
Abstract
Background:
Studies show significant associations between the various dimensions of religiousness and end-of-life (EOL) decisions, such as individuals with high religiosity are more likely to choose aggressive care at EOL. However, these studies focused largely on smaller cancer populations. To our knowledge, there is no existing literature about the association between religiosity and EOL decisions within a national sample of older adults.
Objective:
The objective of this study was to investigate the association between religiosity and advance directive (AD) completion, and among those with an AD, documented EOL care preferences, using a nationally representative sample.
Methods:
This was an observational study. Descriptive statistics and logistic regression were conducted with 6051 decedents from the Health and Retirement Study using self-reported frequency of religious service attendance, importance of religion, and religious affiliation.
Measurements:
The dependent variables were AD completion and care preference. The independent variables were self-reported frequency of religious service attendance, importance of religion, and religious affiliation.
Results:
Protestants and Catholics had significantly lower odds of AD completion, compared with those with no religious preferences. Decedents who reported religion as very important had significantly lower odds of AD completion than decedents who said religion is not too important. Furthermore, decedents who attended religious services at least once a week, compared with those who do not attend, had significantly higher odds of completing an AD. Among those who completed an AD, neither religiosity nor religious affiliation was significantly associated with preference for prolonged care.
Conclusions:
Our study demonstrates the influence religiosity has on the development of ADs, prompting seriously ill patients' religious needs to be recognized and supported. It further suggests that religious services may provide a good opportunity for promoting knowledge and completion of ADs.
Introduction
The influence of religion and religiosity on end-of-life (EOL) decision making has gained attention among researchers in the past decade. In a study on religious and spiritual support provided to cancer patients at EOL, 88% indicated that religion was at least somewhat important to them. 1 Studies also show significant associations between the various dimensions of religiousness and EOL decisions.2,3 Several studies found that religiosity is influential in advance care planning and in the preference for life-sustaining treatment.1,4 More specifically, greater religiosity generally demonstrates an inverse relationship to advance directive (AD) completion rates as well as in the preference for life-sustaining treatment.5,6 However, these studies largely focus on cancer populations and often use small nonrepresentative samples. Less is known about the association between religiosity and AD completion, and to our knowledge, no existing literature includes a national sample of older adults. Therefore, using a nationally representative sample from the Health and Retirement Study (HRS), 7 this study aims to determine the association between religiosity and AD completion, and among those with an AD, documented EOL care preferences.
Methods
Sample and procedures
This study used data from the HRS core and exit interviews between years 2000 and 2014. The HRS is a longitudinal biennial study that has been conducted in the United States since 1992. It has a nationally representative sample of Americans ≥50 years. The interviews conducted are comprehensive, multidisciplinary, and comprises questions about older Americans' health, retirement, disability, and socioeconomic status, among others. 8 Minorities are oversampled to ensure a nationally representative sample. 9 After the death of a study participant, a final exit interview is conducted with a proxy. The goal of the exit interview is to gather information about the respondent's activities between the last wave of interview and death, as well as the circumstances surrounding the respondent's death. The HRS is sponsored by the National Institutes of Health/National Institute on Aging (Grant NIH R01AG018016) and the Social Security Administration.
Independent variables
In this study, we had three independent variables: frequency of religious service attendance, importance of religion, and religious affiliation. These were found in the HRS core interview. For religious service attendance, the respondent was asked “About how often have you attended religious services during the past year?” and the responses were coded as “at least once a week,” “at least once a year but fewer than once a week,” and “not at all.” Importance of religion was determined by asking, “How important would you say religion is in your life; is it very important, somewhat important, or not too important?” and their responses were coded accordingly. As for religious affiliation, responses were limited to “Protestant,” “Catholic,” “Jewish,” “some other religion,” and “no preference.”
Dependent variables
We had two dependent variables in this study: AD completion and preference for aggressive care at EOL, as asked in the exit interview. Proxies were first asked, “Did [FIRST NAME] provide written instructions about the treatment or care that [she/he] wanted to receive during the final days of [her/his] life?” If the proxy answered yes, then he/she was asked four more questions about if the decisions involved limiting care in certain situations; withholding any treatment; keeping the patient comfortable and pain free; and desire to give all care possible to prolong life. A dichotomous variable was constructed based on these four care choices. If the response was to prolong life, we coded that as preferring aggressive care. For all other responses (limited care, comfort care, or to withhold treatment), we coded that as not preferring aggressive care.
Covariates
Sociodemographic factors and health characteristics were used as control variables, and included age, gender, ethnicity, education, and marital status. We also examined common medical conditions, including cancer, depression, stroke, heart disease, lung disease, and cognitive impairment.
