
Abstract
Background:
Spirituality is important for many family members of patients in the intensive care unit (ICU). Clinicians without training in spiritual care experience difficulty identifying when family members are experiencing distress of a spiritual nature.
Objective:
The purpose of this study was to develop a guide to help clinicians working in the ICU identify family members who may benefit from specialized spiritual support.
Design:
Cross-sectional study.
Setting/Subjects:
A national sample of spiritual health practitioners, family members, and ICU clinicians.
Subjects:
A panel of 21 spiritual health practitioners participated in a modified Delphi process to achieve consensus on items that suggest spiritual distress among family members of patients in the ICU through three rounds of remote review followed by an in-person conference and a final round of panelist feedback. Feedback on the final set of items was obtained from an end-user group of four family members and six ICU clinicians.
Measurements:
Quantitative data were summarized with descriptive statistics. Content analysis was used to analyze written comments.
Results:
A total of 220 items were iteratively reviewed and rated by panelists. Forty-six items were identified as essential for inclusion and developed into a clinical guide, including an introduction (n = 1), definitions (n = 2), risk factors (n = 10), expressed concerns (n = 12), emotions (n = 7) and behaviors (n = 7) that may suggest spiritual distress, questions to identify spiritual needs (n = 6), and introducing spiritual support (n = 1).
Conclusions:
We have developed an evidence-informed clinical guide that may help clinicians in the ICU identify family members experiencing spiritual distress.
Introduction
Spirituality is important to many critically ill patients and their families.1–3 Current guidelines for family-centered care in the intensive care unit (ICU) recommend offering spiritual support to families of critically ill patients. 4 In ICUs without a dedicated unit spiritual health practitioner or chaplain, other interprofessional team members have the responsibility to identify family members who may benefit from specialized spiritual support. Gaps exist in addressing families' spiritual needs and may be related to a focus on life-saving interventions, as well as clinician lack of awareness, misconceptions, lack of training, and uncertainty around spirituality and associated support.5–7 For example, clinicians may not know how to discuss spiritual needs with family members, have a narrow view of spirituality that is conflated with religion, or assume that families who would like spiritual support will self-refer or have their needs addressed in the community. 8 Furthermore, while clinicians readily identify end-of-life situations as an indication for spiritual care in the ICU, families may wish for spiritual support in other circumstances. 9
Approaches to identifying spiritual distress are well-established within spiritual health practitioner training and the associated literature, yet there has been limited integration within interprofessional education. Specifically, while families frequently report wishing to receive spiritual support from members of the ICU team, there is a notable absence of empirically developed recommendations for identifying the spiritual support needs of families in critical care settings. 7
Assessment of signs and circumstances that suggest a need for spiritual support has been identified as an important skill for clinicians to develop. 10 Instruments to help identify spiritual distress in family members in acute care settings have not previously been reported in the literature. 7 The purpose of this study was to develop a guide to help clinicians working in the ICU identify family members who may benefit from spiritual support.
Materials and Methods
We used a two-phased approach to develop a guide for identifying family members of critically ill patients, who may benefit from spiritual support. The first phase consisted of a modified Delphi consensus process with experts in the field. The second phase involved obtaining feedback from end users. The study was approved by the institutional research ethics board.
Phase 1: Modified Delphi consensus process
Methodology
The Delphi process is an established method of obtaining consensus among experts through a series of anonymous questionnaires, with each round informed by the results of the previous questionnaire. 11 We used three rounds of remote electronic survey, followed by an in-person conference.
Panelist selection
Spiritual health practitioners from across Canada were invited to participate in the consensus process. Information about the study was sent to directors of spiritual care services at 15 Canadian university-affiliated hospitals for distribution to their members. The Canadian Association for Spiritual Care also posted information about the study on their website and sent members an invitation. All spiritual health practitioners with experience working in any ICU setting were eligible to participate. The only exclusion criterion was the inability to commit to participating in all three rounds of electronic survey. We aimed to recruit 15–25 participants for the expert panel.12,13 All participants were oriented to the purpose of the study and their role as panelists through a teleconference.
