
Abstract
Objective:
The aim of this study was to describe the patterns of discharge and re-enrollment to a community palliative care service, and to identify factors associated with re-enrollment.
Background:
Community-based palliative care is a limited resource. The evidence base to guide discharge practices from community palliative care services is limited.
Methods:
A retrospective audit of the electronic medical records for all patients discharged from the Sacred Heart Community Palliative Care Service (SHCPCS), Sydney, from July 2010 to July 2016 was conducted. Patients were excluded if they were discharged due to death, transferred out of catchment area, declined the service, transferred to another hospital, or were referred inappropriately.
Data extracted included sociodemographic variables, living situation, diagnoses, and discharge and re-enrollment details. Using binary logistic regression analysis, predictive factors, including socio-demographic characteristics, diagnosis and length of episode of care, were evaluated.
Results:
Of the 739 patients who met the inclusion criteria, 42 (5.7%) were re-enrolled to the service. The median length of the initial episode of care was 65 days and the median timeframe between discharge and re-enrollment was 216 days. Patients living in residential care facilities (odds ratio [OR] 3.45; 95% confidence interval [CI] 1.28–9.28; p = 0.01) and those with malignant diagnoses (OR 2.22; 95% CI 1.00–4.93; p = 0.04) had higher rates of re-enrollment.
Discussion:
The proportion of patients re-enrolled to the service was low. Both patient factors and disease factors were associated with re-enrollment. Future prospective studies evaluating prognostic factors to assist with effective discharge processes and guidelines are warranted.
Introduction
Community palliative care services play an integral role in helping people with life-limiting illnesses to live as well as possible, either in their homes or in a residential aged care facility (RACF). These services may range from managing symptoms in patients who are still receiving treatment and assisting with advance care planning, to supporting people who receive end-of-life care at home.
In Australia, the demand for palliative care services has been increasing. The Australian Institute of Health and Welfare reported that between 2014 and 2018, there was an 18.5% increase in the total number of government subsidized palliative medicine specialist services (from 299.1 to 354.5 per 100,000 people). In the same report, hospitalizations for palliative care increased by 25.6% between 2013 and 2017. 1 The increase in demand is multifactorial. First, the population is aging with increasing medical complexities. 2 Second, both the improved survival of cancer patients and earlier referral of cancer patients to palliative care services3–5 mean that cancer patients need palliative care services for a longer period. 6 Third, there is increasing recognition that patients with nonmalignant advanced organ disease also need palliative care services. 7
This increased demand means specialist palliative care services must employ efficient models of care in which services provided are responsive to the needs of the community. To optimize resource use, patients who have stable symptoms and no specialist care needs should be managed by their primary care provider(s). In accordance with the framework described by Palliative Care Australia, formal links with and access to specialist palliative care providers should be available as required. 8 For those patients with fluctuating symptoms, re-enrollment into the community palliative care service should occur whenever the primary care provider requires specialist input.
Although there is considerable literature evaluating the referral processes to specialist palliative care services,3–8 there are limited data to guide the discharge practices from specialist palliative care services. 9 In particular, there is a dearth of literature describing discharge patterns from specialist community palliative care services. One American study that evaluated patients who were enrolled into community-based palliative care found that re-enrolment back into palliative care after previous discharged occurred in 17.8% of discharged patients within a two-year period. 10 Another study based in the United Kingdom found that about 12% of patients were re-enrolled in their service after previous discharge within a six-month period. 9 The primary objective of this study was, therefore, to describe patterns of re-enrollment to a community palliative care service and identify factors associated with re-enrollment to the community palliative care service. The secondary objective was to review service delivery issues, including the reason(s) and appropriateness of initial discharge for those patients who were re-enrolled.
Methods
Setting
Sacred Heart Community Palliative Care Service (SHCPCS) is a specialist consultative metropolitan service in Sydney, Australia, that covers a defined geographical catchment area of ∼400,000 people. Patients are referred to the service by either their treating specialist or general practitioner. The service has a multidisciplinary team that includes medical, nursing, physiotherapy, occupational therapy, social work, psychology, and bereavement services that performs home visits. The nursing staff visits homes seven days a week, and patients have access to a 24-hour telephone helpline. On average, 750 patients are referred to the service each year.
After referral, patients are triaged by telephone, and an initial assessment is undertaken at the patient's home. A case manager is assigned to each patient. There are currently no formalized discharge criteria; if a patient has been stable for approximately three months, their case manager may discuss their case at a weekly multidisciplinary meeting to seek agreement that specialist palliative care input is no longer required. If there is consensus, the patient and the patient's general practitioner would be contacted regarding the plan for discharging the patient from the service and further information about re-enrolling the patient is provided should it be required in the future.
