
Abstract
Abstract
Many of America's Veterans have unique medical and psychosocial needs related to their military service. Since most medical care received by Veterans occurs outside of the Department of Veterans Affairs (VA) health care system, it is imperative that all medical providers have a working understanding of the unique needs of Veterans and some of the many programs and services available to Veterans through the VA. This article, created by an interdisciplinary team of palliative care and hospice providers who care for Veterans throughout the country, seeks to improve the comfort with which non-VA clinicians care for Veterans while increasing knowledge about programs for which Veterans might qualify through the VA.
Introduction
One in four Americans who dies in the United States today is an American Military Veteran. 1 It is surprising to some clinicians that the majority of Veterans do not receive care at a Department of Veterans Affairs (VA) Medical Center but are cared for in clinics and hospitals all over the country. Given the aging Veteran population nationally, the VA has been committed to providing high-quality palliative care (PC) for Veterans for 20 years and has created a multitude of new programs that seek to improve care for Veterans with serious illness or who are at end of life (EOL). 2 Many non-VA employed medical providers are unaware of these programs and other benefits that Veterans have earned through their military service. Many clinicians also feel uncomfortable evaluating for military-related causes of existential or psychosocial suffering at EOL. 3
Given the need for all medical providers to provide exceptional care to Veterans, we have assembled a team of hospice and PC providers from VA facilities across the country to address commonly identified knowledge gaps around caring for our Veterans with serious illnesses or who are at EOL. We hope to show the ways in which many more Veterans could be getting care that is tailored to their individual needs.
Tip 1: There Are Four Major VA Strategies to Improve Care for Seriously Ill Veterans, Especially for Those at EOL
These actions and programs have focused on caring for Veterans with serious illnesses with which every clinician should be familiar.
The first program was the VA Comprehensive End-of-Life Care Initiative (CELCI; 2009–2012). The CELCI addressed four domains: (1) increasing reliable access to palliative and hospice care; (2) building a national network of skilled clinician leaders to enhance care delivered to seriously ill Veterans by specialists and nonspecialists; (3) collaborating with community partners to improve the care of terminally ill Veterans outside VA, and (4) establishing an infrastructure for using performance measures to improve care delivery. As a result of these efforts, in 2018 there were over 90 hospice/PC units across 146 VA facilities and PC teams at every VA medical center. More Veterans now choose to die in designated VA hospice beds than in acute and intensive care beds combined. Eighty percent of Veterans who die in inpatient VA facilities (which include acute care units in hospitals, hospice/PC units, and VA-owned and operated nursing homes) have received at least one VA-based PC consult. 4
Second, by law, VA must offer to provide or purchase hospice care for every enrolled Veteran that a VA physician has determined is appropriate for hospice. This care could include palliative or hospice care at a VA facility or home hospice care delivered by a community hospice agency (since the VA does not directly provide home hospice care). Veterans eligible for Medicare may use their Medicare Hospice Benefit but for those without Medicare or who choose VA-funded hospice care, VA funding is available. 5
A third strategy to improve EOL care for Veterans is housed at the Veteran Experience Center (VEC). Since 2010, the VA has actively solicited feedback about care in the last month of life for all Veterans dying in inpatient VA facilities. This population-based quality improvement program includes the Bereaved Family Survey and examines Veteran, family, and health care system factors that affect Veteran and family experiences of care. Results are used to identify areas in need of improvement at the facility level and provide clinician education, regional quality improvement initiatives, and a comprehensive clearinghouse of best practices. 6
A final example of the VA's commitment to delivering care that aligns with Veterans' goals, values, and preferences was launched in 2017. The Life-Sustaining Treatment Decisions Initiative (LSTDI) both requires VA practitioners to initiate proactive goals of care conversations (GoCCs) with seriously ill Veterans and to document the content of the conversation. The template used to document the conversation launches life-sustaining treatment (LST) orders that are durable across all care settings. The LST note template and order set are one component of a multipronged strategy that also includes staff training to enhance proficiency in conducting and documenting GoCCs and monitoring and information technology tools to support implementation and quality improvement. The LSTDI program was launched nationally in 2017 after a multifacility demonstration project. This project tested and refined LSTDI processes and tools and identified strong implementation practices for system-wide dissemination. 7
Tip 2: VA Health Care System Is the Largest Integrated Health Care System in the United States and Offers Programs and Benefits Beyond Most Civilian Systems
The Veterans Health Care system (VHA) is the largest integrated health care system in the United States. 8 Current estimates are that there are more than 19 million Veterans living in the United States. In fiscal year 2016, ∼50% of all Veterans used at least one VA benefit. This equates to more than 9 million Veterans who sought care at VA hospitals and clinics. 9
In addition to basic primary care, specialty care, and hospital services, the VA offers many other programs that may not be available in typical health care systems. Programs such as Aid and Attendance can assist with payment for additional caregiving services when Veterans and families are in need. Other programs include Home-Based Primary Care, which delivers primary care services to eligible Veterans in their own homes. 10 Telehealth can bring primary care services to those in rural areas or who have difficulty traveling to their local VA clinic due to mobility issues.