Survey instrument
Items for the first iteration of the rating instrument were derived from a scoping review of the literature 7 and interviews and focus groups with family members of ICU patients, spiritual health practitioners, and ICU clinicians (nurses, physicians, respiratory therapists, social workers, and indigenous health liaison specialists). 8 The initial rating instrument consisted of four sections: I—Definitions, II—Identifying family members who may be experiencing spiritual distress, III—Guide development, and IV—Demographic information (Supplementary Appendix SA1).
Section I consisted of literature-based definitions of spirituality and spiritual distress, with four items for ranking and a section for free-text comments. Section II contained 113 items grouped into 7 subsections, including risk factors for spiritual distress (n = 18); concerns that family members might mention (n = 22); physical symptoms (n = 7), emotions (n = 22), behaviors (n = 12) and objects (n = 5) that family members might display; and questions that clinicians might ask to identify spiritual distress in family members (n = 27). The items in these subsections were presented across a 7-point Likert scale for rating degree of importance in identifying spiritual distress (one not at all important and seven extremely important), as well as a section for free-text comments and suggestions for additional items of significance. Section III contained a free-text box for recommended considerations in developing the guide. Section IV consisted of demographic questions. The rating instrument was entered into a secure electronic survey platform (SurveyMonkey, Palo Alto, CA) to facilitate distribution and data collection.
Consensus process
Three rounds of remote electronic surveys were conducted between February and June 2018, followed by an in-person consensus conference. Panelists were sent a link to the rating instrument by email and given two weeks to respond. A reminder was sent to those who had not completed the survey by the end of the two-week period.
The rating instrument was iteratively modified after each round of the survey; Likert scale items for which consensus had not been achieved were included in subsequent rounds of the survey and items for which consensus had been achieved for either inclusion or exclusion were omitted from subsequent rounds. Responses to open-ended questions were used to modify existing survey items and generate new items; open-ended questions were not included in the third round. For the second and third rounds of the survey, participants were also provided with anonymized data on which items had achieved consensus for inclusion and exclusion, as well as a summary of responses to open-ended questions.
All panelists were invited to a full day in-person consensus conference facilitated by two experienced qualitative researchers (A.L.R. and S.S.), which took place on June 18th 2018 in Calgary, Alberta, Canada. The in-person conference was audio-recorded and memos were recorded by A.R., K.G.M., and S.S. The meeting began by reminding panelists of the goal—to reach consensus on a parsimonious set of items that would fulfill the purpose of the clinical guide, the purpose being to help clinicians without specialized training in spiritual care identify family members of ICU patients, who might benefit from spiritual support. This was followed by a discussion of how the guide would be used in the clinical setting and deliberation on and refinement of the definitions of spirituality and spiritual distress.
Each item for which consensus had been achieved in the three rounds of electronic survey (n = 120) was then reviewed and consensus decisions on item inclusion and exclusion were made through round table discussion on whether the item aligned with the purpose of the guide and established definitions of spirituality and spiritual distress. Items for which consensus had not been achieved by the end of the third round of electronic survey (n = 31) were also reviewed. The decisions made during the in-person conference were integrated into the definitions and items for identifying family members who might benefit from spiritual support; instructions for clinicians and free-text boxes for recording clinical observations were also added. This version of the clinical guide was distributed electronically to all panelists for a final round of review. Panelists were instructed to provide written comments on the content, language, and sequence of items.
Data analysis
Ratings of survey elements
After each round of electronic survey, panelist Likert scale ratings were summarized using means and standard deviations. Excel software was used for statistical analysis. Consensus was defined as a mean score of one to two for exclusion (“not important to include in the guide”) and six to seven for inclusion (“essential to include in the guide”). Consensus was considered to not have been achieved if the mean score was three to five (“may be important to include in the guide”).
Written comments from surveys
Panelists' written comments from the three rounds of electronic survey were analyzed in two ways following each round of the survey. First, individual comments within each section were either used to modify the original item or developed into a new item; modified items and new items were included in the subsequent round of survey. 14 Second, thematic content analysis 15 was used to analyze the written comments. K.G.M. applied open coding and constant comparison techniques to generate codes and identify themes. The codes and themes were reviewed by A.R. and discrepancies resolved through discussion; the themes were provided to panelists in the subsequent round of survey. Atlas.ti version 10 software was used for qualitative data management.
