
Abstract
Background:
Incorporating patient narratives into the electronic health record (EHR) is an opportunity to integrate patients' values and beliefs into their care and improve patient–clinician communication.
Objective:
The study's aims were to (1) identify barriers and facilitators influencing the implementation of a cocreated patient narrative intervention and (2) assess the acceptability/usability of the patient's narrative from the perspective of key stakeholders—the patient and acute care bedside nurse.
Design:
We used an implementation design using mixed methods.
Setting/Subjects:
Twenty patients and 18 nurses were enrolled from five units in an acute care hospital.
Results:
For patients, the narrative intervention provided an avenue to discuss and share how illness has impacted their life in psychological, social, and spiritual belief domains. For nurses, the ability to read the patient's narrative provided benefits that fostered improved communication and more connection with their patients. Despite successfully meeting recruitment targets, time was the largest barrier for patient and nurse participants. Overall, the nurse participants gave high ratings on most of the items on the System Usability Scale with one exception—EHR integration. The lack of EHR integration on the System Usability Survey corresponds with the nurses' stated desire for a prominent location of patient narratives in the EHR.
Conclusions:
The patient narrative intervention was acceptable and usable for hospitalized patients and nurse participants. Our study demonstrates that a cocreated patient narrative intervention provides avenues for patients and nurses to connect despite being in hectic acute care settings.
Trial Registration:
ClinicalTrials.gov NCT03391115
Introduction
There is a growing population of racial and ethnic minority patients 1 with serious illnesses in the United States who are underserved by palliative care. Minority patients with serious illnesses and/or their caregivers desire to discuss care preferences with clinicians, yet they do so at lower rates than white patients.2–4 Alarmingly, minority patients with serious illnesses often do not receive treatment consistent with their wishes.1,2,5 These disparities are often caused by poor clinician–patient communication about patient-centered interventions, creating care inconsistent with patient's preferences.2–6 A better understanding of patient perspectives helps clinicians tailor palliative care interventions centered on patients' cultural values and beliefs.7–9 The use of a patient narrative is an effective way to communicate cultural values and beliefs.10,11
In health care settings, the electronic health record (EHR) is one of the primary modes of communicating information about patients to the health care team. Incorporating patient narratives into the EHR is an opportunity to integrate patient values and beliefs into their care and improve patient–clinician communication. This study assessed the feasibility of an innovative intervention to incorporate patients' values and beliefs into their care through integration of a cocreated patient narrative into the patient's EHR to improve communication between a hospitalized patient and the acute care bedside nurse.
Methods
Study design
We used an implementation design 12 using mixed methods (quantitative survey and qualitative interviews). Study aims were to (1) identify barriers and facilitators influencing the implementation of a patient narrative intervention and (2) assess the acceptability and usability13,14 of the patient narrative intervention from the perspective of key stakeholders—the patient and acute care bedside nurse.
The Consolidated Framework for Implementation Research (CFIR) was used to describe the breadth and depth of data collected for this study. 12 The CFIR has five domains: (1) intervention characteristics, (2) characteristics of individuals, (3) outer setting, (4) inner setting, and (5) process of implementation.12,15,16
Intervention characteristics
The patient narrative intervention is a written narrative document cocreated between the principal investigator (PI) and the patient/family. First, the PI asked patients to share their narratives based on open-ended interview questions about how their illness had affected their psycho–social–spiritual well-being (Supplementary Data A.) For this narrative interview, the PI created a 1–2-page patient-focused narrative metastory based on the audio recording and field notes. Consistent with narrative analysis methodologies, 17 this metastory of each individual's story incorporates details of the patient narrative noted during the interview. After the narrative interview, the interviewer wrote a first draft of the metastory, which is a written, first-person patient narrative. Next, the written narrative was returned to the patient for review and editing within 24–48 hours after the narrative interview. Once the cocreated narrative was approved by the patient, the PI uploaded it into the progress note section of the patient's EHR. Finally, the PI verbally notified the assigned nurse that the narrative was available (Fig. 1).