Mental health services include inpatient and outpatient counseling and psychiatric services. Many VA clinics can provide these services through the Telehealth program. Recently, VA has increased programming in suicide prevention. Additionally, confidential services are available through the Veterans Crisis Line. 11
Figure 1 shows that, while the number of living Veterans has been steadily decreasing, the utilization of health care services by Veterans within the VA Health Care System has been increasing. 12 As this trend is expected to continue, VHA is constantly expanding these and other programs to accommodate the growing need.
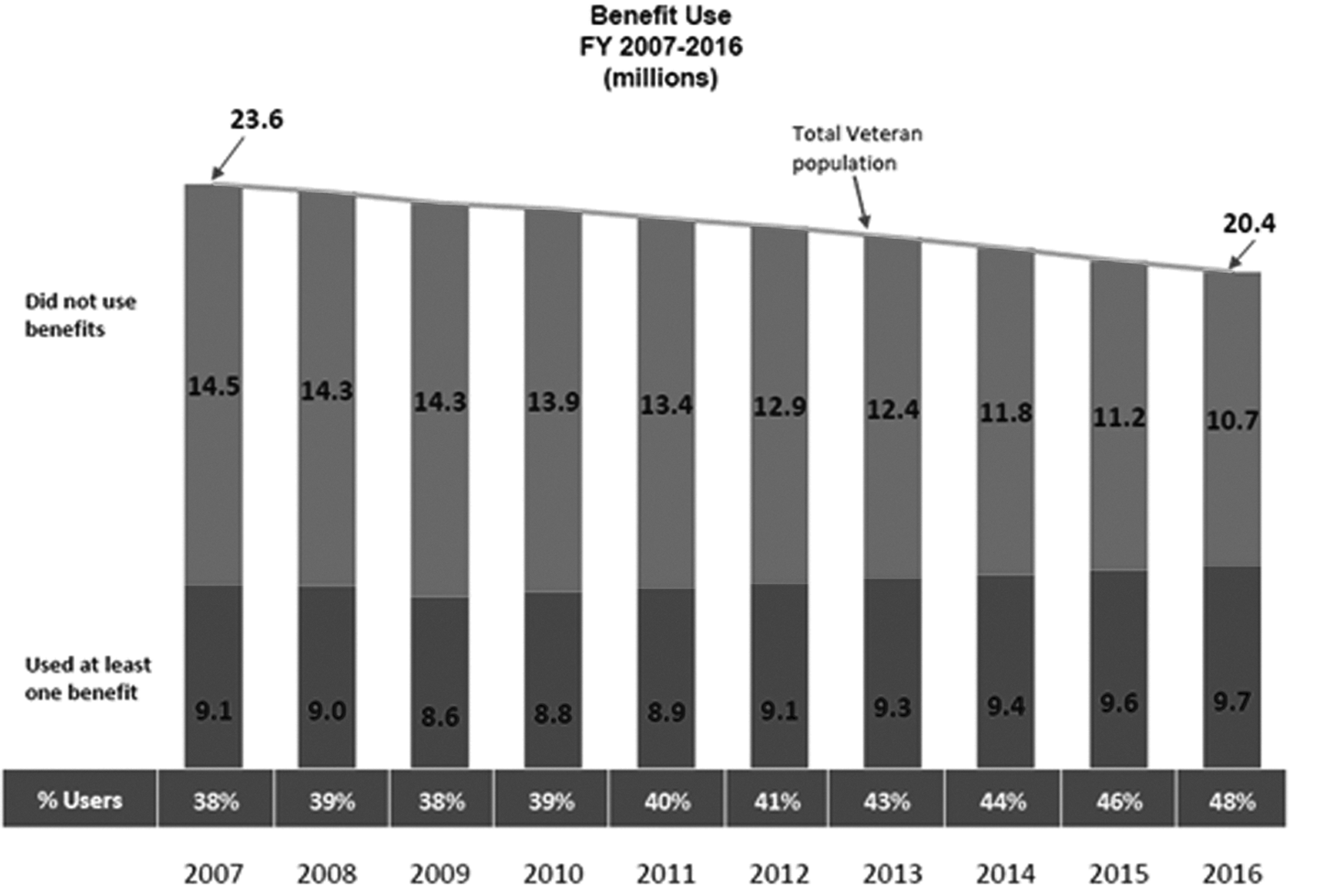
The number of Veterans using VA benefits increased slightly in recent years despite a 13% decline in the total Veteran population since 2007. Source: U.S. Veterans Eligibility Trends and Statistics, 2016 prepared by the National Center for Veterans Analysis and Statistics. VA, Veterans Affairs.