In-person conference and feedback on clinical guide
Memos from the in-person conference, supplemented by verbatim quotes from the audio recording, were summarized and used to develop the content of the initial draft of the clinical guide. Each of the comments that panelists provided as feedback on this guide was considered separately and revisions made to generate the final draft.
Phase 2: End-user feedback
Participant selection
A national sample of family members of former ICU patients and ICU clinicians identified through purposive and snowball sampling were invited to provide feedback on the draft of the clinical guide. Spiritual health practitioners who had participated in the Delphi process made recommendations for clinician participants. Clinician participants recommended family members of ICU patients who had participated as family representatives in other ICU initiatives.
Data collection
An electronic copy of the final draft of the clinical guide was circulated to participants for feedback. Participants were asked to provide written comments on the content, language, sequence of items, and feasibility of use in the clinical setting.
Data analysis
Each of the comments provided by the family members and clinicians was addressed separately by one of the researchers (A.R.). The feedback was either integrated into the guide or further discussed with the respondent and other research team members to come to a decision on whether or not to incorporate into the guide.
Results
Participant characteristics
Thirty spiritual health practitioners expressed interest in participating in the Delphi consensus process. After the introductory teleconference, 21 consented to participate as panelists. All panelists completed all three rounds of electronic survey. Fourteen panelists attended the consensus conference in person, and three attended by teleconference. Nine panelists provided feedback on the initial draft of the clinical guide. The end-user participants who provided feedback on the clinical guide consisted of six interprofessional ICU clinicians and four family members of previous ICU patients. Participant characteristics are described in Table 1.
Demographic Information
One participant did not respond, n = 20.
Consensus conference participants.
One participant did not respond, n = 5.
ICU, intensive care unit.
Item ranking and modification
