
Abstract
Background:
Antibiotic prophylaxis is usually adopted to prevent urinary tract infection (UTI) after nephrostomy catheter placement and replacement. This prophylaxis has been little studied in cancer patients, and its efficacy is uncertain.
Objective:
To determine the rate of UTI associated with percutaneous nephrostomy catheters placement and replacement and associated risk factors.
Methods:
This retrospective study collected data from the available medical records. Catheter-related UTI was defined as any diagnosis of UTI based on clinical symptoms recorded in antibiotic prescription charts, and on the results of urine culture collected up to 7 days after percutaneous nephrostomy catheter. The associations between categorical variables were analyzed using Fisher's exact test. The risk factors for UTI were assessed using logistic regression.
Results:
In the univariate analyses, there was no significant difference in the rate of urinary infection between patients receiving and not receiving antibiotic prophylaxis before percutaneous nephrostomy and after replacement.
Conclusion:
The results of the present study suggest that the use of antibiotic prophylaxis for managing urinary tract obstruction by percutaneous nephrostomy is not recommended in cancer patients. In contrast, for catheter replacement, antibiotic prophylaxis appears to have a protective effect for UTI.
Introduction
One of the consequences of the prostate, colon, rectal, cervical, bladder, and ovary cancers evolution is malignant ureteral obstruction.1–5 Treatment adopted to safeguard renal function is urinary tract desobstruction, and nephrostomy catheters are one of the options.6–8
Although ultrasound-guided percutaneous nephrostomy is less invasive for performing desobstruction, complications may occur3,9,10 such as urinary tract infection (UTI), with an incidence rate of 12% to 30%.3,8,10–13
Antibiotic prophylaxis is adopted to prevent UTI after this procedure. However, it has been little studied in cancer patients, with uncertain efficacy.11,14,15
The objective of this study was to determine the rate of UTI associated with initial placement of percutaneous nephrostomy catheters and subsequent replacements, the main etiological agents involved, and the associated risk factors.
Materials and Methods
This retrospective study collected data from the available medical records at the Medical and Statistical Archive Service. The study participants were diagnosed with malignant neoplasm in two hospitals from the Pio XII Foundation: Barretos Cancer Hospital (BCH), in Barretos, and Jales Cancer Hospital (JCH), in Jales, both in the São Paulo state, Brazil, and selected based on information available in the database of the Department of Radiology of the two hospitals.
The patients were subjected to ultrasound-guided percutaneous nephrostomy, performed by the interventional radiology team at BCH from August 2014 to December 2015 and at JCH from July 2012 to December 2015.
The first procedure (catheter placement) is performed during percutaneous nephrostomy for managing urinary tract obstruction. The standard routine of antibiotic prophylaxis consists the use of cefazolin before nephrostomy (empirical prophylaxis). For catheter replacement, this same protocol was adopted at the JCH until April 2013, after which targeted antibiotic prophylaxis was used depending on urine culture and antibiogram results, collected ∼7 days before nephrostomy (targeted prophylaxis). At BCH, catheter replacement followed the standard prophylaxis routine throughout the study.
Catheter-related UTI was defined as any diagnosis of UTI based on clinical symptoms recorded in antibiotic prescription charts, and on the results of urine culture collected up to 7 days after percutaneous nephrostomy catheter placement or exchange.
Two databases were created: one contained information on patients and the other contained information on procedures. Both databases had a unique identifier, allowing data correlation between them. The study population was characterized by descriptive statistics.
The associations between categorical variables were analyzed using Fisher's exact test. The risk factors for UTI were assessed using logistic regression. The level of significance adopted in all statistical analyses was 5%. SPSS software version 21 was used in all analyses.
The study was approved by the research ethics committee of our institution under the Certificate for Ethics Assessment number 50812115.3.0000.5437.
Results
The recruitment and selection of the study participants are shown in Figure 1.