Data collection
We conducted a retrospective audit of the electronic medical records of all patients discharged from SHCPCS from July 2010 to July 2016. To assess the factors associated with re-enrollments, patients were excluded if they were discharged from the service due to death, transferred out of area, declined the service, transferred to another hospital, or were referred inappropriately. The classification of reasons for discharge was determined by the patient's case manager (Fig. 1). The remaining eligible patients were dichotomized into two groups: Patients who were re-enrolled were compared with those who were not re-enrolled.
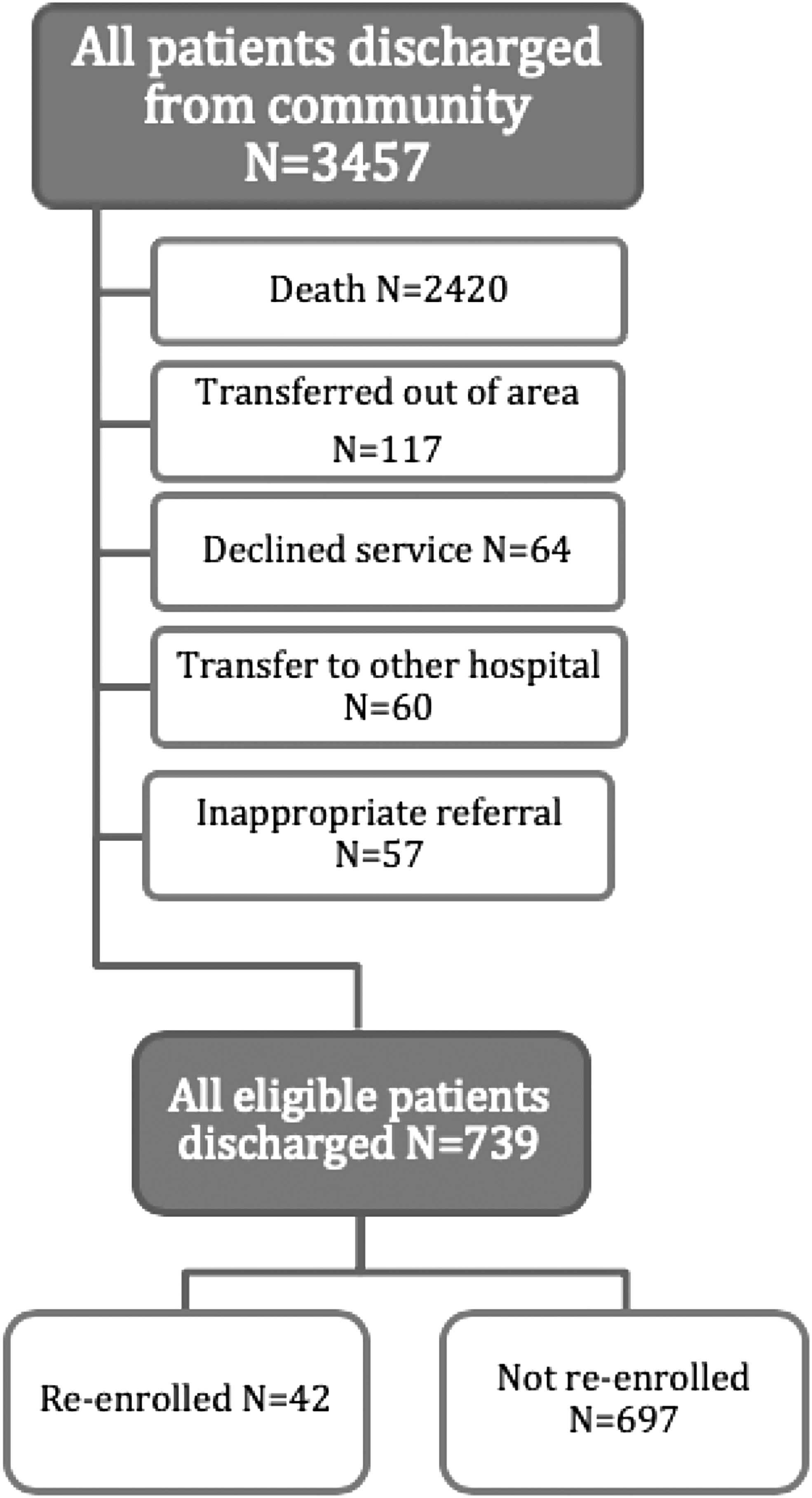
Flowchart showing inclusion of eligible patients.
