
Abstract
Background:
In health care, clinical effectiveness involves evaluating the degree to which clinical interventions achieve beneficial patient and caregiver outcomes.
Objective:
To evaluate the clinical effectiveness of care in a specialist palliative care unit (SPCU) in Ireland, including an analysis of the temporal relationship among admission, Phase of Illness and patient and family distress.
Design/Measurements:
A consecutive case series with prospectively collected admission data (n = 400). Using a casemix tool (Phase of Illness), pain, other symptoms, psychological and family distress, and performance status were documented on admission and then daily by medical staff.
Results:
Three hundred forty-two (85%) patients had complete data recorded on day 1. After admission, there were linear correlations between days since admission and progressive improvements in pain (Cramer's V = 0.131, p < 0.001), other symptoms (V = 0.206, p < 0.001), psychological distress (V = 0.101, p < 0.001), and family distress (V = 0.124, p < 0.001). Forty-three percent were in an unstable phase on admission. Nearly two thirds (60.7%) of these unstable patients converted to a stable phase within 48 hours of admission. Over the first 72 hours, 70.7% of unstable patients converted to a stable phase. There was also a significant correlation between phase stabilization and pain and symptom control (p = 0.007). Stable phase over the first 4 days and first 14 days was associated with significantly higher performance status.
Conclusion:
This study demonstrates the significant clinical effectiveness of SPCU admission across the different aspects of patient and family care.
Background
Clinical effectiveness is defined as the application of the best knowledge, derived from research, clinical experience, and patient preferences to achieve optimum processes and outcomes of care. 1 Many measures have been proposed to evaluate the efficiency and effectiveness of palliative care interventions; however, most have not been tested or evaluated prospectively or longitudinally. 2 Multiple metrics have been evaluated with the aim of demonstrating clinical effectiveness.3–7 To demonstrate clinical effectiveness, we must monitor our effect on patient and caregiver outcomes and collect data in a manner that is minimally burdensome to patients, caregivers, and staff. In palliative care, five phases of patient illness have been identified: stable, unstable, deteriorating, terminal, and bereaved. 8 The Palliative Care Problem Severity Score (PCPSS) is a tool that quantifies case complexity for pain, other symptoms, psychological distress, and family/caregiver distress and scores each domain on a 0–3 basis. 9 As such, the overall score is out of 12. Patient Phase of Illness, PCPSS and functional status has been proposed as a casemix model for palliative care. 8 This model has been developed and implemented nationally in Australia. To date, no prospective studies have tracked the daily effect of specialist palliative care unit (SPCU) admission on patient, family, and caregiver outcomes.
Aims
To evaluate the clinical effectiveness of care in a SPCU in Ireland, including an analysis of the temporal relationship among unit admission, the patient's Phase of Illness and different aspects of patient and family distress. An additional aim was to evaluate the relationship between patient phase and other aspects of casemix.
Methods
This was a consecutive case series with prospectively collected data of 400 consecutive admissions to a SPCU between May 1st, 2014 and January 10th, 2015 using three tools for data collection. All patients admitted to the inpatient unit receive a comprehensive assessment and management plan to address their physical symptoms, psychosocial and spiritual distress, and family/caregiver distress by a consultant-led multidisciplinary specialist palliative care team, which includes doctors, specialist nurses, physiotherapy, occupational therapy, social work, complementary therapy, and pastoral care. Casemix was evaluated using the Phase of Illness and the PCPSS. In addition, functional status was documented using the Palliative Care Performance Scale.
Casemix model
The term casemix has several meanings, from the literal “mix of cases (patients)” seen by a consultant/hospital/region, to the way in which patient care and treatments are classified into groups. These groups are useful for performance comparisons, to cost health care, or to fund it. 10 Many casemix models use diagnosis-related groups to capture patient-driven resource utilization. 11 In Palliative Medicine, care is driven by patient need rather than diagnosis. The Australian casemix model was developed and published by Eagar et al. in 2004. 8 It evaluates casemix complexity using different domains unrelated to the patient diagnosis, including PCPSS, Phase of Illness and performance status.
