
Abstract

Dear Editor:
In 2013, we described the concept of a house as a visual framework for goals of care conversations. 1 In the intervening years, there have been reports of this model being used at various educational institutes, providing specialty and generalist palliative care, and complex conversation training. When the model was first introduced it had four components, a foundation, two uprights and a roof, each representing an aspect of the goals of care conversation.
It became apparent that the framework was missing one critical element, that of a cross beam capping the patient and medical story uprights (Fig. 1). What follows is a brief outline of each of the five elements of this updated visual model for goals of care conversations.
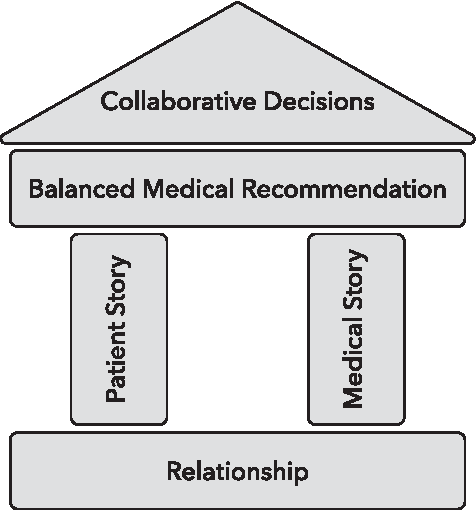
Framework for goals of care conversations.
The foundation represents relationship, encompassing the importance of establishing trust, respect, and competency. This is where we align our intention and ask for permission to begin the conversation.
The left upright represents building the patient story, asking before telling. To gather the emotional and cognitive data needed to elicit patient preferences and eventually make a recommendation, we suggest three practical relevant time-efficient types of questions. The first pertains to how the illness is affecting their ability to do what brings joy and meaning to life. The second is what they know about their current illness and the third is where they find strength and support day to day.
The second upright is our story or in other words, the medical story. When we have identified a patient, who might benefit from a goals of care conversation, there is likely some concern about prognosis. Disclosing medical information in the goals of care conversation often requires delivering some aspect of serious news, than responding to emotion. It may be that a higher level of care is needed or that current treatments may be starting to outweigh anticipated benefits. Whatever the serious news, it is an opportunity to align intention, share our concerns, and determine patient priorities considering the medical realities.
The capping beam in the updated model represents the task of making a balanced recommendation, part of our professional responsibility. When we incorporate both the patient preferences and medical realities into our recommendation, we avoid driving the patient toward uninformed autonomy with a smorgasbord of options, on the one hand, or being paternalistic, on the other.
The final component of the house model is the roof, representing collaborative decision making. This includes next steps if there is consensus to accept specific recommendations. If the patient or family does not accept our recommendations, it gives us an opportunity to collaborate on how to respectfully continue supporting them in their ongoing care.
When we have a solid understandable learnable framework for the goals of care conversation, we can focus on the integrity of the process, letting go of the outcome. These are not win or lose conversations but rather an opportunity to build climates of healing for our patients and for ourselves.