the FaceTime application installed and a cellular data package. The nurse brought the Apple iPad to all home-based palliative care follow-up visits that occurred in the interval between regularly scheduled physician visits. These visits were triggered by a change in clinical status requiring reassessment. Using FaceTime on the Apple iPad, the palliative care nurse contacted the palliative care physician in Halifax facilitating direct patient, caregiver, and nurse interaction with the physician, and where required, adjustment of the management plan. Patients continued to have access to standard in-person physician assessment and follow-up during biweekly palliative care physician visits to Windsor.
Outcome measures
We utilized a paper-based survey to assess patient satisfaction with the consultation including the video, audio, and connection quality. Responses were rated on a 5-point Likert scale, ranging from very dissatisfied to very satisfied. Participants were asked to complete the survey within seven days of the consultation and return it by mail in a pre-addressed postage-paid envelope. All data were recorded in aggregate form and analyzed using descriptive statistics.
The following criteria were used to assess the feasibility of our intervention:
Feasibility criteria
Video/audio quality
≥70% of participants report that the video quality was sufficient to communicate effectively with the palliative care physician (≥4/5).
≥70% of participants report that the audio quality was sufficient to communicate effectively with the palliative care physician (≥4/5).
Connection stability
≤30% of video consultations terminated due to unsatisfactory video link
Patient/caregiver satisfaction
≥70% of participants rate their overall satisfaction with the video consultation as satisfied or very satisfied (≥4/5).
≥70% of participants report that video consultation adequately addressed their medical needs and concerns (≥4/5).
≥70% of participants agree or strongly agree that they would be willing to utilize mobile video telehealth again (≥4/5).