“Admission 1” refers to the timeframe between initial enrollment and discharge, whereas “Admission 2” refers to the timeframe between re-enrollment and re-discharge. The “Discharge period” refers to the timeframe between discharge and re-enrollment. Patients who were not re-enrolled would not have a second admission.
The following data were extracted: sociodemographics (age, gender, living situation-living alone, living with others, RACF, or unknown), duration of Admission 1, and diagnosis (malignant vs. nonmalignant). Patients were dichotomized into two groups of more than or less than 65 days for the duration of Admission 1, which was the overall median duration of care.
For patients with more than two admissions into the community service, the assessed admission was the penultimate admission. It was thought to be the likely period of care to be most representative of the patients' issues, as they generally deteriorate with each subsequent admission, requiring more assistance from the SHCPCS.
Tools
Currently, there are no validated discharge criteria for palliative care services. We have modified the referral criteria developed by Hui et al. (2016) to assess the reasons for re-enrollment. 11 The referral criteria identify patients who should be reviewed by palliative care services, whereas the converse could be interpreted as patients who do not need review by palliative care services. For example, in Hui's study, a major criterion for referral to the palliative care outpatient team was unstable physical and emotional symptoms. 11 Conversely, in the version we have modified, a patient must have stable physical and emotional symptoms to be discharged. The original discharge criteria were developed for cancer patients, therefore the cancer-specific discharge criteria were excluded for nonmalignant cases. In our study, if patients met all the discharge criteria, we deemed them to be appropriately discharged.
Statistical analyses
Descriptive statistics were used to summarize demographic data. Univariate analysis was conducted. Categorical variables were assessed with the chi-square test to compare groups. To determine factors associated with re-enrollment, binary logistic regression analysis was performed with age, gender, living situation, length of episode of care, and diagnosis (malignant vs. nonmalignant) as independent variables. To account for missing data from “unknown living situation,” complete case analysis was used. Analysis was performed by using the Statistics Package for Social Sciences (SPSS Version 21; SPSS, Inc., Chicago, IL).
Ethics
Ethical approval was granted by St Vincent's Hospital (Sydney) Human Research Ethics Committee on June 26, 2017 (reference LNR/16/SVH/346).
Results
Patterns of re-enrollments to the service
Of the 3457 patients discharged from the SHCPCS, 739 (17.4%) patients were eligible for inclusion in the analysis and 42 (5.7%) patients had been re-enrolled in the service (Fig. 1). Among those who re-enrolled, eight patients (19%) had more than two admissions into the community palliative care service. Of those, six patients had three admissions whereas two patients had four admissions. Patient characteristics are summarized in Table 1. Among the re-enrolled patients, the most common malignant diagnoses were breast and lung cancer. The most common nonmalignant diagnosis was neurological disorder (Appendix Table A1). Although the median discharge period was 216 days, the distribution of the discharge periods was as follows: 0–30 days for 6 (14%) patients, 31–60 days for 3 (7%) patients, 61–90 days for 1 (2%) patient, 91–120 days for 6 (14%) patients, 121–150 days for 3 (7%) patients, and greater than 150 days for 23 patients (55%). The most common reasons for re-enrollment were physical symptoms (n = 34, 81%), emotional symptoms (n = 13, 31%), assistance with decision making and care planning (n = 6, 14%), delirium (n = 4, 10%), brain or leptomeningeal metastases (n = 2, 5%), diagnosis of advanced malignancy with progressive disease despite second-line systemic therapy (n = 2, 5%), patient requests (n = 2, 5%), and other reasons (n = 4, 10%).
Characteristics of Discharged Patients
Factors associated with re-enrollment
In the univariate analysis, the factors that were predictive of re-enrollment were gender (p = 0.04) and living situation (p < 0.01) (Table 1). In the multivariate analysis, the patients' living situation remained a significant predictive factor for re-enrollment. Patients from aged care facilities (OR = 3.45; 95% CI 1.28–9.28; p = 0.01) were more likely to be re-enrolled. A malignant diagnosis was also associated with an increased chance of re-enrollment (OR = 2.22; 95% CI 1.00–4.93; p = 0.04). Gender (p = 0.09), age (p = 0.46), and duration of admission 1 (p = 0.2) were not significant factors. For the majority of re-enrolled patients, the reasons for discharge from the initial admission were that they were in a stable condition (n = 29, 69%) and had no ongoing specialist palliative care needs (n = 27, 64%). A small number of patients or family declined further contact (n = 7, 17%) or were not contactable for more than three months (n = 4, 10%). Two patients (5%) were referred to other hospice services. Only a minority of patients were discharged inappropriately according to the adapted discharge criteria (Table 2). 11
Discharges According to the Adapted Discharge Criteria
Discussion
This study of 3457 patients describes the pattern of re-enrollment of previously discharged patients from a community palliative care service over a five-year period. Only small numbers of patients were re-enrolled (5.7%) in the service and the majority were re-enrolled only after a reasonable period (>150 days).