Tip 3: VA Policy Allows for Concurrent Care Including PC and Hospice
In 2003, VA Directive 2003–008 mandated the formation of PC Consultation Teams at every VA Medical Center. 13 This Directive allowed for Hospice and PC services to be offered to Veterans on equal standing with any other medical service and these services should be provided in inpatient and outpatient settings. The Directive also required Medical Centers to offer to provide or purchase hospice care either in an inpatient setting or in the Veteran's home setting. Veterans can also receive comprehensive hospice care within Community Living Centers (CLC) and other designated areas within VA Medical Centers.
Most VA Medical Centers have an Inpatient Hospice Unit. These units are usually housed in a CLC that is affiliated with the Medical Center. Unlike traditional Medicare hospice inpatient units, these units do not require Veterans to have unmanaged symptoms to be eligible for admission. Each Inpatient Hospice Unit allows Veterans nearing the end of their lives to stay for a period of time based on the Veteran's needs. Unlike access to VA nursing home services for long-term care, hospice units are available to every VA-enrolled Veteran whether or not they have service-connected conditions. 14
The CELC Initiative, in addition to the innovations described in section 1, added to the hospice benefit for Veterans by allowing for concurrent PC. Concurrent PC gives Veterans the ability to receive disease-focused medical interventions given with palliative intent while also receiving hospice care if their prognosis is six months or less. As a result of the CELC Initiative, hospice use increased during the time of the initiative as did the provision of concurrent PC. 15
Despite these innovations, there are still significant barriers to Veterans' ability to receive hospice services, particularly in the concurrent PC model. In addition to the usual barriers to hospice care, such as the perception that hospice means “giving up,” hospice agencies or Medicare Administrative Contractors may perceive impediments to an enrolled Veteran receiving treatments for their terminal condition beyond what the hospice agency is able to provide, even when these VA services supplement and do not duplicate what the hospice agency is providing.
Tip 4: Only by Asking Will You Reliably Know if Your Patient Is a Veteran and Eligible for Enrollment at VA
It is important to know if your patients are Veterans. As part of any consultation or admission, asking all patients about their military service is crucial. The military history checklist is one of many useful tools that can be found at the We Honor Veterans (WHV) website. 16
If your patient is a Veteran but not enrolled at a VA Medical Center, they can enroll using their discharge paperwork (DD-214) online, in person, by phone, or by mail. 17 To access VA health care programs, Veterans must have served in the active military, naval, or air service, have separated under any conditions other than dishonorable and, for Veterans who enlisted after late 1980, must have served 24 continuous months or the full period for which they were called to active duty. 17
Many Veterans are not enrolled at a VA Medical Center, or are enrolled but choose to receive the majority of their medical care elsewhere. There are many reasons for this, including: the Veteran has health insurance elsewhere; wants “someone who needs it more” to get VA-provided care; or simply do not wish to go to a VA facility. Fortunately, for those who qualify for VA care, hospice and PC services are available.
Tip 5: The Experience of Each Veteran Is Unique
Veterans receiving care through VA are generally sicker than the population in general. 18 The era in which a Veteran served, their role in the military, whether they enlisted or were drafted, their exposures to events or toxins, their injuries, and their current medical condition are all factors in who the Veteran is. For example, the Veterans who returned from World War II were celebrated while the Veterans who returned from Vietnam were often reviled. The deployment experience of Veterans has changed. For instance, WWI, WWII, and Korean Conflict Veterans left home and sometimes did not return for years while those in the Vietnam Era and later were more likely to return home periodically and this continues in present-day deployments. Given this variation, it is impossible to generalize the experience of a Veteran and only by asking a Veteran can a medical provider understand the lasting impacts of military service to Veterans.