After the first round of the survey, 78 of the 118 items achieved consensus for inclusion and five achieved consensus for exclusion (Fig. 1). Consensus was not reached for 35 items, and based on free-text comments, 10 of these items were modified and 26 new items were added, resulting in a total of 61 items for the second round of survey. After the third round of survey, consensus had been achieved to include 120 items and exclude 5 items, and consensus had not been achieved for 31 items. All items that had achieved consensus for inclusion or for which consensus had not been achieved (n = 151) were reviewed during the in-person conference. At the end of the conference, 46 items had achieved consensus for inclusion with modifications, and consensus was achieved to exclude the remaining 105 items. Details of item selection are described in Supplementary Appendix SA2.
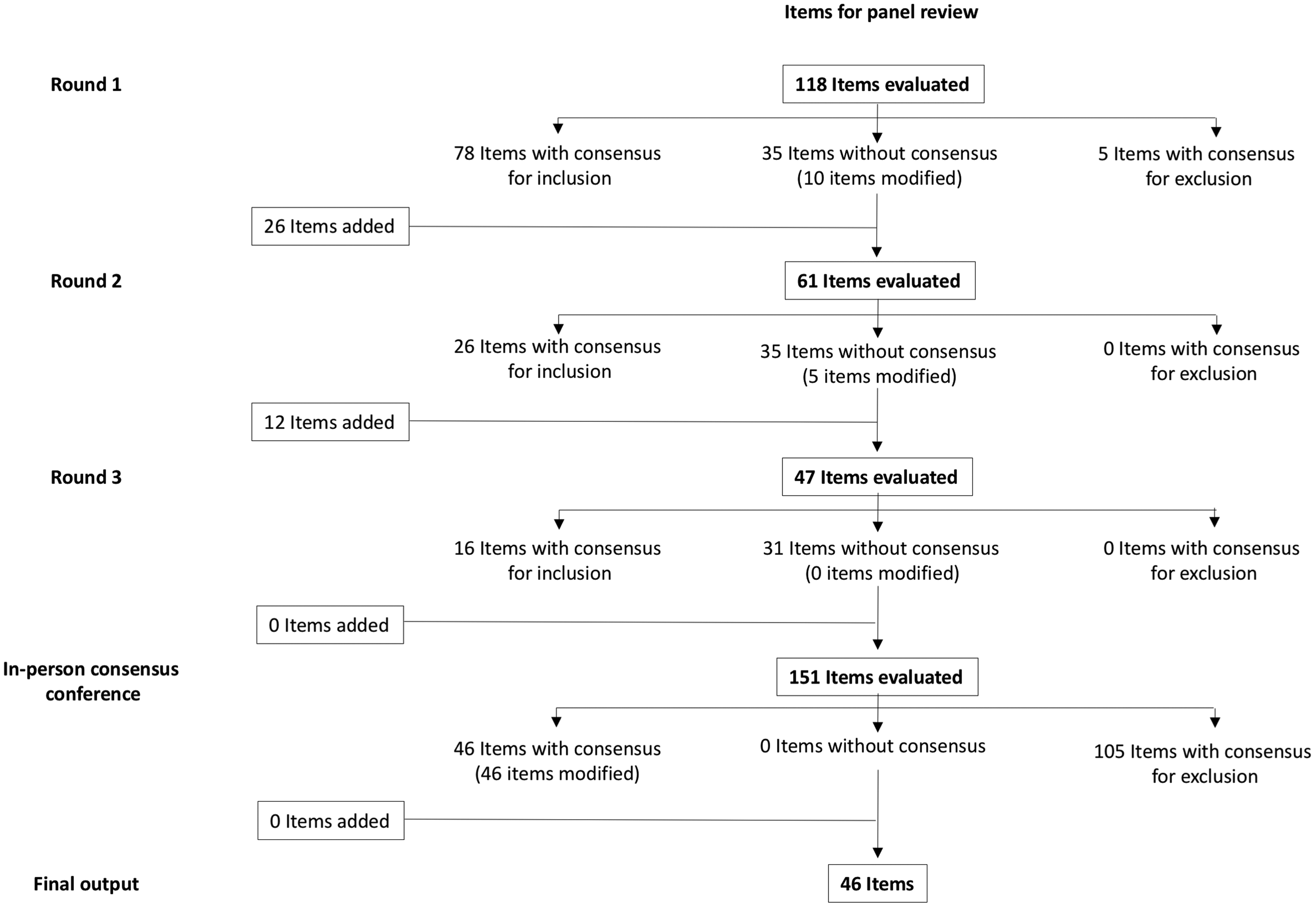
Flow diagram of item selection through a modified Delphi consensus process.
Qualitative evaluation
Written feedback provided by panelists and end users included comments on content and formatting to enhance the clarity and clinical utility of the guide, process of future implementation, and support for the guide (Supplementary Appendix SA3).
Feedback related to content included suggestions for clarifying concepts and terms and modifying language to improve sensitivity and reduce complexity. Many panelists recommended additions within each section of the guide. Feedback on formatting related to the sequencing of items and recommendations for graphic design. Comments on the process of implementing the guide included concerns that certain questions may be uncomfortable or cause distress, and the importance of adapting questions to the clinical context and taking context into consideration when interpreting responses. Several panelists recommended that certain candidate questions were more appropriately asked by those with specialized training in spiritual care. Skillful communication was highlighted as foundational when applying the guide in clinical settings. Finally, support for the guide consisted of comments that supported the concept and content of the guide, and anticipated a positive impact on family members and clinicians. The final list of items from the consensus process is presented in Table 2.
Final Set of Items Developed Through Delphi Consensus Process and End-User Feedback
Clinical guide
The clinical guide for identifying spiritual distress in family members of ICU patients developed from triangulation and integration of the results from the modified Delphi consensus process and end-user feedback consisted of the following five sections: Introduction, Orientation to key terms, Clinical observations that can indicate spiritual distress, Questions to identify sources of spiritual strength and support needs, and Recommendations for introducing spiritual support (Supplementary Appendix SA4).