There are variations in discharge practices and processes of patients across palliative care services. Some services discharge patients at the earliest opportunity, that is, when patients are stable; whereas other services keep patients enrolled and intervene only when required. In a study conducted in the United Kingdom by Newbury et al., 9 patients were discharged only if the local discharge criteria were fulfilled. The criteria used were as follows: (1) The initial objectives at the time of the referral have been met; (2) there is no longer a need for specialist intervention but re-enrollment is welcomed; (3) the patient and carer have declined any further specialist input; and (4) the general practitioner is aware of the discharge. These criteria were based on general guidelines and not validated. In addition, nursing staff frequently emphasized to the patient and their carers that re-enrollments were welcome as the need arose.
Despite a long follow-up period of five years, the number of re-enrolled patients in our study was small at 5.7%. In comparison, 11.6% of patients were re-enrolled over a six-month period in the study by Newbury et al. 9 and 17.8% over two years in the study by Bull et al. 10 Our service also had a longer initial admission of 146.6 days compared with 86 and 55.9 days in the other studies, respectively. The potential reasons for a lower re-enrolment rate could be related to a less proactive discharge screening process or because patients were carefully selected for discharge. The longer duration of the initial admission may be explained by the lack of a formalized approach for patient discharges or a higher proportion of patients with complex needs requiring ongoing specialist palliative care support. There are currently no international or national consensus or benchmarks for discharging patients, making it unclear whether our discharge processes are acceptable, or whether they are comparable to other institutions.
The majority (55%) of patients in our study were re-enrolled after more than 150 days following their initial discharge. In comparison, 39% of patients in the study by Newbury et al. were re-enrolled in this timeframe. Ideally, when patients are selected appropriately for discharge, they are expected to have a period of stability in their condition. Therefore, there should be a longer “discharge period” even if they were re-enrolled later on. If patients were re-enrolled shortly after discharge, they may been inappropriately selected for discharge as they have ongoing specialist palliative care needs. With a systematic approach, patients can be regularly reviewed and discharged if they remain in a stable phase.
Living in an RACF was found to be a significant predictive factor for re-enrollment. Patients living in RACFs have variable prognosis, with many patients suffering from chronic illnesses with multiple co-morbidities.12,13 Patients may be re-enrolled due to symptoms related to acute exacerbations of their illnesses and discharged when the reasons for referral had been addressed.
As the number of deaths in RACFs increases, 14 RACFs are transforming into an end-of-life care service. 15 There is an urgent clinical need for improving access to palliative care to patients in RACFs and education for RACF staff. Staff in RACFs have variable training and may lack familiarity with the principles of palliative care; this may affect their confidence in looking after patients with life-limiting illnesses.16–18 In an Australian pilot study, Chapman et al. reviewed how the integration of a specialist palliative care service may impact residents, relatives, and staff in RACFs. 12 The model involved a palliative care nurse practitioner leading “Palliative Care Needs Rounds” to support clinical decision making, education, and training in four RACFs. The study demonstrated a reduction in length of hospital stays and a lower death rate in the acute care setting. This model could have a substantial impact on service development and resource allocation to address the palliative care needs of those patients.
Interestingly, patients living alone at home were not found to be a significant predictive factor for re-enrollment. Patients who lived alone may be more inclined to present to an acute hospital setting if they require medical review, rather than requesting re-enrollment to the community palliative care service.
About 70% of patients in this cohort have a malignant diagnosis. This proportion is consistent with what is seen nationally in Australian specialist palliative care services. 19 A malignant diagnosis was also found to be a predictive factor in multivariate analysis. As the number of cases was small, the impact of different tumor streams on re-enrollment was not assessed. Some prognostic factors that should be taken into consideration before discharge include brain or leptomeningeal metastases, where patients are at increased risk of being re-enrolled due to the likelihood of rapid deterioration and ongoing symptoms. Not only do these patients have poorer prognosis, but there are also associated psychosocial implications. These events often herald the beginning of progressive functional decline and are associated with psychological and carer distress.20,21 Gender was also a significant predictive factor in univariate but not multivariate analysis. This is likely to be due to the disproportionate number of female residents in RACFs in this study, which acted as a confounding factor.