Palliative Care Problem Severity Score
Developed by Smith and Firms in 19949 and again by Eagar et al. in 2004,
8
the PCPSS aims to numerically evaluate the complexity of a patient's and family's casemix across four domains. Each is scored from zero to three, with zero indicating the absence of distress and three indicating severe distress in the domain. The overall score is out of 12. The PCPSS incorporates the following domains:
Pain (0–3) Other symptoms (0–3) Psychological distress (0–3) Family and caregiver distress (0–3)
The PCPSS is clinician rated, scored daily and is now advocated by the Australian Palliative Care Outcomes Collaboration (PCOC) for routine screening of all Palliative Care patients in Australia. 12 It is complemented in the Australian model by the Symptom Assessment Scale (SAS), a patient-rated distress measure. 13
Phase of Illness
This refers to a distinct clinical period, 9 which reflects illness stage. It is a good indication of the type of care required. An episode of inpatient palliative care may have a single phase or multiple phases. Phases are not sequential and a patient may move back and forth between phases within the one episode of inpatient palliative care. 14 The PCOC defines five phases of a patient's illness: stable, unstable, deteriorating, terminal, and bereaved. 14 Patients and their families/caregivers can move between phases in any order and can be in any phase more than once. These phases are defined in Figure 1. 14

Phase of Illness definitions.
Palliative Performance Scale
This is a validated and useful15,16 scale that measures functional status from 0% to 100%. In the original model by Eagar et al., 8 the RUG-ADL scale was used. PCOC has since supplemented this with the Australian-modified Karnofsky Performance Scale (AKPS). 14 Like the AKPS, the Palliative Performance Scale (PPS) is a validated tool and is scored from 0% to 100%. As the PPS was already being routinely used in our SPCU, it was used for the purposes of this study.
Data collection
Ethics approval was received from the University Hospital Limerick Research Ethics Committee (March 2014). Phase of Illness and the four domains of the PCPSS were documented on admission by the admitting doctor and thereafter on a daily basis by the medical team. Scores were documented on a specially developed scoring sheet (Fig. 2) along with other scores about the intensity of activity of health care professionals to be reported