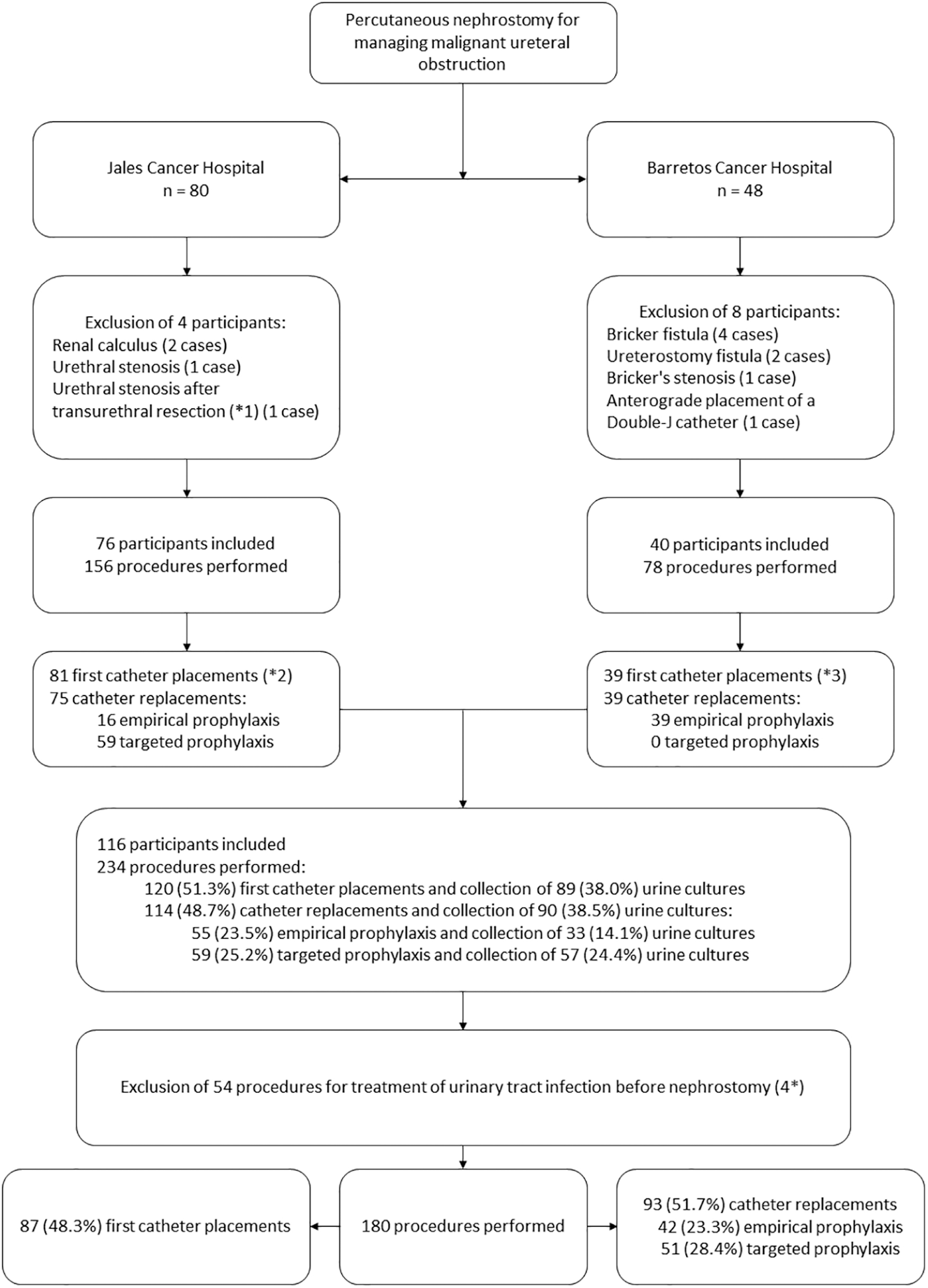
Schematic representation of the study sample. (*1) Transurethral resection. (*2) This number was higher than the number of participants because of catheter withdrawal due to regression of neoplastic disease, with subsequent progression, new ureteral obstruction, and new treatment for obstruction. There have also been cases of treatment of new obstruction on the contralateral side of the same patient. (*3) This number was smaller than the number of participants because in one patient, initial catheter placement was not performed by the interventional radiologist but by the urologist using a different catheter. However, it was possible to evaluate this patient because the catheter exchange procedures complied with the inclusion criteria of the present study. (4*) Except for microbiome analysis.
The sociodemographic and clinical characteristics of the patients and the characteristics of the procedures are summarized in Table 1. The median age of the patients was 60 years, ranging from 17 to 92 years.
Sociodemographic and Clinical Variables of Patients and Characteristics of Percutaneous Nephrostomy Procedures Performed for Treatment of Malignant Ureteral Obstruction
JCH, Jales Cancer Hospital; BCH, Barretos Cancer Hospital.
Endometrium (one patient), rhabdomyosarcoma (one patient), unknown primary site (one patient), body of the uterus (one patient), and vagina (one patient).
Information not available (two patients).
Information not available (three patients).
Information not available (18 procedures).
Antibiotic prophylaxis was performed before initial nephrostomy catheter placement in 79.3% of the cases and before catheter exchange in 84.9% of the cases (p = 0.337).
First placement of the percutaneous nephrostomy catheter
The distribution of cases of UTI after the first procedure is shown in Table 2. The overall rate of UTI after initial placement was 1.2%. There was no significant difference in the rate of UTI between patients receiving (0%) and not receiving (1.5%) antibiotic prophylaxis before percutaneous nephrostomy (p = 0.999).
