
Abstract
Background:
It remains unclear whether the end-of-life (EOL) treatment/environment impacts on survival after anticancer treatment in terminally ill women with ovarian carcinoma (OC).
Objective:
The aim of this investigation was to clarify how long those women actually survived after their last anticancer treatments and their hallmarks.
Setting, Design, and Measurements:
Between 2003 and 2011, 79 terminally ill women with OC were retrospectively analyzed as a single institutional study. Postcancer treatment survival (PCS), defined as the duration between the last date of the abovementioned “cancer treatment” and that of death from any cause, was analyzed on stratification by type of supportive care or where patients spend their EOL. Inverse probability of treatment weighting (IPTW)—adjusted Kaplan–Meier and Cox regression analyses were employed to compare PCS between the two groups.
Results:
The median PCS of patients was 10.8 weeks. In the multivariable analysis, the performance status and EOL place retained their significance as independent prognostic factors of poorer PCS (performance status [2–3/0–1]: hazard ratio [HR] = 3.279 [95% confidence interval; CI 1.967–5.586; p < 0.0001], EOL place [hospital/home hospice]: HR = 0.574 [95% CI 0.355–0.913; p = 0.0188]). In the IPTW-adjusted cohort, the median PCS rates were 15.0 and 9.7 weeks in patients of home/hospice and hospital groups, respectively (p = 0.04). Also in the IPTW cohort, the EOL place retained its significance (IPTW-adjusted: HR [95% CI]: 1.548 [1.009–2.374], p = 0.045, multivariable adjusted with IPTW: HR [95% CI]: 1.670 [1.077–2.588], p = 0.022).
Conclusion:
Our current data may be hypothesis generating; it is possible that the EOL environment is a crucial prognostic factor for survival after anticancer treatment.
Introduction
Ovarian carcinoma (OC) is one of the most aggressive malignancies of the female genital tract worldwide, with >238,700 newly diagnosed cases and 151,900 reported deaths per year. 1 OC is also known as a “silent killer” since the majority of women with OC are generally asymptomatic until disease progression throughout the peritoneal cavity. 2 Owing to the established therapeutic strategy including maximum cytoreductive surgery and systematic chemotherapy, in approximately four out of every five women, complete clinical remission can be achieved. Nevertheless, in up to three out of every four women who achieve a complete response, recurrence eventually develops despite a transiently favorable prognosis. 3 Once patients experience recurrence, they enter a new clinical phase that is extremely different from the phase of remission–induction treatment. After recurrence, they must endure treatment-related toxic adverse events, fear for their life, anxiety, and various undesirable symptoms. Thus, palliative medicine is frequently coadministered with aggressive cancer-related treatment.4,5
In general, patients with OC tend to receive aggressive anticancer treatments near the end of life (EOL) or in the terminal stage. 6 Chemotherapy at the EOL is a complex and controversial issue in clinical practice of OC as well as other malignancies. We should recognize that patients with OC show heterogeneous oncologic stage in relation to disease progression. Especially, it is critical for physicians to balance between chemoeffectiveness and its related cytotoxicity at near EOL stage. Excessive cure-oriented therapies at the EOL may cause various issues, such as enormous financial strain, unfavorable side effects, and the waste of precious time, whereas it does not necessarily improve survival. However, it remains unclear whether the EOL treatment/environment impacts on subsequent survival after anticancer treatment in terminally ill women with OC. Accordingly, here, we investigated a cohort of 79 patients with OC at the EOL stage. The aim of the present investigation was to clarify how long those women actually survived after their last anticancer treatments and the hallmarks of EOL treatment and the associated environment.
Patients and Methods
Patient cohort
Between 2003 and 2011, a total of 79 terminally ill patients with OC were accumulated by Nagoya University Hospital (NUH). Patients were eligible if they fulfilled the following: (1) terminally ill patient with OC who consequently died of the disease, (2) had sufficient clinical data, including the details of the last anticancer treatment and oncologic outcome, and (3) had information on the EOL status, supportive treatment/care, Eastern Cooperative Oncology Group (ECOG) performance status, maximum opioid use, and place where they spent their EOL. Data were collected from clinical follow-up visits, medical records, telephone inquiries, and/or written reports from referral institutions. This study was approved by the ethics committee of Nagoya University. The clinical stage was assigned according to the International Federation of Gynecology and Obstetrics (FIGO). The histological cell types were assigned according to the criteria of the World Health Organization (WHO) staging system. 7 The treatments of OC were generally based on criteria described previously.8,9 Maximum opioid intake was calculated as the oral morphine use. 10 The ratio of each equianalgesic dose to oral morphine intake per 24-hour opioid was calculated as follows: transdermal fentanyl (1:30), morphine suppository (40:60), modified-release oxycodone (20:30), parenteral morphine (1:2), and parenteral fentanyl (0.6:60). 10 Regarding where patients spent their EOL, we divided all patients into four cohorts: university hospital, general hospital, hospice, and home care groups. The university hospital cohort included patients who continuously received anticancer therapy and subsequent palliative care from initial treatment until death in NUH. Each general hospital, hospice, or home care cohort included those who had received primary therapy in NUH and thereafter were referred/moved to a neighboring general hospital, hospice, or home care, respectively. General hospital was defined as a regional hospital without specific palliative care unit. In an EOL counseling session, the cessation of the anticancer treatment and final EOL place were decided reflecting patient/family's hope.
