
Abstract
Background:
Fluid management is a clinical challenge in patients with end-stage renal disease (ESRD), especially among those who opted for conservative treatment. We initiated a comprehensive program of psychosocial interventions.
Objectives:
To study the impact of this psychoeducational (Appropriate amount of intake, Self-efficacy, and Adherence [ASA]) program on symptom burden and acute admission rates related to fluid overload (FO) in this group of elderly ESRD patients attending renal palliative care outpatient clinic under our division.
Methods:
All elderly (age >60 years) patients who were followed in our renal palliative clinic had one or more acute admissions related to FO during the first three months were identified and invited to participate in this program. The palliative care nurse assessed each pair of patient/caregiver before doctor consultation, documented the symptom burden by the Edmonton Symptom Assessment Scale, provided symptom advice with use of pamphlets, monitored fluid and drug compliance, and provided psychosocial–spiritual support. The patient symptom score, body weight (BW), and three month acute admission episodes were compared before and after psychoeducation interventions by paired t test.
Results:
Data from 138 patients were analyzed. Of them, edema, shortness of breath, and insomnia occurred in 131 (95%), 67 (49 %), and 44 (32%) patients, respectively. A total of 125 patients (90.6%) had poor fluid/diet compliance, whereas 59 patients (42.7%) had poor drug compliance. The BW decreased significantly from 57.1 (12.8) kg at baseline to 52.5 (13.6) kg after three months of the ASA program. The acute admission rate related to FO dropped significantly from 7.6 episodes/patient/year to 6.4 episodes/patient/year.
Conclusion:
Our data demonstrated that the ASA program could improve patient symptoms and reduce acute hospital admissions, and thus improve the overall patient wellbeing and reduce health care utilization. Further studies are required to delineate the efficacy of different components in this ASA program and how to enhance its delivery.
Introduction
Fluid management is a clinical challenge in patients with end-stage renal disease (ESRD),1,2 especially among those who opted for conservative treatment. In this context, adherence to fluid restriction is integral to preventing fluid overload (FO). Dyspnea is often the first symptom experienced by ESRD patients who choose conservative care; the sensation of dyspnea is sometimes also exacerbated by worsening acid imbalance. Factors that influence fluid intake and restriction include sensation of thirst, consumption of food with high water content, use of water to facilitate intake of medications, and patients' wish and ability to adopt appropriate strategies for fluid management.3–5
Previous studies showed that limiting one's fluid intake is a psychological and behavioral challenge as the individual has to deal with the learned and/or the physiological urge to drink and at the same time manage the necessary health-related restraints on drinking. 6 Educational components including diet (i.e., low salt) and fluid intake advice combined with a variety of psychological techniques have been used in assisting ESRD patients to develop healthy behaviors, reduce nonhealthy behaviors, and relieve emotional distress. 6 Self-efficacy is widely used as a theoretical concept 7 and to understand health behavior and facilitate behavioral change. Adherence to self-care behaviors in ESRD is generally low. 8 Many patients with ESRD opted for conservative treatment are elderly and so may have impaired cognitive function. This makes learning new self-care skills problematic. 9
In Hong Kong, all patients who reach Stage 5 chronic kidney disease (CKD) were interviewed by nephrologists, and the options of renal replacement therapy (dialysis or renal transplantation) versus conservative management were discussed; ∼20% of patients chose the latter option. Patients who opt for conservative management in our region were referred to the renal palliative care clinic, which is an integrated clinic jointly run by renal and palliative care physicians. Our collaborative renal palliative care (CRPC) program commenced since 2011 encountered significant default rates up to 30–50% (i.e., number of schedule visits not attended divided by the total number of scheduled visits), which were largely because of readmissions related to FO. 10 Indeed, previous studies have suggested that insufficient knowledge on the appropriate fluid intake contributes to FO. 11 Furthermore, self-efficacy and adherence to self-care behaviors can facilitate behavioral changes,12,13 and hence potentially improve fluid management in ESRD patients who opted not for dialysis. Therefore to further improve our CRPC program, we initiated a comprehensive program of psychosocial interventions, and here the brief report retrospectively reviewed and evaluated the impact of this comprehensive program on acute admission rate and symptom burden.