Tip 6: Veterans May Have Medical Conditions Based on Their Military Experience and Disabilities Connected to Military Service Can Be Compensated
The Veteran experience may also include exposures and injuries that are unique to their time in the service. Hazardous chemicals and materials, such as herbicides like Agent Orange, asbestos, radiation, burn pits, mustard gas, contaminated drinking water at Camp Lejeune, and service during Gulf War, are some examples. These exposures can lead to specific disease states. For instance, exposure to Agent Orange has been linked to multiple conditions, including cancers (chronic B cell leukemia, Hodgkin's disease, multiple myeloma, prostate cancer, soft tissue sarcoma, and respiratory cancers), type 2 diabetes, ischemic heart disease, Parkinson's disease, peripheral neuropathy, porphyria cutanea tarda, and others. 19
Also, the incidence of some diseases is higher in the Veteran population. Some, like Amyotrophic Lateral Sclerosis occur in the Veteran population about 1.3–1.5 times the rate of the non-Veteran population. The mechanism for this has not yet been discovered. 20 Others, like liver disease, including cirrhosis, hepatitis C, and hepatocellular carcinoma, and head and neck cancers not resulting from human papilloma virus, occur more frequently in Veterans than in non-Veterans. 21
Given that some illnesses are more common in Veteran populations, there are many benefits available to Veterans in addition to medical care. Some of these benefits are particularly important in EOL care situations: service connection disability compensation, survivor benefits, and burial benefits.
Service connection describes an injury or a physical and a mental health condition resulting in disability that is linked to the military service. The Veteran can receive monthly tax-free compensation based on the degree of disability. 22
Survivors or dependents of Veterans may also be eligible to benefits, including education assistance, home loan guaranties, health care insurance, survivors' pensions and VA Dependency and Indemnity Compensation (DIC). The spouse or a child of a Veteran are eligible for DIC if the Veteran died from a service-related injury or illness. A surviving spouse may also be eligible for a monthly pension if their yearly family income meet certain limits set by Congress. 23 Given the benefits available to families of those who die from service-related injuries or illnesses, special care must be taken when completing the death certificate of a Veteran to ensure service-connected, contributing mental and physical illnesses are listed in the appropriate location on the death certificate.
Tip 7: Veterans Differ Socioeconomically from the General Population and Have Significantly Different Mental Health Needs, which May Affect EOL Care and Increase Suicide Risk
The United States Department of Defense estimates that there will be an average of 200,000 new Veterans each year 24 although deaths of Veterans from the World War II and Vietnam eras will lead to an overall decrease in the number of US Veterans by 19% from 2014 to 2024. 25 On average, Veterans have had a lower mortality rate than the general public (referred to as the “healthy soldier effect”), although this effect has, unfortunately, reversed for Veterans from recent conflicts. 26 Nearly half of Veterans are over age 65. Among Veterans in the labor force, unemployment rates are lower than for non-Veteran civilians, although Veterans covered by VA health care are unemployed at rates 50% higher than the general Veteran population and 20% higher than the civilian population. 25
Mental health disorders are more prevalent in Veterans than in civilians. 27 Suicide is also significantly more common in Veteran populations. Male sex, depression, manic-depressive disorder, heavy or binge drinking, and alcohol-related problems are all associated with increased risks of suicide in a mixed active duty and Veteran population. Perhaps surprisingly, there is no significant association between deployment and suicide. 28 Barriers to VA-provided care include stigma around mental illness, distance from and complexity of the VA system, and variable confidence in the VA system can lead Veterans to seek medical care privately, 29 so all health care providers should vigilantly assess suicide risk in their patients who are Veterans.
