
Abstract
Introduction:
Patients with serious illness often have pain, uncontrolled symptoms, and poor quality of life. Evidence continues to evolve regarding the role of cannabis to treat chronic pain, nausea, and anorexia. Little is known about how patients with serious illness perceive its benefits and harms. Given that an increasing number of clinicians across the United States are treating patients with medical cannabis, it is important for providers to understand patient beliefs about this modality. We assessed patient perceptions of benefits and harms of cannabis who obtained a medical cannabis card within an ambulatory palliative care (APC) practice.
Methods:
We recruited patients with a medical cannabis card, allowing for legal possession of cannabis oil, from an APC practice in Georgia. All participants reported using cannabis products. Patients completed an online survey that included questions about their cannabis use, concurrent opiate or controlled medication use, and perceptions of benefits and harms of cannabis.
Results:
All 101 patients invited to participate completed the survey. A majority had cancer (76%) and were married (61%), disabled or retired (75%), older than 50 years of age (64%), and men (56%). Most patients ingested (61%) or vaporized (49%) cannabis products. A majority of respondents perceived cannabis to be important for their pain (96%) management. They reported that side effects were minimally bothersome, and drowsiness was the most commonly reported bothersome harm (28%). A minority of patients reported cannabis withdrawal symptoms (19%) and concerns for dependency (14%). The majority of patients were using concurrent prescription opioids (65%). Furthermore, a majority of cancer patients reported cannabis as being important for cancer cure (59%).
Conclusion:
Patients living with serious illnesses who use cannabis in the context of a multidisciplinary APC practice use cannabis for curative intent and for pain and symptom control. Patients reported improved pain, other symptoms, and a sense of well-being with few reported harms.
Introduction
In a majority of states, select patients are allowed to use cannabis for medical use.1–4 Seriously ill patients with a variety of illnesses may qualify for legal possession of cannabinoids of various forms. 5 Georgia law allows qualified patients with a state-sanctioned card to possess low 9-tetrahydrocannabinol (THC) oil (≤5%) with equal or greater amount of cannabidiol (CBD). 6 Patients are increasingly requesting authorization for legal cannabis in ambulatory palliative care (APC) practices that care for patients with comorbid chronic pain, substance use disorder (SUD), and serious illness.7–10 Many patients are referred early in their disease trajectory when opioid therapy for pain or other polypharmacy may confer risk of diversion, dependence, or SUDs. Given the increase in cannabis requests at our institution, we assessed perceptions of cannabis' benefits and harms among patients who reported using cannabis and had a state-sanctioned card in our APC practice.
Methods
Recruitment of participants
Patients were recruited from an academic APC practice serving primarily advanced cancer patients and other serious illnesses. Patients who met inclusion criteria for invitation to complete the survey were (1) at least 18 years of age, (2) an active APC patient, (3) functionally and cognitively capable of completing an online survey, (4) met a qualifying condition for a state-sanctioned cannabis card, and (5) actively procured and carried the card. All patients who reported using cannabis products who met the inclusion criteria were asked to complete a survey at the end of their regularly scheduled clinic appointment. The study was approved by the Institutional Review Board.
Survey
We used experiential data and patient feedback from >1 year of cannabis counseling within the APC clinic to draft the survey. The survey was voluntarily administered from December 2017 to July 2018 during scheduled clinic appointments. No monetary incentives were provided for participation, and patients provided online informed consent for the study. Survey items assessed concurrent opioid and controlled medication use, means of cannabis consumption, and perceptions of benefits and harms. Perceived benefits and harms of cannabis were assessed using a Likert scale from “extremely important” to “definitely not important,” and “extremely bothersome” to “noticeable, but not bothersome,” respectively. All survey items were optional to complete.
Because of the small sample size and variety of cannabis products that patients used, this study is limited to descriptive analysis. Descriptive statistics, including frequency tables with proportions and bar graphs, were used to summarize the data. Wald confidence intervals for proportions were set at 95%. All calculations were performed using SAS software version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Demographics and qualifying conditions for cannabis
Of the 101 patients who were invited to participate in the survey, 100% responded. Fifty-four participants (55.7%) were men. The majority were 50 years of age or older (64.0%) (Table 1). Most patients had at least a high school degree or equivalent (82.6%) and were married (61.2%). Most patients were on disability and reported to be unable to work (56.7%). None were actively seeking employment. Only 15 patients were employed.
Patient Demographics
Includes multiple sclerosis/amyotrophic lateral sclerosis (n = 1), graft-versus-host disease (n = 1), HIV (n = 1), seizures/epilepsy (n = 1), Crohn's disease (n = 1).
GED, general education diploma.
Most patients reported cancer as their qualifying diagnosis for a state-issued card (75.5%) followed by severe peripheral neuropathy (17.0%). The remaining diagnoses were for amyotrophic lateral sclerosis/multiple sclerosis, graft-versus-host disease, seizures/epilepsy, and Crohn's disease.