Methods
All elderly (age >60 years) 14 patients followed-up in our renal palliative clinic who had one or more acute admissions related to FO during the first three months were identified and invited to participate in this program. Inclusion criteria were as follows: (1) CKD stage 5 according to the Kidney Disease Outcome Quality Initiative (K/DOQI) Guidelines 15 ; (2) referral criteria appropriate for gold standard framework 16 ; and (3) mentally competent (defined as subjects who have the mental ability to choose between right and wrong and also the ability to express themselves, and were determined by the attending physicians). Patients who have their mental competence in doubt were referred to occupational therapist or psychiatrist for formal assessment. Elderly patients with evidence of dementia were properly assessed for their mental competence before recruitment into the program.
Comprehensive psychoeducation interventions
Our psychoeducation program focused on Appropriate amount of intake, Self-efficacy, and Adherence (ASA), with the aim to improve elderly patient's knowledge and adherence to self-care behaviors and reduce health care utilization by continuous monitoring of their symptoms. Education provided by palliative care (PC) nurse emphasized on both salt and fluid intake. The nurse was coached by a dietician and was in continuous dialog with the dietician about nutritional problems. Patients were advised to limit sodium intake to 2–3 g/day (corresponding to 5 g of salt per day) and fluid intake to a maximum of 1.5 L/day. Pamphlets with relevant information were also provided to patients and their caregivers.
Interventions
A social–cognitive framework 17 that addressed beliefs, behaviors, emotions, and physical feelings was used to elicit and assess the relative contribution of self-reported factors influencing thirst and drinking. Each patient was offered up to four to five treatment sessions and an additional booster session. Standard dietetic advice regarding sodium intake was given during the intervention period. Standard advice for managing thirst was also discussed. This included established strategies, such as limiting salt intake, using ice chips, measuring daily allotment of fluid, performing mouth care, eating raw or frozen fruits and vegetables, sucking on hard candy, and to chew gum. 18 Thus, self-regulation strategies included preplanning, substitution, dietary modification, situational control, distraction, and record keeping to reduce fluid intake. 19
An initial criterion of successful self-regulation was introduced in concordance with the participant. Thus, individual patient preferences/patient-reported values around symptom burden were assessed and then used to determine the “intervention.” As the participant successfully reached the preset performance level, the goal was gradually set to a more strict level of fluid intake. Thus, the step-by-step change of the criterion was individualized and the number of increments thereby varied between the subjects. 20 Moreover, each of these steps could be regarded as intermediate goals in the process of excessive fluid overload reduction. During the intervention phase, subsequent body weight (BW) measurements were recorded for patients as feedback.
The number of sessions was adjusted according to each participant's requirements. The individualized analysis was used to identify problems of individual patients and to derive a treatment based on given prerequisites. This made it possible to identify reinforcements and cues linked to fluid intake behavior, that is, to provide a profile of situation-specific fluid intake behavior and personal circumstances for fluid intake, and elicit relevant dietetic and psychosocial factors. An example of personal approach was an elderly ESRD lady presented with worsening symptoms related to excessive watermelon consumption causing FO and hyperkalemia. On review of her diet records, we found out that she had consumed 200 mL watermelon juice and 8–10 scoops of watermelon every day. After counseling, she agreed to reduce the juice and scoops amount by one-third initially and further reduction based on her response. Her symptoms gradually improved after regular monitoring at home and review in clinic. 21
In this ASA program, both patients and their main family caregivers received education, counseling, and intervention from on-site PC nurse in clinic. Fluid advice and FO prevention were reinforced through psychocognitive approach and improvement in “self-efficacy” because ESRD patients usually had difficult in fluid restriction and lack of clear instructions in self-monitoring of fluid status.
In each ASA session, the PC nurse assessed each pair of patient/caregiver before doctor consultation. The patient symptom burden was self-reported by using the Edmonton Symptom Assessment Scale (ESAS). 22 The detailed components of “ASA” are given in Figure 1. The patient home blood pressure and BW record were reviewed. The disease status and the importance of fluid control were also explained to the caregivers in the clinic session. The caregivers were reminded to monitor the patients' fluid compliance by means of weight measurement and diary for food/fluid intake.