As there are currently no standardized discharge criteria from a community palliative care service that have been published or validated, we modified referral criteria developed by Hui et al. to determine whether patients were appropriately discharged from the service. 11 Although this intuitively seems logical, we note that other factors may contribute to the consideration of discharging patients. These factors may include patients who may have been enrolled in error, patients who do not have a serious illness, patients with no active symptoms or complications from chronic conditions or serious illness, no hospital admissions or emergency department visits in the previous six months, patients who are not home bound, and patients who have access and transportation to other health services including primary care services. In this study using the modified criteria, the majority of patients were discharged appropriately. A quarter of the patients declined further input, or they were not contactable on discharge, including patients with unstable symptoms. Although it is not ideal to discharge patients with unstable symptoms, a patient's autonomy must be respected. It is encouraging that patients and their care providers were aware of the processes of re-enrollment and patients were accepting re-enrollment as their condition changed.
Of note, our adapted discharge criteria were designed for the assessment of cancer patients. Therefore, some of the cancer-specific criteria were not applicable to the nonmalignant cases in this study. Due to the comprehensive nature of the criteria, the use of the discharge criteria would require input from a multidisciplinary team rather than individual judgment.
This study has a number of limitations. As it was a retrospective study, only previously recorded data were available for extraction. A prospective study may include data on caregiver assessments, access to reliable primary health care services, avoidable hospital admissions, and emergency department presentations. As a single site study from 2010 to 2016, there was only a small sample size of 42 re-enrolled patients. This study, however, started with about 3500 patients who were discharged, and it has a substantial study timeframe of five years. This study did not compare the outcomes of re-enrolled patients with those who were not re-enrolled, as the outcomes of patients who were not re-enrolled to the community palliative care service were not available for comparison. As the patients have been discharged from the service, it would have been inappropriate to call patients' families or general practitioners to follow up on these patients. Lastly, with a growing nonmalignant population with increasing frailty, the findings may be less generalizable to a broader population given the high proportion of cancer patients in this study.
Future areas of research include the development and validation of discharge criteria for community palliative care services that could also be implemented by other services. It is essential to collaborate with other palliative care services to establish best practice guidelines and to develop a more systematic approach to the discharge of patients. In addition, research infrastructure that has the ability to track patients who are discharged from the community palliative care service will paint a clearer picture of the outcomes of patients who may have been discharged prematurely or inappropriately. More research is being done in this area by our group.
Conclusion
Community palliative care service is a limited resource. Identifying appropriate patients for discharge will optimize resource use and improve the efficiency of the service delivery. In this study, patients had a low re-enrollment rate, and they had remained under the community palliative care service for a comparatively long period, which is possibly reflective of a highly selective discharge process or an inadequate discharge process. This study has highlighted the potential factors contributing to re-enrollment, which were increased for patients living in RACFs and those with malignant diagnoses. Additional resources and education to staff in RACFs may improve outcomes for patients, and decrease re-enrollments to the community palliative care service. Further studies should evaluate the impact of other patient and disease factors to assist in the implementation of effective discharge processes.
Footnotes
Funding Information
No funding was received for this project.
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Diagnoses of Patients Discharged from the Community Palliative Care Service Included in Final Analysis
| Diagnosis | Re-enrolled, n (%) N = 42 | Not re-enrolled, n (%) N = 697 |
|---|---|---|
| Malignant diagnosis | 30 (71.4) | 480 (68.9) |
| Breast | 7 (16.7) | 41 (5.9) |
| Lung | 6 (14.3) | 106 (15.2) |
| Urological | 3 (7.1) | 49 (7.0) |
| Colorectal | 3 (7.1) | 57 (8.2) |
| Hematological | 3 (7.1) | 33 (4.7) |
| Gynecological | 2 (4.8) | 29 (4.2) |
| Upper GI | 2 (4.8) | 81 (11.6) |
| CNS | 1 (2.4) | 19 (2.7) |
| Head and neck | 0 (0) | 18 (2.6) |
| Unknown primary | 1 (2.4) | 24 (3.4) |
| Others | 2 (4.8) | 23 (3.3) |
| Nonmalignant diagnosis | 12 (28.6) | 217 (31.1) |
| Neurological disorder | 9 (21.4) | 72 (10.3) |
| Cardiovascular | 2 (4.8) | 40 (5.7) |
| Respiratory | 1 (2.4) | 52 (7.5) |
| Renal | 0 (0) | 13 (1.9) |
| Others | 0 (0) | 40 (5.7) |
CNS, central nervous system; Upper GI, upper gastrointestinal tract.