Forms and frequency of use
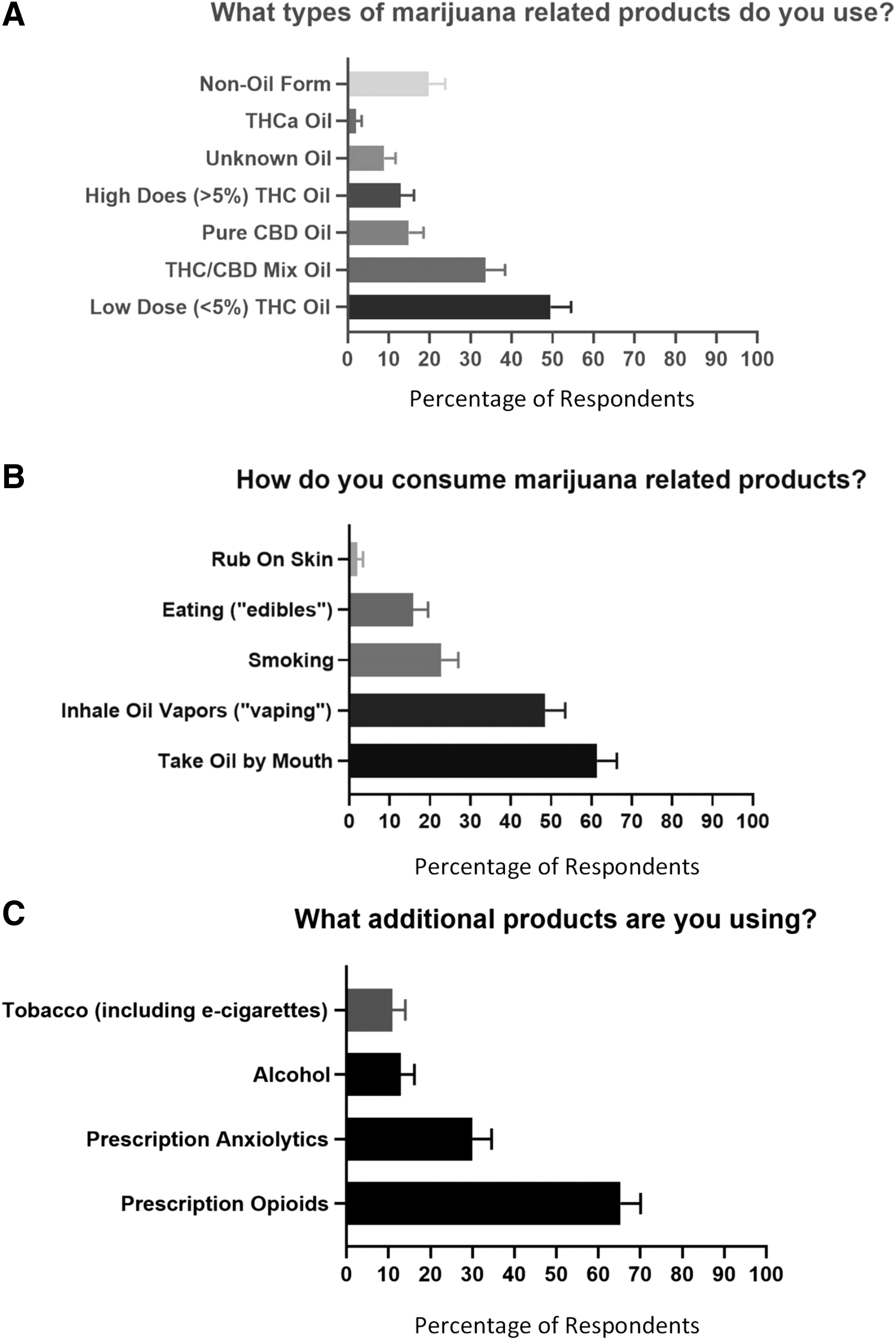
The most commonly reported products used by patients were state-sanctioned low-dose THC (≤5%) oil (49.5%) and mixed THC/CBD oil (33.7%). Of note, patients were able to select more than one product (Fig. 1). A minority of patients used non-oil forms of cannabis (20.0%). The remainder used pure CBD oil (14.9%), >5% THC oil (12.9%), tetrahydrocannabinolic acid (THCa) oil (2.0%), or were unsure of the contents of their oil (8.9%). Patients were allowed to free-text responses, and responses were reclassified to their appropriate category for analysis. Among surveyed patients who used cannabis in the oil form, the majority consumed it orally (61%) or inhaled the oil as a vapor (49%), known popularly as “vaping.” Patients also smoked plant-based cannabis (23%), ingested edibles (16%), or used a topical product (2%). Patients commonly used cannabis multiple times daily (59%) (Table 1).
Cannabis and other medication use
Most patients registered for a state-issued card reported using concurrent opioid therapy (65.3%), and a minority of patients used prescription anxiolytics/sedatives (29.7%), alcohol (12.9%), and tobacco (10.8%) (Fig. 1). No surveyed patients reported taking other schedule I drugs such as heroin, cocaine, or psychedelics.