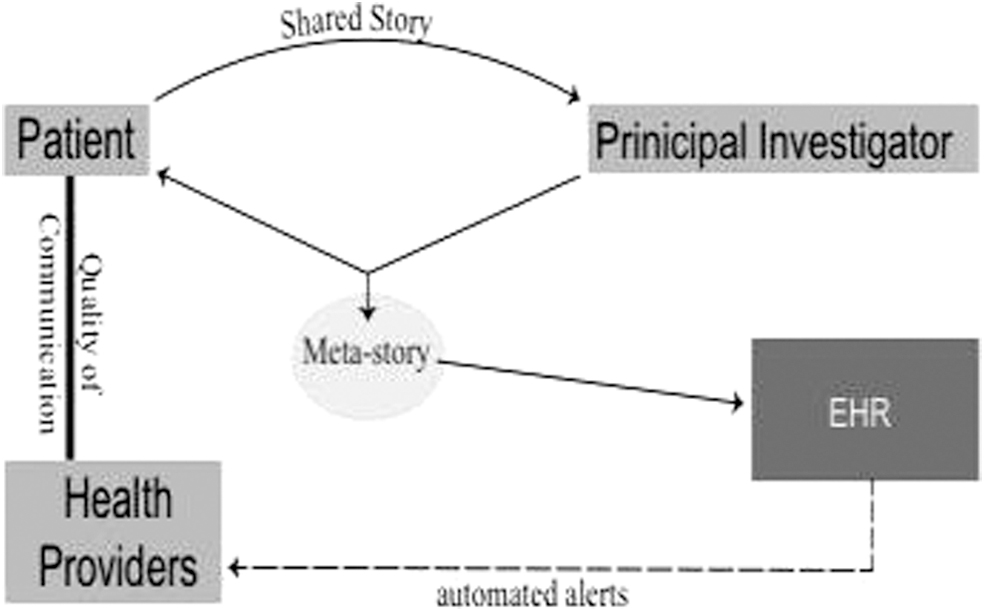
Patient narrative intervention.
Characteristics of individuals
Participants formed a dyad: a patient hospitalized with a serious illness who self-identified as a minority and their assigned acute care bedside nurse.
Outer and inner settings
The outer setting was the academic institution. The inner setting included five units in an acute care hospital. The study was approved by two Institutional Review Boards (IRBs): the academic institution and hospital from which participants were recruited.
Process of implementation
The PI obtained agreement from the hospital administration to implement the narrative intervention in participating hospital units that cared for patients with cancer, heart failure, chronic obstructive pulmonary disease, and/or end-stage renal disease receiving hemodialysis. Through collaboration with the nursing hospital administration and dedicated unit nurse managers, the PI educated the nursing staff at staff meetings about the patient narrative intervention and how to refer eligible patients to the study. Throughout the study, the participating nurse managers received monthly to semimonthly e-mails relaying the number of patients recruited and notifications of when patient narratives were uploaded into the patient's EHR.
To facilitate recruitment of patient participants, the PI did weekly recruitment rounds in all five participating units. Once the PI identified a potential participant, she introduced the study by reviewing the patient recruitment flyer and the informed consent with the patient. Interested patients completed the informed consent, and the PI scheduled a convenient time for collecting the patient's narrative and demographic information. After the PI uploaded each cocreated patient narrative into the patient's EHR, the PI verbally instructed the patient's assigned nurse on where to locate the patient narrative in the EHR.
Data collection
Acceptability
The PI conducted semistructured exit interviews with each patient and nurse participant. On average, exit interviews occurred three days (range one to eight days) after narratives were uploaded into patients' EHRs. Interviews were audio-recorded and transcribed verbatim. Exit interviews included semistructured questions on the acceptability of the patient-focused narrative intervention (Supplementary Data A).