Results
Between January 1 and August 15, 2017, 15 patients conducted a home-based video consultation with the palliative care physician. Patient demographics are outlined in Table 1. Caregivers were present for only two of the consultations. Questionnaires were returned for 14 of 15 encounters (response rate 93%). Thirteen of 14 questionnaires were completed by the patient, 1 of 14 questionnaires was completed by the caregiver because the patient was so ill.
Patient Demographics
Feasibility
One hundred percent of respondents reported 4 of 5 or greater satisfaction scores for audio and video quality. There were two instances wherein FaceTime calls were dropped; however, the connections were immediately reestablished and the consultation was completed. No encounters had to be aborted due to network instability. Figure 1 shows the mean patient/caregiver satisfaction scores for audio, video, and overall connection quality.
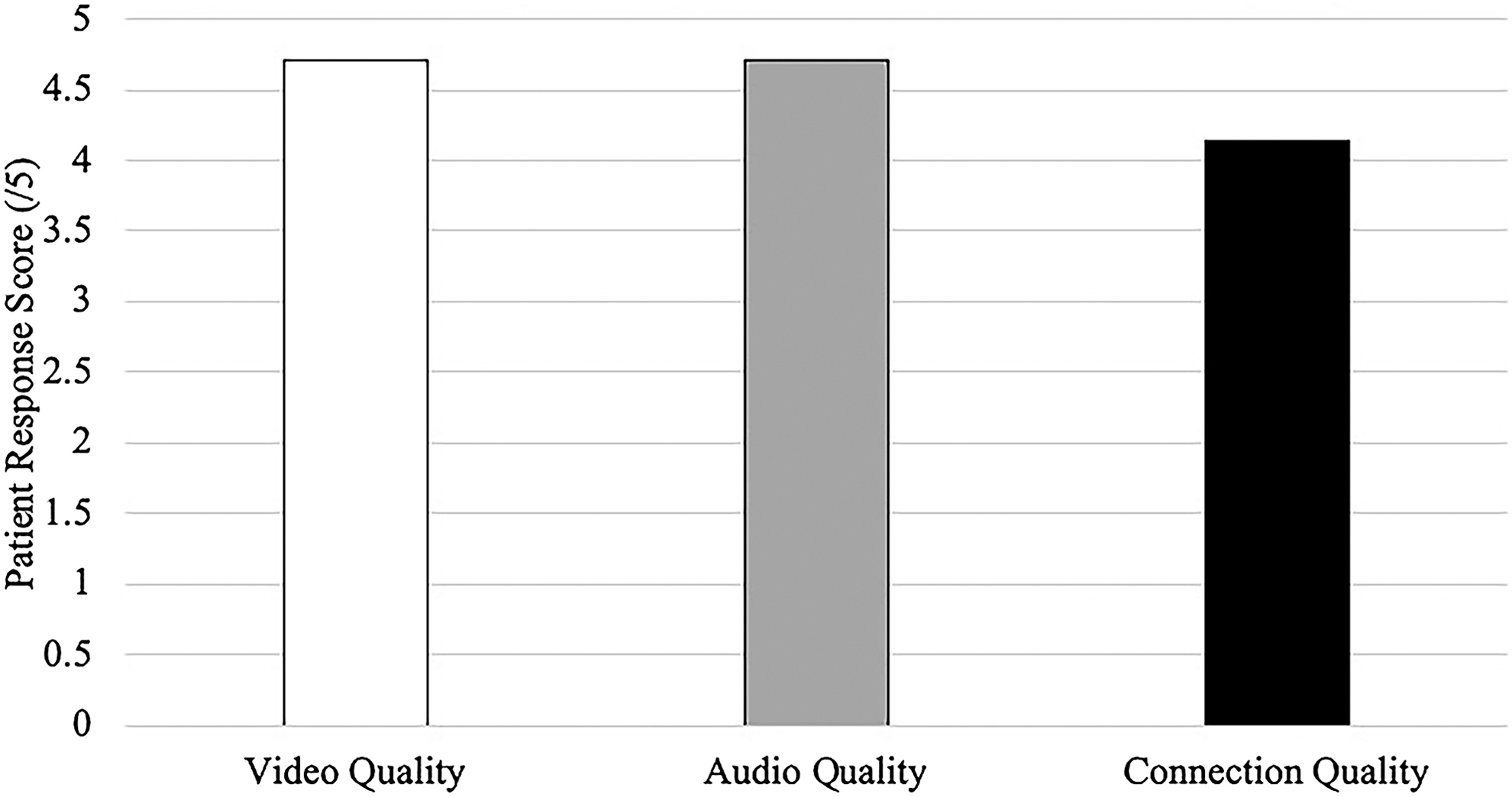
Mean participant ratings for audio, video, and connection quality.
Acceptability
Acceptability results are summarized in Table 2 and Fig. 2. Eighty-five percent of respondents reported they were “satisfied” or “very satisfied” with their experience. All patients reported being “satisfied” or “very satisfied” (mean rating = 4.71) that their medical concerns were addressed. All patients reported that they “agreed” or “strongly agreed” that they were willing to use the technology again (mean rating = 4.64).
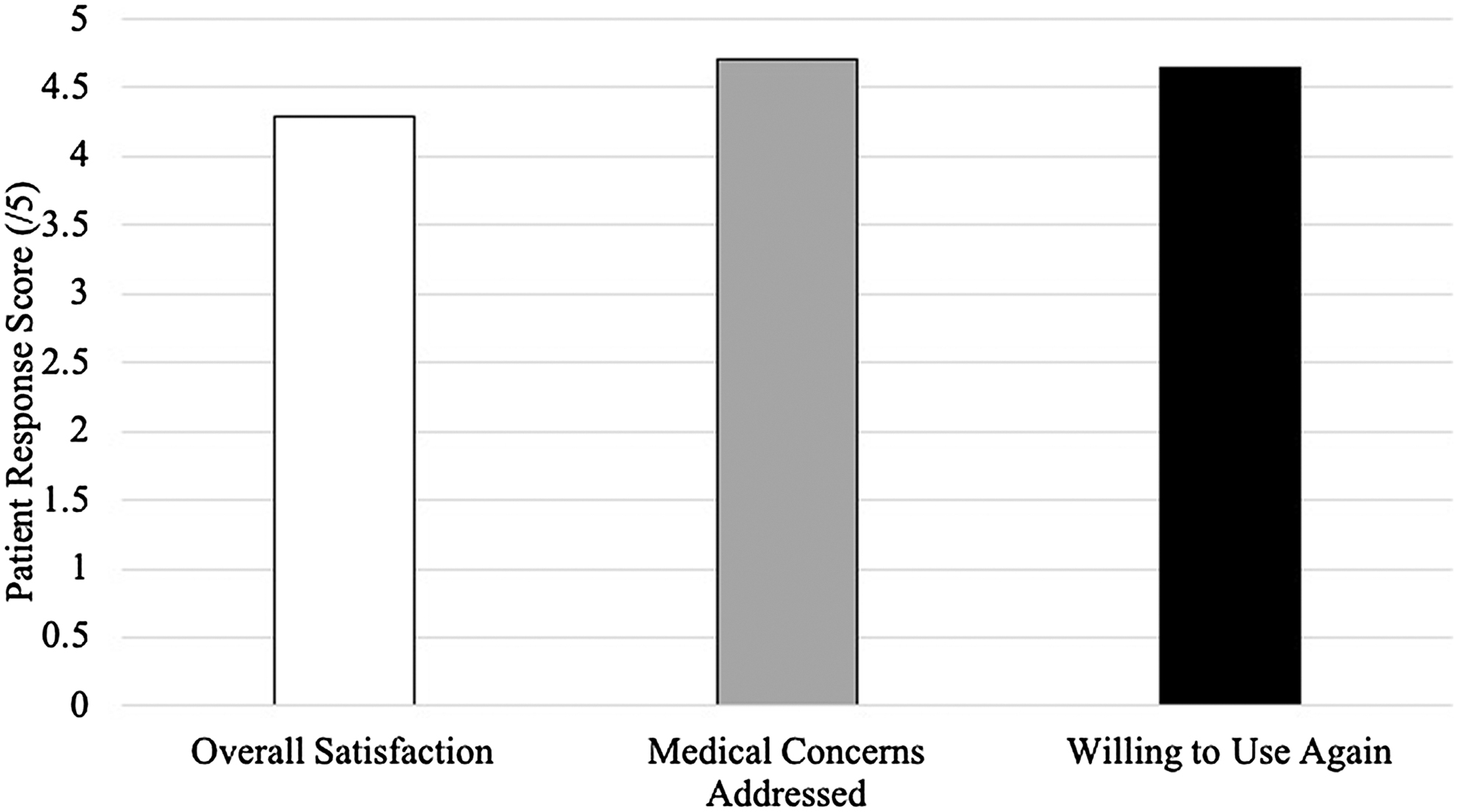
Mean participant satisfaction scores for palliative care FaceTime telehealth consultation.
Participant Satisfaction with Mobile Video Encounter
Discussion
Home consultation by FaceTime and iPad was universally well received with audio and video quality rated as satisfactory across all encounters. Few technical difficulties were experienced, and no consultations were terminated due to poor connection. These findings indicate that palliative care consultation by FaceTime over a cellular network is a feasible means of extending access to services in resource-challenged areas of Nova Scotia and support further exploration on a broader scale.