Associations between the Time of Nephrostomy Catheter Placement, Antibiotic Prophylaxis Protocols Used, and Urinary Tract Infection after the Procedure
The results of urine culture collected before initial catheter placement indicated the occurrence of microbial growth in 36.8% of the cases. The identified pathogens are described in Figure 2.
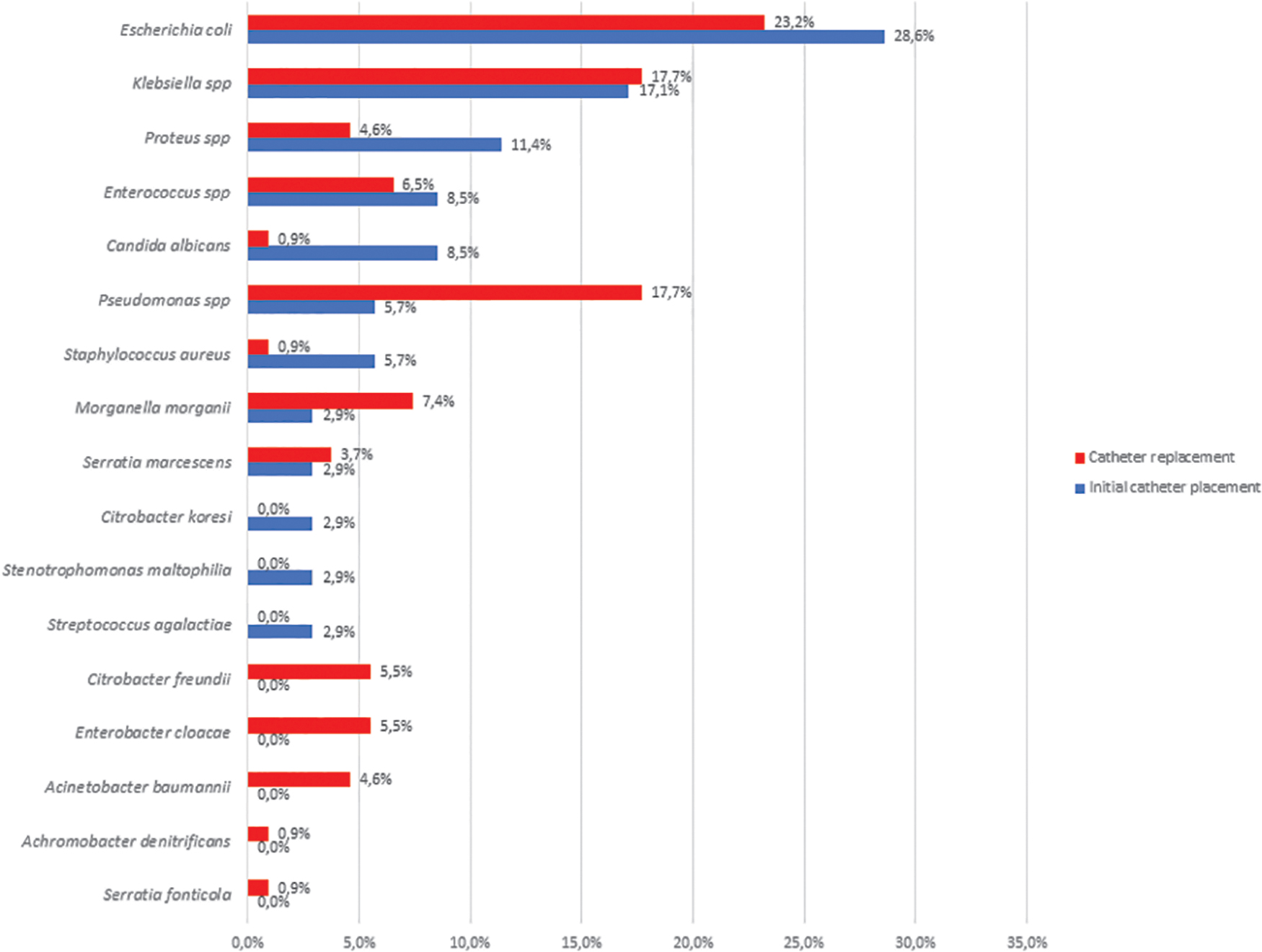
Results of positive urocultures asked before the first placement (n = 35) and replacement (n = 108) of the nephrostomy catheter.
During initial catheter placement, 77.8% of the antimicrobial agents used for prophylaxis of UTI were not effective against the identified microorganisms.
Replacement of percutaneous nephrostomy catheter
The distribution of cases of UTI after catheter exchange is shown in Table 2. The overall rate of UTIs after catheter exchange was 11.4%, which was significantly higher than that obtained after initial catheter placement (1.2%; p = 0.010).