Discussion
We have developed an evidence-informed practical guide for clinicians working in the ICU to help them identify family members who may benefit from spiritual support. To our knowledge, empirically developed guides of this nature have not previously been published in the literature. The guide we have developed mirrors a typical clinical approach, beginning with initial observations and followed by specific questions. It includes definitions of key concepts, a description of clinical observations and examples of clinical questions that can be helpful in identifying family members who may benefit from spiritual support, and suggested phrasing for introducing spiritual health practitioners.
The guide is intended as a guide for clinicians without specialized training in spiritual care to facilitate clinical assessment and meaningful conversations around spirituality in a sensitive manner, which can then be continued and further explored as needed by practitioners specialized in spiritual care. We emphasize that the guide should not be used as a checklist or a script, but rather as a conversation guide. Clinicians can apply the sections of the guide that resonate with them and adapt other sections as needed to align with their established clinical practice and family members' needs.
Spirituality and spiritual distress are terms that have a myriad of meanings for patients, family members, and clinicians.16–19 This study makes an important contribution to existing literature by establishing definitions that are conceptually aligned with the expert experiences of spiritual health practitioners and that resonate with both clinicians and family members. While terminology and the clinical guide were developed through a rigorous process of consensus, we acknowledge that spirituality is individually and culturally defined. Hence, we caution clinicians against a “one-size fits all approach,” 20 and other definitions exist in the literature.21–23
Our operational definition is not intended to be universal and was established for the specific purpose of developing our guide, to ensure conceptual clarity and agreement between participants on what was being discussed. The definitions of key concepts served as the lens through which the remainder of the guide was developed. Suggestions and disagreements that arose during the consensus and subsequent feedback processes around items to include in the guide were screened and resolved, respectively, by filtering them through the agreed upon definitions. Therefore, we believe that these definitions will facilitate a common understanding and a shared clinical lexicon among clinicians who adopt our guide in clinical practice settings.
The observations described in the guide may help identify family members experiencing spiritual distress; however, there are many types of distress, such as psychological (cognitive, behavioral, and emotional), social, spiritual, and moral. 24 These different types of distress can have similar external manifestations 25 and multiple types of distress may be present at any given time and be intertwined and inseparable.26,27 We caution that relying on observations alone can lead to misinterpretations based on automatic judgments and false assumptions. The observations we outline are intended to be a starting point for clinicians to initiate conversations that explore family members' experiences more fully and identify how they would like to be supported. Identifying a spiritual element to the distress has implications for the types of support that may best meet their needs.
While the observations described herein help identify family members experiencing spiritual distress, individuals who are not experiencing spiritual distress may also benefit from spiritual support. 9 The clinical questions are intended to help identify this additional group of family members who may feel better supported when spiritual care is incorporated into the care offered in the ICU. Spiritual support can involve religion-specific activities such as prayer, spiritual-focused conversations around meaning and purpose, counseling interventions to facilitate reflection, hope and reconciliation, emotional support through empathy and comfort, or advocacy around ways to meet patients' and their families' needs. 28
Given the sensitivity around spirituality and spiritual distress, 17 our guide pays particular attention to the nuances of language in the description of key concepts, the wording of the clinical questions and the phrasing of how spiritual care can be introduced. The questions included were informed by our rigorous consensus process and chosen carefully, to avoid questions that clinicians without specialized training in spiritual care may not feel comfortable asking and that could elicit answers to which they may not know how to respond or are beyond their scopes of practice.
The clinical guide has limitations. It was developed based on the expert opinion and experiences of Canadian spiritual health practitioners and may not reflect notions of spirituality and spiritual distress in other cultures. Feedback on the guide was obtained from only a small sample of clinicians and family members, whose views may not represent those of the larger population. Finally, the guide has not been applied or validated within the clinical setting, including among diverse patient populations or practice settings. Next steps will be to implement the guide within the ICU context and evaluate its reliability and validity in identifying family members who may benefit from spiritual support.
Conclusions
We have developed an evidence-informed practical clinical guide to help clinicians working in critical care settings identify family members of patients in the ICU, who may benefit from spiritual support. The purpose of this guide is to empower ICU clinicians to identify and initiate these important conversations in a sensitive and compassionate manner. Future research will be needed to determine how the guide can best be integrated within the clinical setting, its practical application, and its impact on clinicians and the families they support.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.