Successful implementation is known to depend on ensuring nurses buy-in and that technological infrastructure is reliable. 19 Furthermore, there are significant associations between audio/video quality and patient/clinician acceptance and perception of the effectiveness of telehealth encounters. 20 This study involved a palliative care nurse who was fully engaged and comfortable with utilizing FaceTime and facilitating the video interaction between the patient and the palliative care physician. If this project were to be expanded, it would be important to further ensure nurse buy-in with moderating the patient–physician communication using this type of technology.
Reliable connection and the promptness of addressing connection difficulties were found to be paramount to the success of mobile video telehealth services. 21 The LTE-A cellular data network that was used in this study has been shown to be reliable even in remote areas of Nova Scotia. Just as promising is that the LTE-A network covers one of the largest geographical areas in the Maritimes. This indicates the potential for utilizing FaceTime over the LTE-A network in other remote areas of Nova Scotia, and the Maritimes.
Canadian palliative care has been noted to be an inconsistent and inadequate patchwork of services that is in critical need of reform. 22 As calls for improved palliative care grow, we need to embrace service models that optimize use of available technologies. These findings add to the limited body of literature evaluating mobile video technology in home hospice settings, demonstrating that these services can be reliably provided over a cellular data network.
Footnotes
Funding Information
Research in Medicine (RIM) Summer Research Grant, Dalhousie Medical School. Each undergraduate medical student at Dalhousie receives a summer research grant to complete a project.
Author Disclosure Statement
No competing financial interests exist.