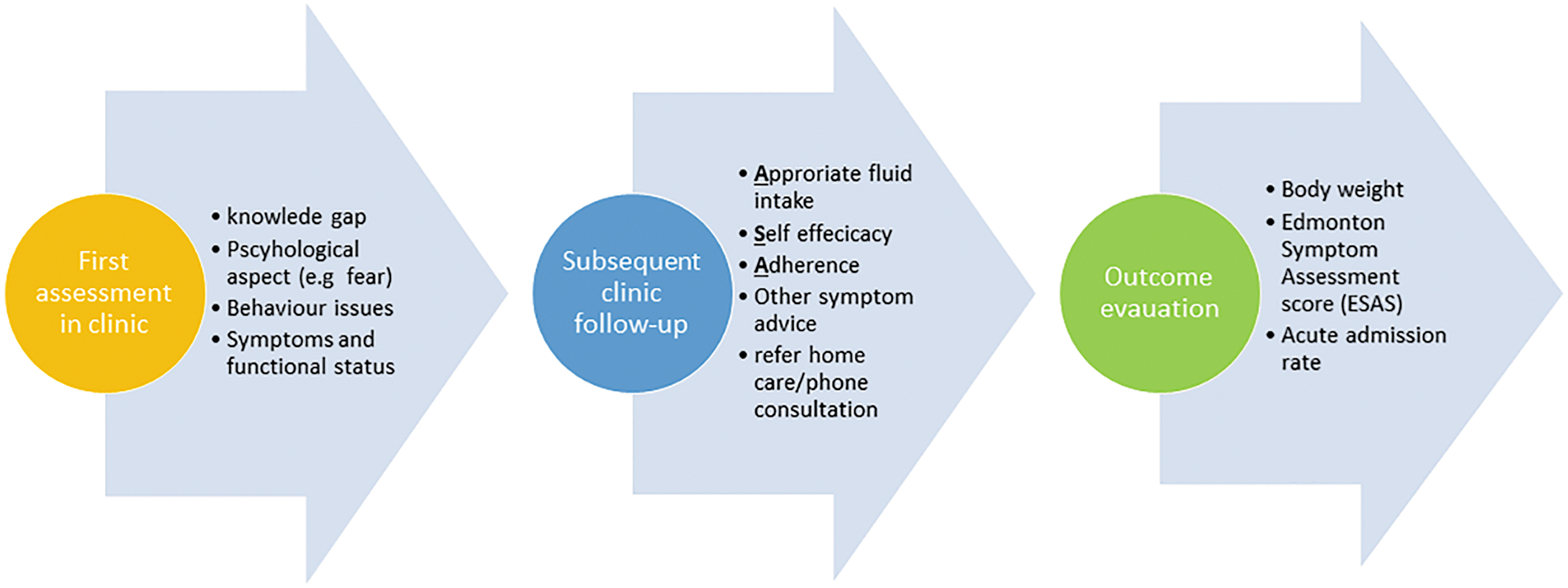
Components of ASA program. ASA, Appropriate amount of intake, Self-efficacy, and Adherence. Color image is available online.
All patients' symptoms and psychosocial problems were reported to the corresponding clinician to facilitate better communication among team members. The use of diuretics for these patients was decided by the attending clinicians. Diuretics were prescribed or escalated if the BW was ≥1.5 kg or 5% increase in BW for those light-weight patients (e.g., BW ≤45 kg). 23 Patients with poor treatment compliance or significant FO were admitted for further management.
Follow-up and monitoring schedules
Patients recruited into this ASA program were followed up in two- to four-week intervals. The symptomatology, amount of fluid intake, BW, and blood pressure were monitored during each clinic attendance and home care visit. Patients with poor insight or treatment response were referred for further counseling, frequent home visit, or even admission.