Usability
The nurse participants were asked to rate the usability of the integrated EHRs and patient narratives using the System Usability Scale.12,13,18 The system usability instrument has 10 items and is scored on a 5-point scale representing strength of agreement (strongly disagree to strongly agree). Scores range from 0 to 100. Scores of 70 or above are passable; scores between 80 and 90 denote better usability; and scores of 90 or above are considered superior usability ratings.12,13
Data analysis
We used descriptive statistics to summarize quantitative data using SPSS, version 24, 19 and we used a qualitative descriptive approach 20 to analyze the exit interviews on barriers and facilitators. Using a deductive approach, the first author organized each individual participant's verbatim quotes into a matrix. 21 This matrix was organized by each semistructured interview question and by nursing unit. The completed matrix was used to evaluate participants' responses to each individual question as a barrier to or facilitator of the intervention. Findings were examined and discussed among all authors until reaching consensus about the final classifications of barriers and facilitators. To organize the data, we used the Atlas.ti, v.8, software. 22 To increase the transparency of our interpretation, we have included verbatim quotes from patient and nurse participants within the text and in Table 1. The verbatim quotes in the text are depicted by quotation marks.
Verbatim Quotes from Exit Interviews: Patient/Nurse
Results
Recruitment, enrollment, and retention
The PI completed 249 recruitment rounds, during which the PI met with charge nurses to identify potential patients. Charge nurses and the PI identified 145 potential patient participants, but excluded 65 for a variety of reasons (Fig. 2).
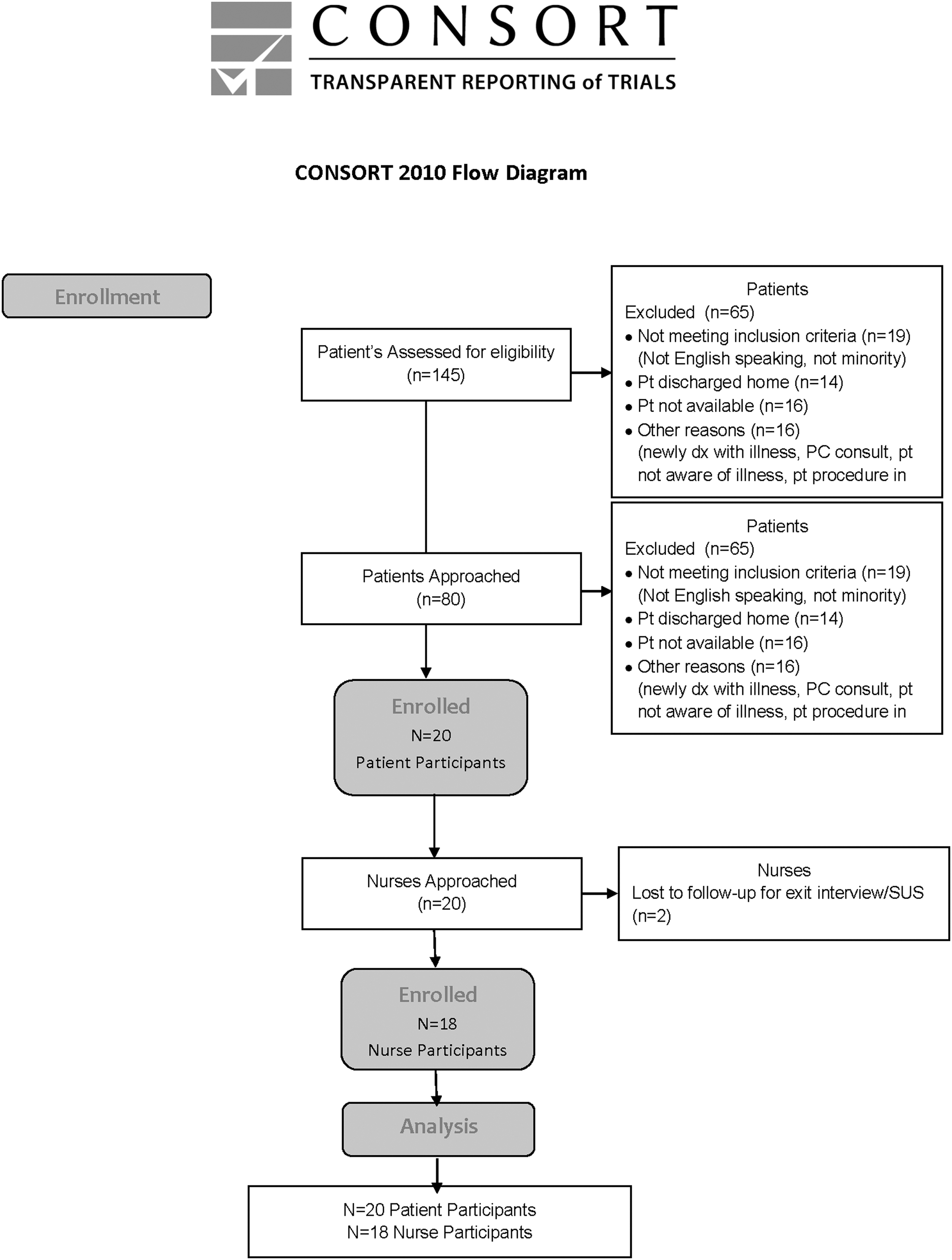
Enrollment diagram.
Twenty patients and 18 nurses from the five units enrolled in the study (Tables 2 and 3). During the 12-month study period (November 2017 to November 2018), 20 of the 80 approached patients enrolled in the study, a 25% enrollment rate. Twenty nurses were approached, 18 enrolled in the study, a 90% enrollment rate. One nurse consented, but unenrolled for personal reasons. One nurse did not set up an exit interview.
Patient Demographics