Perceived benefits and harms
A majority of patients found cannabis to be important or extremely important in reducing pain (95.5%), decreasing anxiety (79.0%), relieving depression/improving coping (77.3%), providing a sense of well-being (73.9%), facilitating sleep (73.0%), increasing energy (69.0%), controlling nausea (66.7%), and stimulation of appetite (62.5%) (Table 2). Patients on concurrent opioid therapy also overwhelmingly reported cannabis as being important or extremely important for pain (95.5%). Among patients with cancer, a majority reported using cannabis products for cancer cure (62.2%).
Patient-Reported Benefits of Cannabis Products
F, frequency; SEP, standard error of percent.
Patients did not report significant harms from cannabis (Table 3). A minority of patients reported drowsiness from cannabis (27.6%), although a few found it bothersome or extremely bothersome (8.1%). Over 10% of patients reported mild to extremely bothersome dizziness, problems with focusing, and confusion. Less than 5% of patients reported bothersome or extremely bothersome (not including mildly bothersome as a category) nausea/vomiting, constipation, hypotension, tachycardia, paranoia, anxiety, depression, headache, thoughts of self-harm, coughing, imbalance, problems with focusing, confusion, mood changes, or hallucinations.
Patient-Reported Harms of Cannabis Products
Patients were able to free text brief narrative responses explaining perceived benefits and harms of cannabis. Selections representative of the collective responses include the following: (1) “makes life with advanced cancer much more bearable…allows me not to focus on my own health issues and to enjoy life as much as possible,” (2) “I no longer wake every 20 to 30 minutes of dread, anxiety, and an utter sense of overwhelming loss. My sleep is sound, deep, and fulfilling,” (3) “reduce dependence on opioids,” and (4) “peace.” Among noted harms, the most common free-texted response was “none” (five respondents) followed by “dry mouth” (two respondents) (Supplementary Tables S1 and S2).
Concerns for dependency and SUDs
A minority of patients reported unpleasant physical or emotional symptoms suggestive of withdrawal including irritable mood, changes in sleep, and pain when stopping cannabis products (19.1%). Few patients reported a perception of mental or physical dependence to cannabis (13.5%). Only three patients were concerned about becoming “addicted” to cannabis. Given the increased risk of developing a SUD among patients with a personal or family history, we asked patients about their personal and family histories. Patients reported a personal (2.2%) or family history (11.1%) of drug or alcohol dependency resulting in rehabilitation program enrollment, and only one patient reported both a personal and family history (Supplementary Fig. S1).
Discussion
Patients with serious illness who use medical cannabis under the supervision of an APC practice report improved pain, symptoms, and a sense of well-being with few reported harms, although a minority of patients endorsed symptoms suggestive of cannabis withdrawal. This study is significant because it explores the benefits and harms of cannabis use in patients with serious illness being seen in an APC that registers patients for medical cannabis cards, and counsels and monitors patients' cannabis use. This differs from studies in palliative care in which only providers' perceptions are explored 11 or cannabis is framed as an illicit drug. 12
The scope of these data extends beyond the state of Georgia to all states with medical cannabis laws. Of note, Georgia and a number of states predominantly in the Southeastern United States have medical cannabis laws but no dispensaries, which may explain why surveyed patients who had low THC oil cards were also using other cannabis products. 13 Further research is needed to clarify the impact of state cannabis laws on patterns of cannabis use.
One startling finding in our study is the high percentage of cancer patients who felt that cannabis has curative properties. This perception may result from messaging in popular media, 14 and necessitates more research to understand how and why certain patients perceive cannabis to be curative.
Our study has several key limitations. We did not verify actual use of cannabis products by drug screening and relied on self-report of cannabis use alone. Our cohort was a self-selected patient population and likely had a greater baseline interest in cannabis as a medical therapy. We limited our study to patients who requested to have a state-sanctioned card and to those who reported use of cannabis. Given the lack of regulation over cannabis products and patients' diverse use of multiple formulations, we were not able to correlate symptom response to specific formulations.
There are significant barriers limiting cannabis-related research including its Schedule I designation.1,15,16 Future investigations should prospectively study the impact of standardized, controlled cannabis formulations on pain, symptoms, and quality of life in populations with serious illness. Based on our clinical experience observing patients' cannabis use in our APC, the role of cannabis in treating comorbid chronic nonmalignant pain, malignant pain, opiate dependence/SUDs, and caregiver quality of life is worthy of inquiry.
Footnotes
Acknowledgments
We thank David Murphy, MD, PhD, and Tammie E. Quest, MD for their contributions to this article.
Funding Information
Ali J. Zarrabi–Fostering the Academic Mission in the Emory Department of Medicine (FAME) Grant, Emory University. Vinita Singh is a KLZ Scholar at the Georgia Clinical and Translational Science Alliance.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.