elsewhere. Once weekly, the sheets were removed from the medical notes and scores entered into Microsoft XL by administration staff. These were then transported to SPSS for statistical analysis and descriptive statistics generated by the University of Limerick Statistics Department.
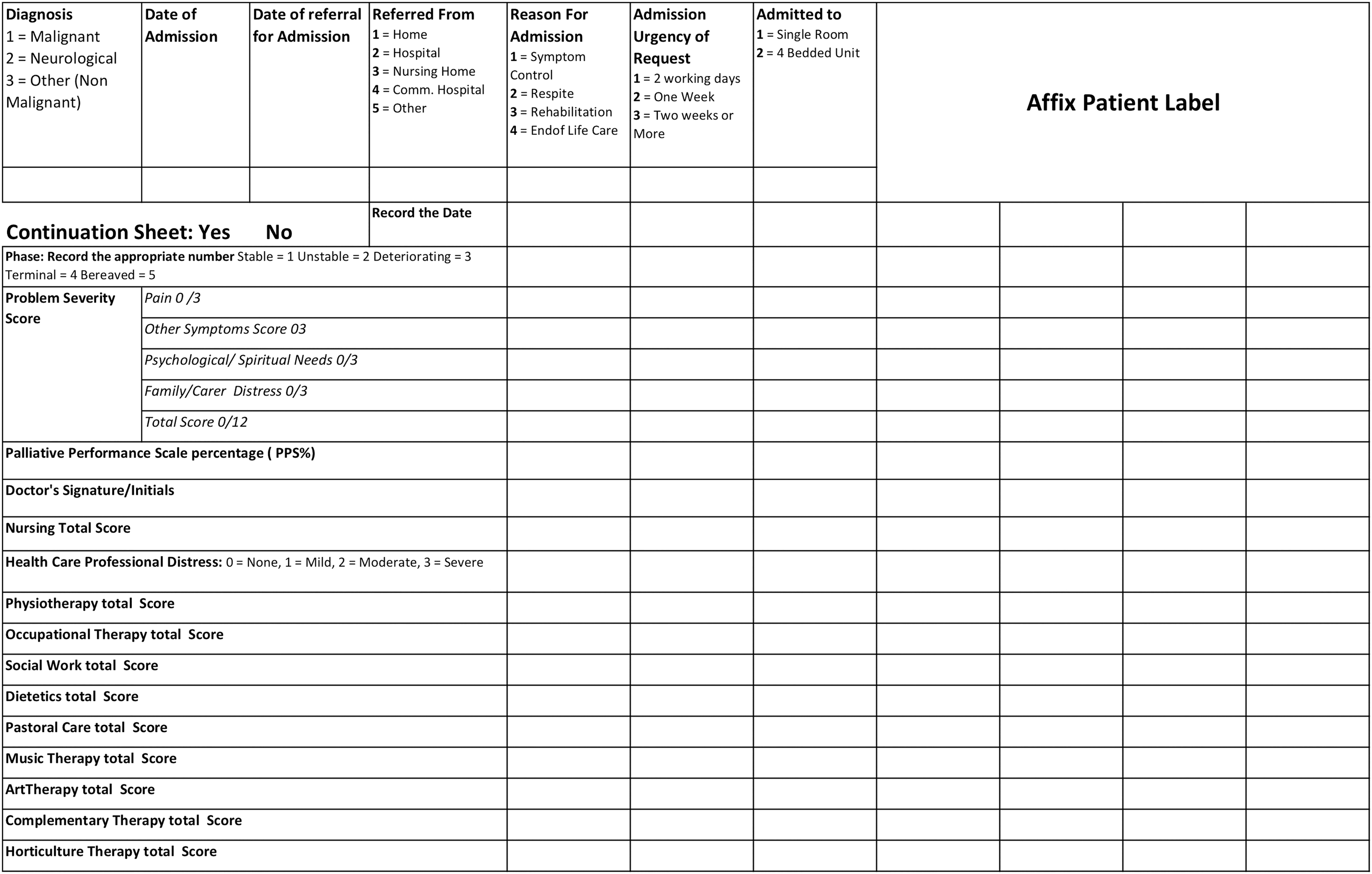
Copy of data collection template.
Results
Three hundred forty-two of the 400 consecutive patients admitted (85%) during the study period had complete data recorded on day 1. On admission 147 (43%) were in an unstable phase, 98 (28.6%) in a stable phase, 76 (22.2%) in a deteriorating phase, and 21 (8.7%) in a terminal phase.
Pain
Pain scores decreased after admission. A significant temporal relationship was identified between pain and time from admission; high, medium, and low pain scores all improved in a significant, progressive, and linear manner after admission (X 2 = 76.34, df = 1, p < 0.001) (Fig. 3).
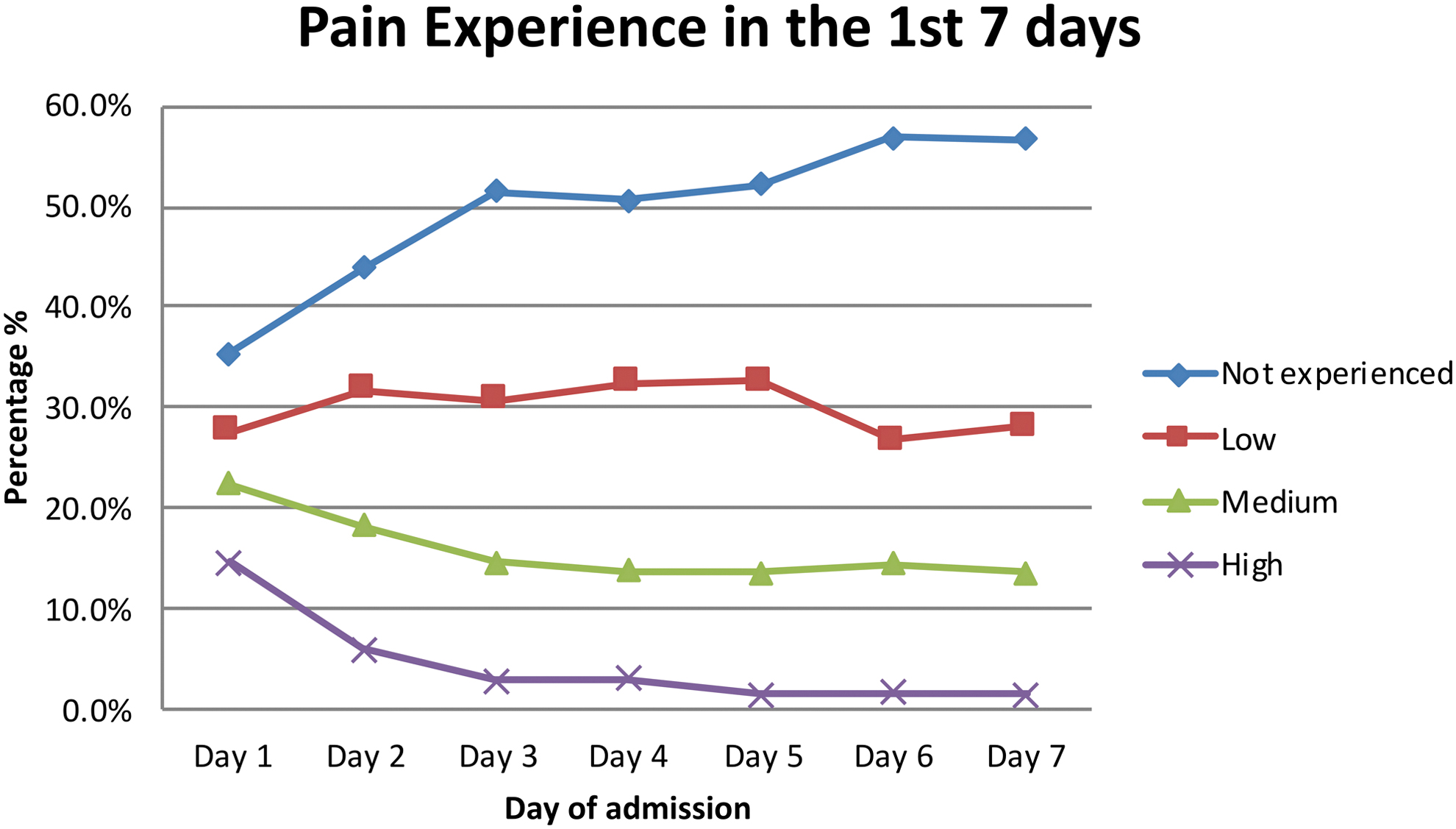
Pain profile by day.
Symptoms other than pain
Symptoms other than pain decreased in a significant, progressive, and linear manner after admission (X 2 = 214.47, df = 1, p < 0.001) (Fig. 4).
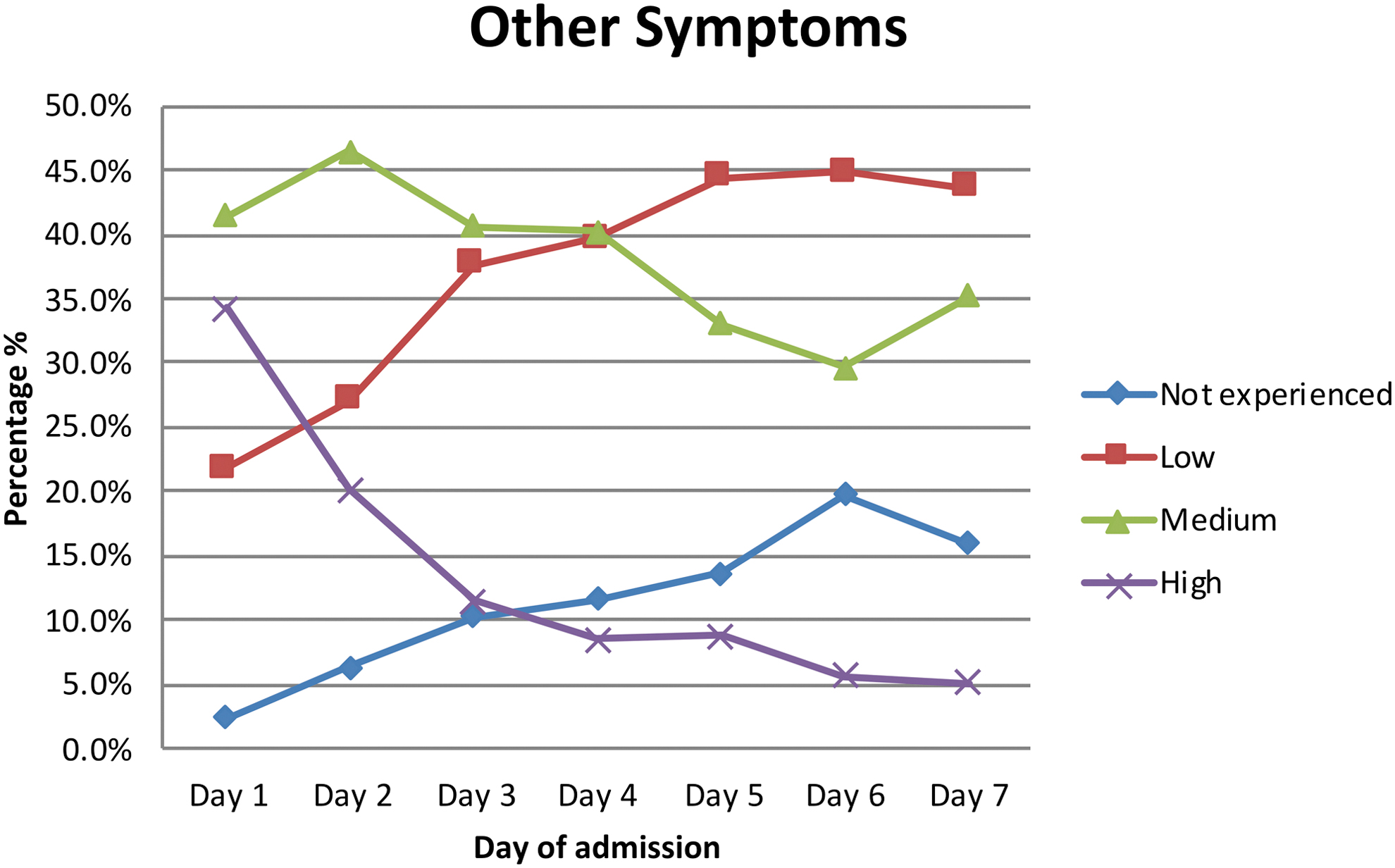
Other symptoms profile by day.