Outcome measures and statistical analyses
Primary outcome was defined as absence of any readmission related to FO within three months after the ASA. Secondary outcomes include change in symptoms scores, BW, and changes in diuretics. Clinical data were retrieved from the hospital Computer Management System and all diagnoses were according to the International Classification of Diseases, 9th Revision, Clinical Modification codes (congestive heart failure [CHF] was denoted as 428.X). Continuous variables were expressed as mean (standard deviation) or median (range) and analyzed with t test (paired or unpaired), Mann–Whitney test, or analysis of variance where appropriate. Categorical variables were expressed as frequencies (percentages) and analyzed with chi-square test or Fisher's exact test where appropriate. The patient symptom score, BW, and three-month acute admission episodes were compared before and after psychoeducation interventions by paired t test. A Pearson correlation analysis was performed to determine if the number of acute admissions was influenced by patients' demographical and clinical factors. Multivariate logistic regression analysis was performed to identify independent factors associated with readmissions (related to FO) three months after ASA program. Age, sex, and variables with p < 0.1 on univariate analysis were included in the multivariate analysis. All analyses were performed by the SPSS statistical package 22.0 (SPSS, Inc., Chicago, IL) and p < 0.05 were considered statistically significant.
Results
Patient characteristics
A total of 243 patients were identified to join the ASA program during the period of January 2014 to October 2017. A total of 138 (57%) patients agreed to participate in this program (Table 1). The reasons for those who declined the program were owing to transport or financial problem. Approximately half the patients in this ASA program had history of CHF. Forty-one patients (63%) had echocardiogram performed, in which 32 (78%) showed an ejection fraction of <40%. Eleven (8.0%) patients were lost to follow-up. Edema, shortness of breath, and insomnia occurred in 131 (95%), 67 (49%), and 44 (32%) patients, respectively. A total of 125 patients (90.6%) had poor fluid/diet compliance, whereas 59 patients (42.7%) had poor drug compliance. Fifty-one patients (37%) also had concomitant hyperkalemia and/or hyperphosphatemia. All patient required diuretics (either loop diuretics [72.6%] or loop diuretics plus thiazide [27.4%]) before joining the ASA program. The median daily dose of frusemide was 80 mg (20–160 mg), whereas the median daily dose of metolazone was 5 mg (2.5–10 mg).
Demographic and Laboratory Data of Renal Palliative Clinic Patients with Acute Admission Related to Fluid Overload (N = 138)
PPS = Palliative Performance Score 0–100% with 11 categories (0% = dead, ≥70% = independent; 100% = totally independent).
CHF, congestive heart failure; SD, standard deviation.
Impact on patient outcomes
There were 485 acute admissions and 289 (59%) of them were related to FO before starting the program. After three months, the acute admission rate related to FO dropped significantly from 7.6 episodes/patient/year to 6.4 episodes/patient/year (p < 0.05) (Fig. 2). In total, 92 (67%) had home care visit and 14 (10%) palliative ward admission for fluid management. After three months, 36 patients (26%) required escalation of diuretics dosage (the median dose increase was 40 and 5 mg for frusemide and metalozone, respectively). Thirteen patients (9.4%) had reduction in diuretics (the median dose decrease was 2.5 mg for metalozone). The median survival time for this cohort was 9.8 months.

Changes of ESAS symptom score and acute admission rate after ASA program. ESAS, Edmonton Symptom Assessment Scale. Color image is available online.
Predictors for readmission owing to FO after ASA program
Multivariate analysis demonstrated that only the presence of CHF was an independent risk factor for hospital readmissions owing to FO (odds ratio = 2.21, 95% confidence interval = 1.08–4.20, p = 0.022) after ASA program (Table 2).
Univariate and Multivariate Analysis for Appropriate Amount of Intake, Self-Efficacy, and Adherence Program Response
No response = 1; response = 0. Those statistically significant correlates (i.e., p < 0.1) in univariate analysis will then be put into the multivariate analysis. Significant predictor will be defined if p < 0.05 after multivariate analysis.
p < 0.1 in univariate analysis.
p < 0.05 in multivariate analysis.
CI, confidence interval; CrCl, creatinine clearance; Hb, hemoglobin level; OR, odds ratio; PPS, Palliative Performance scale; SOB, shortness of breath.