Tip 8: Post-Traumatic Stress Disorder, Military Sexual Trauma, and Moral Injury All May Have an Effect on the Health and Dying Process of a Veteran: There Are VA Resources Accessible throughout the Trajectory of Illness
Post-traumatic stress disorder
Post-traumatic stress disorder (PTSD) is characterized by a traumatic event where actual or threatened death or physical harm was experienced or witnessed. Symptoms include: (1) recurrent, intrusive thoughts, nightmares, or flashbacks; (2) avoidance of activities and places that may trigger memories of the trauma; and (3) increased arousal (sleep difficulty, irritability, hypervigilance). PTSD can emerge at any point after the trauma, including later in life. About 30% of Vietnam Veterans have had PTSD in their lifetime. In a given year, 11–20% who served in OIF or OEF and 12% who served in the Gulf War have PTSD, with overall PTSD rates in Veteran populations ranging from 11% to 79%. 30
Military sexual trauma
Military sexual trauma (MST) is any sexual harassment or assault while a person is in the military. MST is more likely to result in PTSD than most types of trauma, including combat. MST is more common in women Veterans, but because there are many more male Veterans, over half of all Veterans with MST are men. Treatment for mental and physical health conditions related to MST is free. Veterans do not need to be service connected, to have reported the incident(s) at the time, or to have other documentation that MST occurred to receive free MST-related care. 31
Moral injury
Moral injury is a cluster of symptoms, such as shame and guilt that result from experiences which violate a person's core values and principles. In the setting of war, this may result from direct or indirect participation in acts of combat, witnessing death or dying, or giving or receiving orders that are perceived as morally transgressive. 32
Effect on health and dying process of a Veteran
Veterans with PTSD and moral injury commonly have increased symptom burden as they near EOL. The threat to life inherent in terminal illness may mimic the original trauma and this may amplify PTSD and lead to significant distress. These Veterans may have difficulty engaging in life review, as this review may be in conflict with their long practice of avoidance of past events. Also, these Veterans may have a limited social support system and limited trust of systems for similar reasons. 33
Tip 9 : Death, Dying, and Funerals Are Different for Veterans and Their Families
Veterans have a strong sense of personal identity grounded in their military service. 34 Some Veterans may enjoy talking about their military experiences and the foreign countries where they served, but not all Veterans discuss their service freely. Some Veterans who saw combat are hesitant to share their experiences. In basic training, new members of the military learn to suppress emotions and to focus on the mission at hand. So, allowing emotions to surface can be an unfamiliar experience. Complicating this task of opening up, some Veterans feel their personal beliefs in God and honor directly conflict with their actions during combat and this can cause guilt and shame. 35
Elevated anticipatory grief has been found in families that had relational dependency, lower education, and poor grief-specific support, while also experiencing discomfort with closeness and intimacy, spiritual crisis, and an inability to make sense of the loss. Anticipatory grief can be marked by anger, excessive worrying, spiritual distress, and struggling with a loved one's looming death. 36
Since the United States moved to a volunteer military after the Vietnam War, the concentration of service members with a history of Adverse Childhood Experiences (ACEs) has increased. Some of these individuals may have enlisted to escape personal problems, like household dysfunction or abuse. 37 With a higher concentration of ACEs, more and more Veterans may find their social support to be lacking or find that relationships may be severed as they near the EOL.
Veterans with an-other-than-dishonorable discharge, as well as their spouses and dependent children, may be eligible for VA burial and memorial benefits. Benefits include burial in a VA National Cemetery, a headstone or marker for a private cemetery, and burial flags. 38 Some Veterans' families may be entitled to a burial allowance to help cover funeral and burial cost. There is reimbursement for service connected deaths. There may also be some reimbursement for non-service connected deaths. 39
Tip 10: WHV Is a Comprehensive Partnership between the National Hospice and PC Organization and the VA that Seeks to Improve Care that Veterans Receive from Community Health Care and Hospice Agencies
WHV is a program of the National Hospice and PC Organization (NHPCO) in collaboration with the VA. This is a pioneering program that teaches community providers, such as hospice agencies, home health agencies, skilled nursing facilities, and assisted living programs, to recognize the unique needs of America's Veterans and their families. In partnership with VA staff, these community partners learn how to best serve the Veterans in their care. 16
WHV provides educational tools and resources. It also provides tiered recognition to organizations, known as Partners, that demonstrate a systematic commitment to improving care for Veterans. Resources and tools are provided at no cost to community organizations, including hospice agencies.
Several programs have evolved from and now supplement the WHV (www.WeHonorVeterans.org). These include the Hospice–Veteran Partnership (HVP), the Veteran Community Partnership (VCP), Veteran to Veteran Partnership, and the No Veteran Dies Alone (NVDA) program.
Conclusion
Caring for America's Veterans is important. To be certain, those who have served our country often have medical and psychosocial needs different from their civilian countrymen. The VA has made incredible strides over the last two decades to improve the quality of care for Veterans throughout their life. From inpatient and outpatient PC teams to hospice care provided to Veterans to programs like Aid and Attendance and WHV, the VA has created a comprehensive safety net for Veterans with serious illnesses or who are at or near EOL.
Since most health care for Veterans is provided outside of the VA system, all health care providers must be comfortable caring for the needs of Veterans. Screening all patients for military service, taking a careful military history, and anticipating the effects of military service on a Veteran's trajectory through a serious illness are primary skills that all PC providers should possess. It is only through careful, deliberate practice that all health care providers will identify Veterans' needs and also provide the comfort, dignity, and peace to the deserving who gave so much to protect our country.
Footnotes
Author Disclosure Statement
No competing financial interests exist.