Psychological and spiritual distress
Psychological and spiritual distress decreased in a significant, progressive, and linear manner after admission to the inpatient unit (X 2 = 45.13, df = 1, p < 0.001) (Fig. 5).
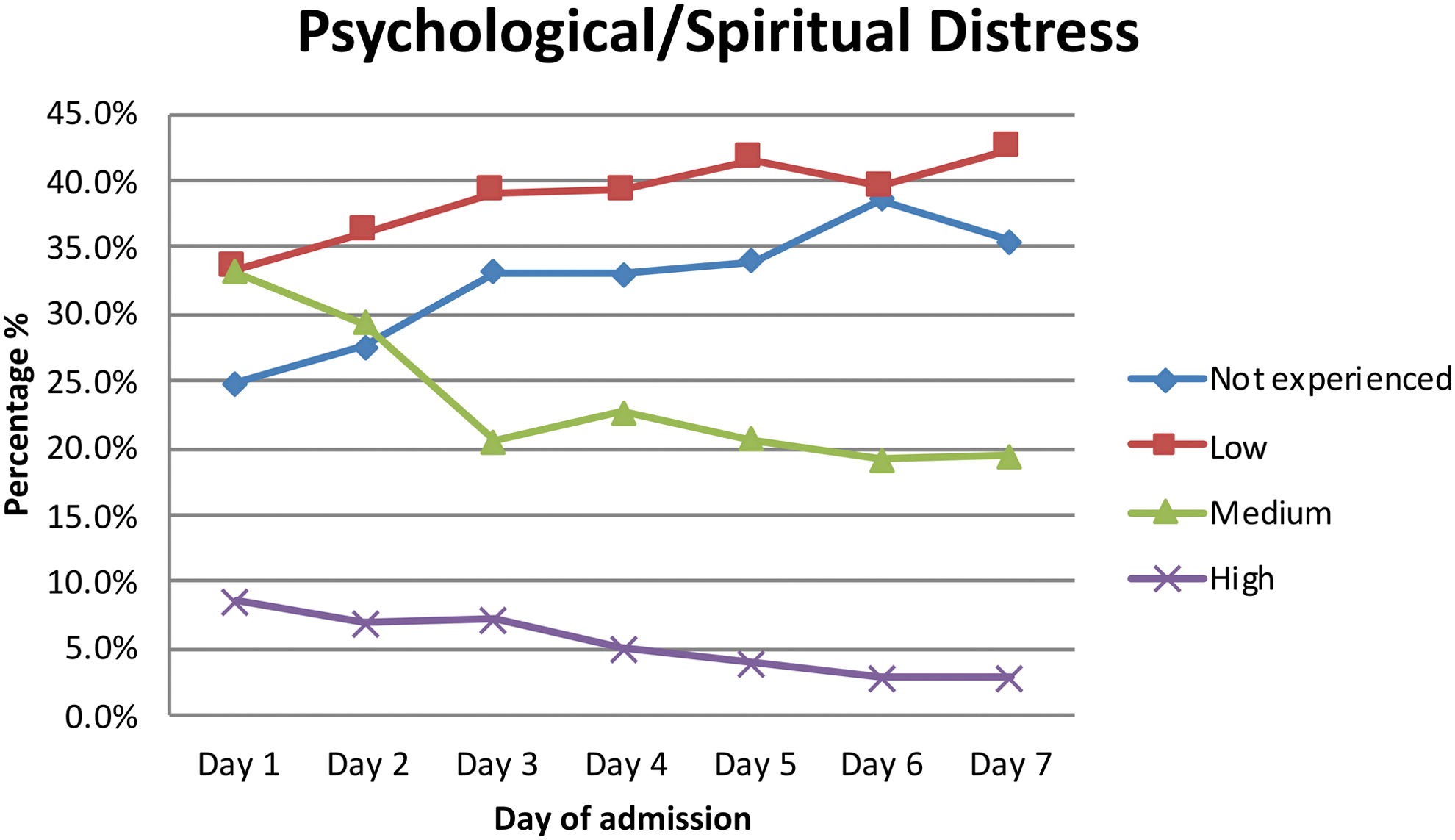
Psychological/spiritual distress by day.