In all tables, continuous variables are reported with their mean and SD, while categorical variables are reported with the sample size and percent within each subcategory.
SD, standard deviation.
Type of illness does not sum to 100% as (n) 2 patients had more than 1 condition.
ESRD, end-stage renal disease.
Nurse Demographics
In all tables, continuous variables are reported with their mean and SD, while categorical variables are reported with the sample size and percent within in each subcategory.
Using the CFIR, three units were high implementation units and two were low implementation units.12,15,16 Seventy-five percent of the participants were recruited from the cardiac medical (n = 8), cardiac progressive care (n = 7), and dialysis units (n = 4). Only one patient was recruited from the pulmonology unit (Fig. 2).
Cocreated patient narrative
The average length of the cocreated patient narrative was 2.4 pages (shortest: 3404 words; longest: 10,693 words). The average time to collect the narrative was 50 minutes (range 29–71 minutes). The average time to write the narrative was 90 minutes (range 58–122 minutes). The average time for patient's review was 49 minutes (range 17–81 minutes).
Exit interviews: Patient
All 20 participants felt being in the study was not burdensome, rather they reported that participating in the study was easy and enjoyable. Two participants said that being interviewed was emotional; however, they felt that having this emotional response was beneficial. Three participants reported uneasiness with participating in the study for the following reasons: (1) stimulating sad emotions, (2) reading their story not told in their voice, (3) needing to edit while in hospital, and (4) concern for how the story affected treatment decisions. Eighteen participants discussed their story with others, including family (n = 12), friends (n = 2), and health care team members (n = 15), which included nurses (n = 9), physicians (n = 3), and nursing aides (n = 2). Eighteen participants confirmed willingness to participate in a similar type of intervention in the future. Eighteen participants felt that the questions asked were not difficult to answer. Five participants suggested improvements to the intervention. Suggestions included the following: (1) make the story longer (n = 2); (2) spend more time in the interview process (n = 1); (3) increase staff's awareness about the narrative (n = 1); and (4) add a picture to the narrative (n = 1).