Changes in symptoms scores and BW after ASA program
The mean ESAS scores of edema decreased significantly from 3.4 (1.7) to 1.7 (1.2) after three months (p = 0.027). Other symptom scores (mean) on shortness of breath, sleep, and wellbeing also decreased from 3.6 to 3.3, 2.3 to 2.1, and 1.8 to 1.5 after three months, respectively, although not reaching statistical significance (p > 0.05). The changes of ESAS symptom item scores are given in Figure 2. The BW decreased significantly from 57.1 (12.8) kg at baseline to 52.5 (13.6) kg after three months of the ASA program (p = 0.017).
Discussion
Our results suggest that the ASA program can significantly reduce morbidity and acute hospitalization owing to FO in renal palliative patients. In this context, the ASA program shows benefit in improving BW, severity of edema, shortness of breath, sleep, and overall wellbeing of ESRD patients who opt not for dialysis. The current guidelines have included patient education on self-care themes for FO as nonpharmacological means to decrease new onset of symptoms of FO and hospital readmissions. 24 Although weight monitoring, low sodium diet, and fluid restriction classic self-care behavior themes were related to fluid management, 15 education strategies that promote self-care behaviors were not consistently employed. One key element of our ASA program is to educate elderly patients with ESRD, to decrease fluid excessive intake, and to have balanced diet control at home, assisted by family and home care nurse visit. Indeed, previous studies in advanced heart failure patients have indicated that revising the methods of delivery of elderly patient education might improve patient's knowledge and adherence to self-care behaviors and thus reduced health care utilizations such as unscheduled hospital admissions. 25 The effectiveness of our ASA was also reflected by the fact that only 26% of patients required escalation of diuretics treatment and almost 10% even needed dosage reduction. Moreover, only 10% of patients required clinical admission to palliative ward to manage FO problems. Of importance, our present findings indicated that the ASA program with comprehensive psychoeducation interventions could significantly minimize acute hospital admissions related to FO. Nevertheless, multivariate analysis data suggested that the presence of CHF remained independent risk factor for readmissions in ESRD patients who opted not for dialysis.
There are several limitations to this study. We recruited all elderly ESRD patients with symptoms related to fluid edema but did not analyze patients according to other demographics factors or comorbidities. Moreover, it is difficult to confirm whether all nonpharmacologic interventions were required to achieve favorable outcomes or only some interventions were more effective. It is unknown if there are any correlations among the number of types of nonpharmacologic interventions used and the outcome on FOs. In addition, it is difficult to ascertain whether the reduction of BW was the result of the ASA program because weight for patients having multiple admissions is known to decrease and could be contributed by uremic symptoms such as anorexia and nausea at the end of life. Here we did not assess thirst symptoms, preintervention self-efficacy, adverse effects of fluid restriction on blood urea, quality of life or survival and patient satisfaction, and this remained important limitations of our study. Although patients who declined the ASA program could serve as a good control group, these subjects have problems with frequent follow-ups and sometimes even default and thus it was difficult to compare their data with the intervention group.
National registry data demonstrated that many ESRD patients continue to have difficulties in managing their fluid restriction and the necessity of controlling the fluid intake incurred substantial treatment-related stress.26,27 To overcome these hurdles, our ASA program were tailormade to the psychosocial needs of patients 28 and aim at reducing the amount of fluid intake gradually, making the program more acceptable to elderly patients. Indeed, the percentage of patients with poor compliance to fluid intake was significantly decreased after the implementation of the ASA program (13% after implementation, compared with 91% before implementation). Other important features that contributed to the success of our ASA program included (1) early proactive model to reduce overload; (2) on-site education and counseling for patients and caregivers, and importance of psychoeducational interventions relieving FOs; and (3) use of simple assessment and referral criteria in our program.
Conclusion
Taken together, our data demonstrated that the ASA program could improve patient symptoms and reduce acute hospital admissions, and thus improve the overall patient wellbeing and reduce health care utilization. Notwithstanding, one should appreciate that this ASA program comprises different components and it remains difficult to discern which element in the ASA program is more effective. Further studies are required to delineate the efficacy of different components in ASA program and how to enhance delivery of this program to patients and their caregivers. It is foreseeable that as our patient demographics become older and frailer, an ASA program with elements of patient psychoeducation and multidisciplinary inputs will serve to improve the overall wellbeing of ESRD patients who opt for conservative management and the health care burdens.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.