After catheter exchange, the rates of UTI were 21.4% in patients who did not receive antibiotic prophylaxis, 14.8% in those who underwent empirical antibiotic prophylaxis, and 6.4% in those who received targeted antibiotic prophylaxis (p = 0.146).
Microbial growth was observed in 90.8% of the urine culture samples collected before catheter replacement. The identified pathogens are described in Figure 2.
More than one microbial agent was found in 26.7% of urine cultures collected at the time of catheter exchange and in 6.7% of urine cultures collected during initial catheter placement (p < 0.001).
The percentage of antimicrobial agents used for prophylaxis of UTI that were not effective against the identified microorganisms was significantly lower in catheter replacement (18.5%) compared with initial placement (77.8%; p = 0.001).
Discussion
These results suggest that antibiotic prophylaxis before the first placement of nephrostomy catheters has small benefit in preventing UTIs whose rates after initial catheter placement were similar between patients subjected or not to antibiotic prophylaxis.
The overall rate of UTI after first procedure was lower than that found in previous studies, which ranges from 12% to 30%.4,5,8,10,12 Bahu et al. 11 found that the incidence rate of nephrostomy catheter-related pyelonephritis was 19%. This difference may be due to the shorter analysis of the period of development of UTI in the present study. The retrospective nature of our study may have limited the correct identification of all cases of UTI. Despite the high rate of pyelonephritis found by Bahu et al., antibiotic prophylaxis did not significantly decrease the rate of this complication after catheter placement. 11
The rate of UTIs after catheter replacement was higher than that obtained after initial catheter placement. Furthermore, the rate of UTIs was nonsignificantly higher in patients subjected to empirical antibiotic prophylaxis compared with those receiving targeted antibiotic prophylaxis. This result is related to the reduced statistical power imposed by the sample size. Larger prospective studies are necessary to further elaborate this finding.
Although the level of significance was not reached, the authors believe that antibiotic prophylaxis plays some role in preventing UTIs after nephrostomy catheter replacement, particularly for prophylaxis based on the results of urine culture collected before catheter exchange, which also allowed the more rational use of antibiotics.
The rate of UTIs after catheter replacement in the present study was higher than that reported by Bahu et al. 11 (4%) because in the present study, the follow-up period was longer, increasing the number of catheter replacements, and increasing the probability of UTIs.
There was a significant difference between the profile of the microbiome before initial catheter placement and replacement, and there was bacterial colonization secondary to the presence of a foreign body in the urinary tract.
The use of antibiotics for other infectious complications, or even the unnecessary use of antimicrobials, may justify the discrepancies in the microbiome before the initial placement and exchange procedures.
The logistic regression analysis did not identify risk factors for UTI after replacing nephrostomy catheters. Bahu et al. reported that neutropenia and the diagnosis of UTI before treatment of urinary tract obstruction were risk factors for catheter-related infections. 11
The presence of nitrite and bacteriuria has not been shown to be risk factors for UTI in this population. Leukocyturia was diagnosed in 98.2% of the urine samples. In 89.1% of these, no cases of UTI were observed (data not shown). It may be due to the colonization of the urinary tract by microbial pathogens, leading to inflammation of the renal pelvis urothelium.
The limitations of the present study include the retrospective nature of data collection, which increases the possibility of biases, particularly those related to the difficulty in differentiating between catheter-related UTI and treatment of asymptomatic bacteriuria. The presence of a positive culture without signs of UTI after nephrostomy has been documented in the literature.11,15,16 Nonetheless, this study is unprecedented on this subject, especially in an oncological population.
Likewise, these patients may have infections or be colonized by multidrug-resistant organisms (MDRO), and the present study data may have some relevance in the rational use of antibiotics and in the more accurate diagnosis of UTI being able to avoid MDRO implications, including higher mortality and morbidity, difficult decision making in palliative care related to treating or not treating these infections in the last days of life of the patient with advanced disease, and worse the psychosocial burden due to the need for contact precautions and isolation. 17
Therefore, the use of antibiotic prophylaxis for managing urinary tract obstruction by percutaneous nephrostomy may be not recommended in cancer patients. For catheter exchange, antibiotic prophylaxis appears to have a protective effect for UTI. If targeted prophylaxis is not available, the profile of the microbiota colonizing the urinary tract after catheter placement should be analyzed, depending on the characteristics of each institution.
Footnotes
Acknowledgments
The authors would like to acknowledge all team that support the idea and believed in it, such as the Nucleus of Support to the Researcher, the Nucleus of Epidemiology and Statistics, and the Institute of Education and Research from Pio XII Foundation—Barretos Cancer Hospital
Funding Information
No funding was received for the development of this study.
Author Disclosure Statement
No competing financial interests exist.