Exit interview: Nurse
All 18 nurse participants described having a positive experience with the intervention. Nurses described the intervention as eye opening, giving them a different perspective about their patients, which led to better understanding “of what they [the patients] are going through emotionally and physically.” Nurses noted that patient stories enabled them to connect with patients. Seventeen nurses noted that the intervention “helped them improve how they related to patients, gain insights about patients' backgrounds, change their perspective of patients, and deepen their respect for patients.” Three nurses noted that the stories gave them more empathy and understanding. One nurse noted that the intervention calmed the patient and made the patient more compliant. Thirteen nurses indicated positive patient reactions, saying that patients “were proud or excited to be able to share their narratives, more positive or conversational toward staff, in better moods, more relaxed, and felt heard.”
Two nurses noted negative patient reactions that included sadness. However, these nurses also noted that this sadness was temporary and the “process had a positive impact in terms of helping the patient process his or her diagnosis.” Seven of the nurses initiated discussion of the patient narrative directly with their patients. Six initiated the conversation with the patient, and one nurse said the patient asked her directly about his narrative. One nurse indicated that she did not know if she was supposed to discuss the narrative with the patient. All of the nurses who participated in the study indicated that they read the narrative, but some read the narrative after the patient had been or was in the process of being discharged or transferred. Other nurses indicated that they did not discuss specifics of the narrative with the patient, but felt the narrative came into general conversation with the patient.
Nine nurses described difficulties with the study. Difficulties included (1) narrative location in the EHR or lack of notification (n = 4); (2) time to devote to reading the narrative or timing of the narrative delivery related to nurse schedule (n = 2); (3) negative emotions brought up by the narrative (n = 1); (4) researcher interrupting nursing care (n = 1); (5) potential for a negative reaction of the patient (n = 1), and (6) identifying patients as minority for enrollment (n = 1). Nine nurses did not report any difficulties.
The location of the patient narrative in the EHR was the primary complaint of the end user. Twelve nurses reported that the EHR placement of the narrative was adequate. Five nurses indicated that the integration of the narrative into the EHR did not work because it was hard to notice or find. These comments are consistent with the lower score on the integration item on the System Usability Scale. Fourteen nurses offered additional comments to improve the intervention. Suggestions included (1) placing the patient narrative in a more prominent location in the EHR, (2) improving the notification system to alert the nurse that the patient narrative had been uploaded, (3) making the narrative shorter, and (4) bolding important components of the narrative.
System Usability Survey
The average System Usability Survey (SUS) composite score was 89.71, SD = 11.11, range 75 to 100, which almost achieved the superior usability rating of 90 or above12,13 (Supplementary Data B). When we evaluated the individual scores of each item on the SUS, all items were above 90, with the exception of item 5: “I found the various functions in the product were well integrated.” This finding was consistent with the nurse exit interview responses supporting the need for the patient narrative to be located in a more prominent place in the patient's EHR.
Discussion
The patient narrative intervention was acceptable and usable for hospitalized patients and nurse participants. Using the CFIR, intervention characteristics, outer setting, inner setting, characteristics of individuals, and process are discussed below to determine where facilitators and barriers occurred and what implementation improvements will be required for future studies.
Intervention characteristics
Despite successfully meeting recruitment targets, time was a barrier for patient and nurse participants. For patients, this involved trying to schedule the narrative interview around busy inpatient days and when they felt well enough. Despite some of these barriers, some patients wanted more time to create longer narratives. For nurses, time issues involved incorporating reading of narratives into their daily workflow. Despite the barrier of time, however, patients and nurses reported high levels of satisfaction with the narrative intervention.
For patients, the narrative intervention provided a way for them to share how illness impacted their meaning in life. These findings are consistent with other literature discussing similar benefits when patient narratives have been integrated into patient care.10,11,23 Future studies incorporating this narrative intervention will test for effects on patient's psychological, social, and spiritual well-being.24,25 Research has shown that patients' values and preferences are not well represented in their care,3,26 so clinicians need an increased understanding of the patient's psychological, social, and spiritual needs to codevelop tailored care centered on patient's values and beliefs.7–9 Of note, the patient narrative only captured one point in time of the patient's narrative. Future studies might investigate how to capture the patient's narrative over time and provide opportunities to integrate the evolved patient's narrative into the patient's EHR.