Family and caregiver psychological distress
A linear relationship was demonstrated with regard to family/caregiver distress and time after admission (X 2 = 75.06, df = 1, p < 0.001). That is, family/caregiver experience of medium and high distress decreases from admission (Fig. 6).

Family/caregiver distress by day.
Phase of illness
Unstable phase
For this study, we concentrated on patients in the unstable phase on admission. This is because in Australia, a key national indicator and benchmark is “time spent in the unstable phase” with an aim to minimize this. When looking at a direct phase change from unstable to stable, 54.6% (n = 68) directly entered stable from unstable, 29.8% (n = 37) remained unstable, 13.7% (n = 17) entered a deteriorating phase, and 1.6% (n = 2) entered a terminal phase over the first 72 hours (Table 1). Pain, other symptoms, psychological and family/caregiver distress, all reduced significantly regardless of phase after admission. This highlights the benefit of SPCU admission regardless of phase at admission.
Crosstabulation Showing Phase Progression from Day 1 to Day 4
Day 1 is day of admission, day 2 is 24 hours following admission, day 3 is 48 hours following admission, day 4 is 72 hours following admission.
Patients may move between phases after admission (e.g., unstable on admission, deteriorating at 48 hours, but improved and classified as stable at 72 hours), and it is important to track phase changes as a quality measure. Of the 147 patients admitted who were in the unstable phase, 74 (60.7%) became stable within 48 hours, and 87 (70.7%) were stable within 72 hours.
Phase over time
Following admission, the proportion in the stable phase progressively increased and the proportion in the unstable and deteriorating phase progressively decreased over time (linear association between phase of illness and time after admission) (X 2 = 19.64, df = 1, p < 0.001). This can be seen in Figure 7.

Phase progression by day.
Phase associations with pain, other symptoms, and psychological distress
Chi-square analysis revealed that those in the unstable, deteriorating, and terminal phases were significantly more likely to have higher pain scores (Cramer's V = 0.180, n = 3266, p < 0.001). That is, Phase of Illness was associated with pain severity. Chi-square analysis also revealed that those in the unstable, deteriorating, and terminal phases are significantly more likely to have higher “other symptom” scores (Cramer's V = 0.180, n = 3266, p < 0.001). That is, Phase of Illness was associated with symptoms other than pain. Further analysis revealed that those in the unstable, deteriorating, and terminal phases were significantly more likely to have higher psychological/spiritual distress scores (X 2 linear association = 3.738, Cramer's V = 0.153, n = 3362, p < 0.001). That is, Phase of Illness was clearly associated with patient psychological and spiritual distress. Finally, patients in the unstable, deteriorating, and terminal phases were significantly more likely to have higher family and caregiver distress scores (X 2 linear association = 161.94, Cramer's V = 0.140, n = 3361, p < 0.001). That is, Phase of Illness was associated with family and caregiver distress.
Phase and functional status
Over the first 4 days and the first 14 days, a stable phase was associated with higher performance scores (Cramer's V = 0.526, p < 0.001). Different phases were associated with differing performance scores (Fig. 8).