Statistical analysis
Descriptive statistics were employed to describe the key characteristics of the sample, AD completion rates, and EOL care preference. We also ran two logistic regressions. The first was to determine if religiosity was associated with AD completion. A second logistic regression was conducted with the subsample of respondents with ADs to determine predictors of preference for aggressive care. We controlled for sociodemographic factors and health characteristics, and used sample weights. All analyses were conducted using STATA v14 (StataCorp LLC, College Station, TX).
Results
The sample size included 10,591 proxies. However, our analytic sample included 6051 proxies because we restricted our sample to HRS decedents ≥50 years who died between 2001 and 2013. In addition, we omitted observations with missing values for respondent weight, year of death, race, as well as dependent variable domains.
Among the 6051 decedents, 2785 (47.7%) had an AD (Table 1). Almost two-thirds of the overall sample was Protestant (63.0%). There were 26.9% Catholic, 2.6% Jewish, 1.2% of other religions, and 6.4% reported no religious affiliation. Logistic regression revealed that Protestants (odds ratio [OR] = 0.70; confidence interval [95% CI]: 0.50–0.97; p < 0.05) and Catholics (OR = 0.66; 95% CI: 0.47–0.93; p < 0.05) had significantly lower odds of AD completion compared with those who reported no religious preferences (Fig. 1).
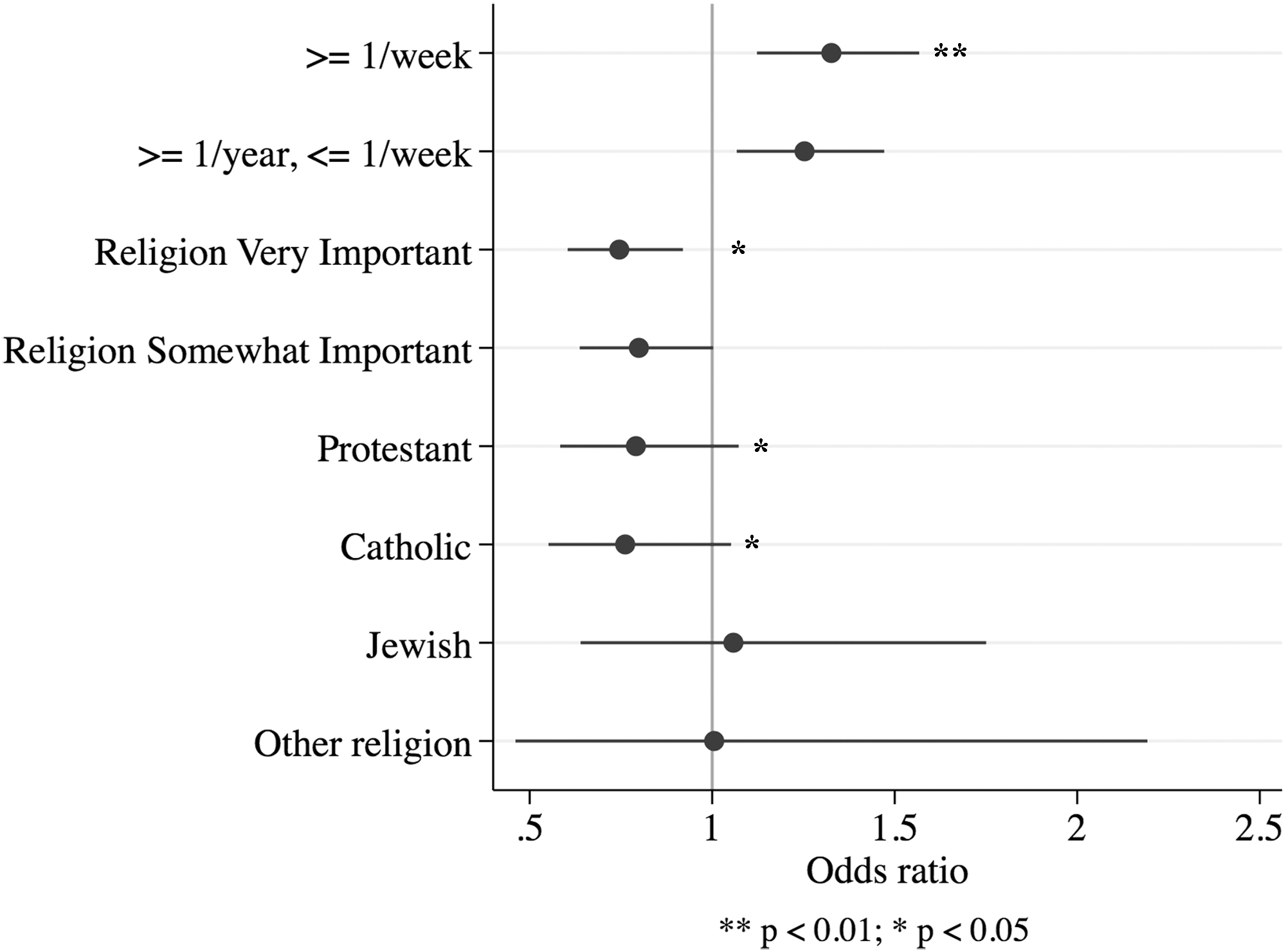
Odds ratios for religiosity predictors of AD completion.