For nurses, the ability to read the patient's narrative provided benefits that fostered improved communication and more connection with their patients. Future studies incorporating this narrative intervention will test for the patient's perceptions of the nurse's quality of communication because patient-centered communication is a core component of person-centered care.26–28
Characteristics of individuals
All patient participants had to self-identify as a minority due to the inclusion criteria of the study. Only three of the nurses, however, self-identified as a minority. Three nurses felt it did help them relate better to patient. In future studies, we will enroll participants from all ethnicities/races and continue to collect data not only on the efficacy but also on the acceptability of the narrative intervention across diverse populations. Acceptability could be significantly different in some cultures based on their accepted norms of direct versus indirect communication preferences, trust/mistrust of research and health care, and level of acculturation to individualistic U.S. culture.
Outer and inner settings
For successful collaboration between academic and hospital settings, the hospital (key) stakeholders are particularly important for successful implementation. The comparison across five units revealed differences that impacted the uptake of the intervention. Based on unit differences in the proportion of enrollment, three units were high implementation units and two were low implementation units (oncology and pulmonology). 14 Despite meeting inclusion criteria, 23 patients declined to participate because of uncontrolled physical symptoms. After three recruitment visits, these participants were unable to participate due to pain, nausea, and/or dyspnea. In future studies, patients who have cancer or chronic obstructive pulmonary disease (COPD) may be more likely to participate in an outpatient setting instead of when they are hospitalized for uncontrolled symptoms.
Process
The recruitment processes were successful. We posit that the acceptability of the narrative intervention stemmed from the engagement of both patient and nurse, providing an opportunity for an interactive exchange that was beneficial for both parties to connect outside of the traditional physiological focus in health care. The opportunity to provide a connection between the patient and nurse was one of the greatest facilitators to implementation. The largest barrier for the patient and nurse was time. However, this barrier was overcome through buy-in by the patient and nurse. Another intervention limitation is the implementation costs related to the time to collect, write, and upload narratives beyond a research protocol. The barriers of time will require further intervention refinement to provide efficiency and sustainability.
Regarding usability, the study was successful. Overall, the nurse participants gave high ratings on most of the items on the SUS with one exception—EHR integration. The lack of EHR integration on the SUS corresponds with the nurses' stated desire for a prominent location of patient narratives in the EHR. This was not an unanticipated suggestion. However, since this was a small pilot study, the EHR informatics team deemed it unreasonable to give the patient narrative a prime EHR location. For future studies, the patient narrative would warrant a better location in the EHR.
Conclusions
Maintaining person-centered care is a critical challenge in the U.S. health care system. However, a therapeutic person-centered approach is commonly believed to have positive effects on patient outcomes.29,30 Our study demonstrates that a cocreated patient narrative intervention can help preserve the voice of patients who self-identify as a racial/ethnic minority and provide avenues for patients and nurses to connect despite being in hectic acute care settings. As we move forward, we plan to explore ways to make the integrated narrative intervention sustainable in our setting and to conduct a pilot study to test the effects on patient–nurse communication and patients' psychosocial health.
Footnotes
Acknowledgments
The authors would like to acknowledge the patients who were willing to share their narratives and the nurses who engaged with the narrative intervention. In addition, the authors would like to thank Claudia Amura, PhD, for her assistance with quantitative data analysis procedures and data visualization.
Author Contributions
All authors made substantial contributions to the design of the work or acquisition, analysis, or interpretation of data; participated in revising it critically; provided final approval of the version to be published; and agreed to be accountable for the work.
Funding Information
Research reported in this article was supported by the National Institutes of Health, National Institute of Nursing Research, under award numbers K24 NR015340 and K99 NR016686.
Author Disclosure Statement
No competing financial interests exist.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.