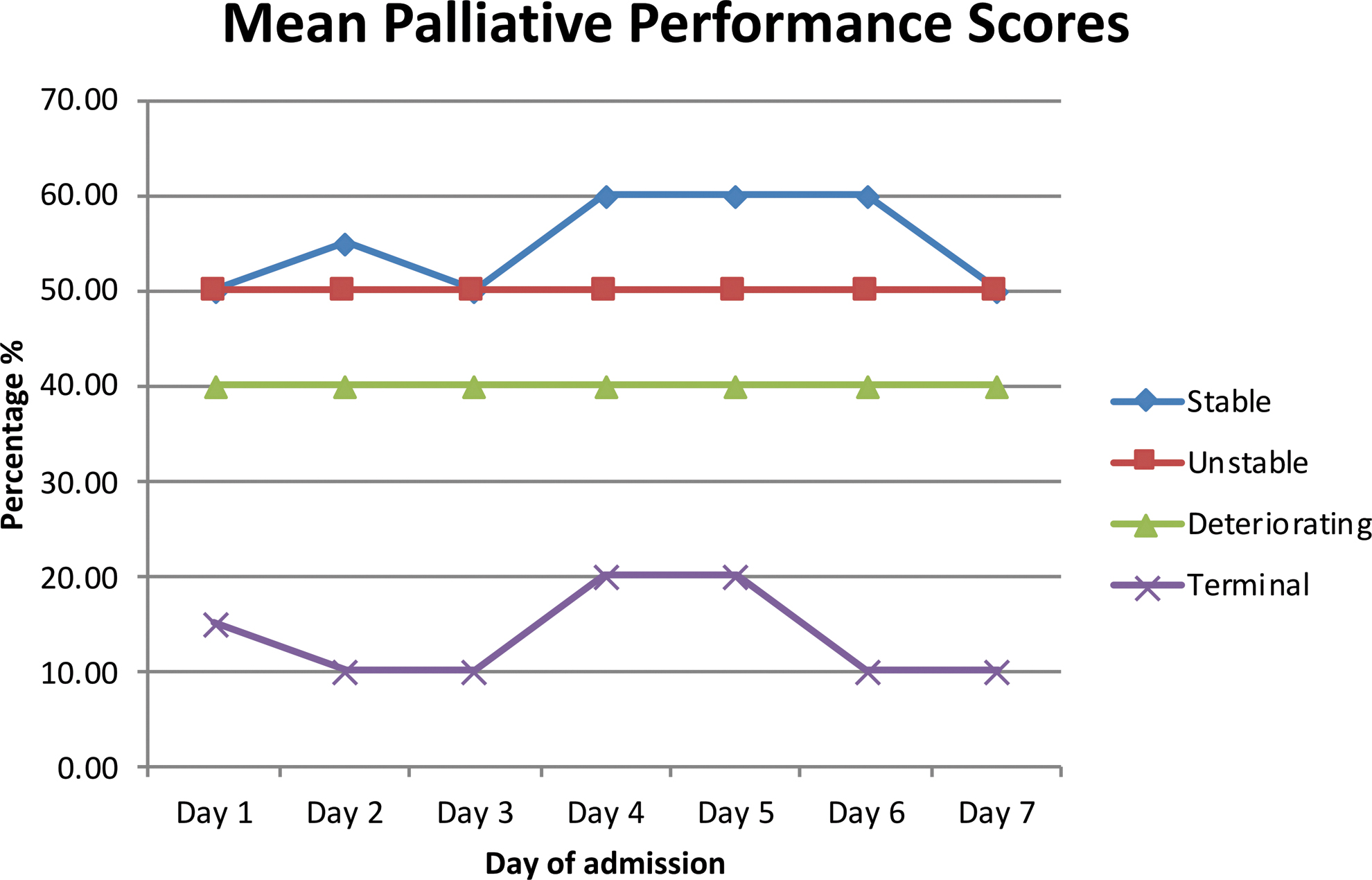
Mean palliative performance score.
Discussion
Clinical effectiveness needs to be measured to establish how well interventions work. It is necessary to demonstrate that clinical interventions achieve worthwhile benefits in practice settings and controlled research environments. 17 We prospectively explored patient and family-related outcomes related to clinical inputs from staff in a SPCU. Clinical performance has traditionally focused on both mid- and high-level process measures.2–7 These are vital for service management, but the most important aspect of service delivery is patient and caregiver outcomes. For this reason, outcome measurement is becoming increasingly important in health care, both general and palliative care. 18 The importance of patient and family/caregiver-reported outcome measures has been well documented and well-validated tools have been developed to measure these. Examples include the ESAS, 19 the POS, 20 the SAS, 13 and SKIPP 21 tools for patients, and the VOICES 22 and POS for families and caregivers.