Sample Characteristics
AD, advance directive.
Logistic regression further revealed that decedents reporting religion as very important (OR = 0.78; 95% CI: 0.62–0.98; p < 0.05) had significantly lower odds of AD completion, as opposed to decedents reporting religion as not too important. However, decedents who attended religious services at least once a week had significantly higher odds (OR = 1.30; 95% CI: 1.09–1.55; p < 0.01) of completing an AD than those who did not attend at all. With regard to preference for aggressive care at EOL within the subsample with ADs, neither religiosity nor religious affiliation was significant.
Other covariates that significantly predicted AD completion were age (OR = 1.04; 95% CI: 1.03–1.05; p < 0.001), being divorced or separated (OR = 1.36; 95% CI: 1.04–1.78; p < 0.05), widowed (OR = 1.42; 95% CI: 1.18–1.70; p < 0.001), or single (OR = 1.58; 95% CI: 1.00–2.48; p < 0.05), and having cancer (OR = 1.59; 95% CI: 1.38–1.84; p < 0.001), depression (OR = 1.26; 95% CI: 1.10–1.44; p < 0.01), or lung disease (OR = 1.21; 95% CI: 1.03–1.42; p < 0.05) (Table 2).
Logistic Regression Analyses of Advance Directive Completion and End-of-Life Care Preference among Those Who Completed an Advance Directive
p < 0.001; **p < 0.01; *p < 0.05.
CI, confidence interval; OR, odds ratio.
Ethnic minorities such as blacks (OR = 0.30; 95% CI: 0.24–0.38; p < 0.001) and Hispanics (OR = 0.35; 95% CI: 0.25–0.49; p < 0.001); decedents in the first (OR = 0.63; 95% CI: 0.48–0.82; p < 0.001) and second (OR = 0.79; 95% CI: 0.64–0.98; p < 0.05) income quartiles; and those in the first (OR = 0.61; 95% CI: 0.49–0.77; p < 0.001), second (OR = 0.69; 95% CI: 0.56–0.85; p < 0.01), and third (OR = 0.79; 95% CI: 0.66–0.96; p < 0.05) asset quartiles; were significantly less likely to complete ADs.
Discussion
To our knowledge, this is the first study to examine the association between religiosity variables and both AD completion and care preference in a nationally representative sample. We found the strength of religious belief inversely predicted AD completion, although higher religious service attendance was directly associated with AD completion. These findings support other health-related studies of differences between importance of religion and religious service attendance.10–12 A previous study found that those reporting strong religious beliefs were more likely to believe God controls EOL decisions, 13 hence those who reported strong religious beliefs may be more inclined to surrender their fate to God, versus completing an AD. The social aspect of religious service attendance may account for the association with AD completion; one study of Baptist churchgoers found that 70% cared or are caring for someone with a serious illness 14 and these situations may be shared or discussed with fellow congregation members following church services.
Our findings suggest that religious services may provide a good opportunity for promoting knowledge and completion of ADs, with pilot studies demonstrating the potential success of this approach.15,16 In addition, based on findings from previous research, provision of religious support from medical providers may increase rates of ADs and impact EOL choices. 17 Further research is needed to determine the effectiveness of faith-based AD interventions. Our findings of ethnic differences in AD development mirror those in earlier studies18,19; thus, future research should investigate the interaction between race and religiosity.
The lack of significance in the relationship between religiosity variables and preference for aggressive care among those who completed an AD contradicts some earlier studies. That said, the significant association between race and preference for aggressive care is consistent with existing literature, suggesting that race is a stronger predictor of EOL care preferences. However, a study by Volandes et al. 20 showed that the effects of race were erased when controlling for health literacy. This suggests an alternative to faith-based AD interventions could be community-based interventions through senior centers and other senior-centric organizations.
This study was limited, in that we used proxy responses that possibly introduces recall bias because the HRS exit interviews were conducted with a proxy anywhere between one and three years after the death of the respondent. This study is also limited because it does not take into account other forms of advance care planning, including electing health care proxies or informal discussions about EOL choices.
Funding Information
Health and Retirement Study, public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740), Ann Arbor, MI (2016).
Footnotes
Author Disclosure Statement
No competing financial interests exist.