However, the daily self-reporting for some of these tools can be burdensome, time consuming, and impractical for weak patients and distressed families. 23 The use of proxies for weak and ill patients and those at end of life is unavoidable. 24 There has long been debate as to the accuracy of proxy reporting for symptoms and quality of life and who should be the proxy reporter, a family member, or clinician. There is little difference between family caregiver and health care professional (HCP) in symptom assessment25–28 and most studies show that congruence increased over time with repeated assessments.29–31
Studies also show greater concordance between patient and proxy in relation to concrete observational symptoms like pain, nausea, etc.32,33 unlike subjective symptoms such as low mood, high anxiety, and poor quality of life, which tend to be overestimated by proxies.34,35 This study utilized the HCP proxy rating of the Phase of Illness, pain, other symptoms, psychological and spiritual distress, and family/caregiver distress as advocated for routine screening by the PCOC since 2012. 12
To address the limitations of proxy rating in the unit, the “SAS” has been added to the casemix model. This is a seven-item patient-reported outcome-measuring tool that patients score alone or with the help of a caregiver or health care professionals. This is in concordance with the PCOC casemix model in Australia. 13
Recently, studies have demonstrated the benefit of the addition of palliative care to usual care versus usual care alone on quality of life, mood, and even survival. 36 Some studies demonstrate that home palliative care increases the chance of dying at home and reduces symptom burden in particular for cancer patients. 37 However, no studies have been undertaken using temporal mapping of Phase of Illness, symptom and psychological distress after admission to a SPCU to ascertain the effectiveness over time of the interventions. Phase of Illness has been deemed crucial for patient care in Australia, with time spent in the unstable phase a national benchmark. Phase of Illness is reliable and acceptable in palliative care 38 with good inter-rater reliability. 39
Our study demonstrates that 70% of patients admitted in the unstable phase become stable within 72 hours. In addition, the proportion in the stable phase increases and the proportion of patients in the unstable and deteriorating phase of illness decreases in a linear and progressive manner after initial admission. This study also demonstrated the strong and significant relationship between Phase of Illness and all aspects of patient and caregiver distress.
The stable phase is associated with better patient and caregiver outcomes whereas patients in the unstable, deteriorating, and terminal phases have progressively higher symptom and psychological distress scores and progressively reduced functional status. However, even when unstable phase patients do not become stable (becoming deteriorating or terminal phase instead), all aspects of patient symptoms and distress, along with family and caregiver distress also reduced in a statistically significant, linear, and progressive manner, indicating the benefits of admission to a SPCU for all patients who were in an unstable phase. This supports the use of Phase in routine practice for casemix classification and for the identification of patients in greatest need. It also supports the routine documentation of Phase and the PCPSS to track casemix trajectory over time and to demonstrate clinical effectiveness. This methodology can readily be transferred to any inpatient unit and we are piloting a community and daycare version in north Dublin and in the Mid-west in Ireland.
Strengths and limitations
A clear strength of this study in documenting patient and caregiver outcomes is its simplicity and lack of burden on patients and their families. However, a limitation is the use of a proxy rating of patient and family outcomes, as these can be variable and at odds with patient and family-reported outcome measures. In addition, although widely used in Australia, the PCPSS has not been formally validated since its initial development more than 20 years ago.
Summary of study findings from a patient and caregiver perspective:
Forty-three percent of patients admitted to the SPCU were in an unstable phase at the time of admission.
60.7% of these stabilized to a stable phase within 48 hours.
70.7% of patients in the unstable phase on admission stabilized to a stable phase within 72 hours.
The proportion of patients in the stable phase increases and the proportion of patients in the unstable and deteriorating phase of illness decreases in a linear manner after initial admission.
Pain, other symptoms, psychological distress, and family/caregiver distress all decrease in a linear manner after admission to the unit.
Unstable phase is significantly associated with pain, other symptoms, psychological and spiritual distress, and family/caregiver distress.
Phase is significantly associated with all elements of patient complexity.
The above demonstrates the clinical effectiveness of inpatient palliative care.
Conclusion
This study demonstrates the clinical effectiveness of admission to a SPCU and also demonstrates what can be achieved for patients with complex symptoms and psychosocial distress outside of the acute hospital system. It further develops the casemix model developed in Australia and uses this to track patient and caregiver outcomes. Patient Phase of Illness is clearly demonstrated to be associated with all aspects of casemix with stable phase being associated with consistently better patient and caregiver outcomes, and unstable phase and other phases being associated with poorer outcomes. This model is now being piloted in Community Palliative Care and Specialist Palliative Day Care nationally in Ireland. It is an example of a proxy rating system that can be used as part of a service quality model that should also utilize the available patient-reported outcome measures and service process measures to demonstrate clinical efficiency and effectiveness in Palliative Care.
Footnotes
Acknowledgment
The authors would like to thank Dr Jean Saunders, Statistician at the University of Limerick, for her help in analyzing data.
Funding Information
The authors received no financial support for the research, authorship, or publication of the article.
Author Disclosure Statement
No competing financial interests exist.