Survival analysis
In this study, “anticancer treatment” was defined as initial cytoreductive/subsequent salvage surgery, and/or chemotherapy, and/or radiotherapy excluding aiming for palliative irradiation. Also, postcancer treatment survival (PCS) was defined as the duration between the last date of the abovementioned “anticancer treatment” and that of death from any cause.
To balance the patient and tumor characteristics between the two groups, propensity score (PS) matching/weighting was performed. 11 PS was estimated by multivariate logistic regression models for the probability of the EOL place (hospital vs. home/hospice) adjusting for the age, histological type (high-grade serous carcinoma [HGSC] vs. non-HGSC), ECOG performance status (0–1 vs. 2–3), maximum opioid intake (<25 mg vs. ≥25 mg), and frequent thoracentesis/paracentesis (yes vs. no). In this study, the statistical methodology of inverse probability of treatment weighting (IPTW) was used for better adjustment for measurable and unmeasurable confounders to minimize any selection bias. 12 Using this method, each patient was weighted by the inverse probability of being in the hospital versus home/hospice group, aiming to balance observed characteristics between the two cohorts.
Within the original (unweighted) and weighted cohorts, survival curves were generated using Kaplan–Meier methods. A Cox proportional hazards regression model was employed to examine multivariable analyses. The distributions of clinicopathologic events were evaluated using the chi-square test. Differences in survival curves were compared using the log-rank test. p < 0.05 was considered significant.
Results
Patients' characteristics
In total, 79 patients terminally ill with OC were identified for the current analysis (Table 1). The median follow-up length of all women was 29.1 (1.0–196.6) months. The median (range) age at the time of final anticancer treatment was 56 (27–80) years. Regarding the distribution of the histological type, 30 (38.0%) women had HGSC and 49 (62.0%) women had non-HGSC carcinomas. The converted maximum opioid use throughout all clinical courses was as follows: <25 mg in 43 (54.4%) patients and ≥25 mg in 36 (45.6%) patients. Thirty-seven (46.8%) patients received >15 cycles of chemotherapy. Furthermore, with regard to where patients received EOL supportive care, 30 were in the home/hospice group (38.0%) and 49 in the hospital group (62.0%) (Table 1).
Patients' Characteristics
ECOG, Eastern Cooperative Oncology Group; HGSC, high-grade serous carcinoma.
Palliative treatment and PCS
Figure 1 depicts the Kaplan–Meier curve of PCS for all patients. The median PCS was 10.8 weeks. We subsequently examined the frequency of EOL medical care in all patients. As shown in Supplementary Table S1, the frequencies of palliative treatments were as follows: pain control (94.9%), intravenous hyperalimentation (31.6%), frequent paracentesis and/or thoracentesis (26.6%), ileus tube/nasogastric (nasal small bowel/stomach decompression long tube) (21.5%), nephrostomy/ureteral stent (12.7%), blood transfusion (10.1%), oxygen inhalation (7.6%), intestinal bypass/colostomy (5.1%), and sedation (2.5%). Table 2 shows Cox univariable analysis of the abovementioned clinicopathologic factors in relation to PCS of women enrolled. Overall, the age (≤55 vs. >55: p = 0.0109), ECOG performance status (0–1 vs. 2–3: p < 0.0001), and EOL place (hospital vs. home/hospice: p = 0.0087) were significant prognostic factors for PCS. There was a marginally significant difference in PCS between women with and without frequent paracentesis and/or thoracentesis (absent vs. present: p = 0.0889). We next conducted Cox multivariable analysis to investigate the independence of their significance on PCS and eliminate selection biases among several of the aforementioned indicators, including the age, ECOG performance status, frequent thoracentesis and/or paracentesis, and EOL place (Table 3). Also in the multivariable model, the ECOG performance status and EOL place retained their significance as independent prognostic factors of poorer PCS (ECOG performance status [2–3/0–1]: HR = 3.279 [95% CI 1.967–5.586; p < 0.0001], EOL place [hospice/home hospice]: HR = 0.574 [95% CI 0.355–0.913; p = 0.0188]) (Table 3). Figure 2 depicts PCS curves on stratification by the EOL place. A significant difference was identified in PCS between women in the home/hospice and those in the hospital group (Log-rank: p = 0.0083; Fig. 2). Supplementary Table S2 shows a summary of survival rates and the log-rank test for PCS.

Kaplan–Meier-estimated PCS in terminally ill ovarian carcinoma patients. Medium survival: 10.8 weeks. PCS, postcancer treatment survival.

Kaplan–Meier survival curves of PCS on stratification by the end-of-life place (hospital vs. hospice/home care). Solid line: home/hospice group (N = 30), dotted line: hospital group (N = 49). Log-rank: p = 0.0083. The original cohort.
Cox Univariable Analysis of Clinicopathologic Parameters in Relation to Postcancer Treatment Survival of Patients Enrolled
95% CI, 95% confidence interval; HGSC, high-grade serous carcinoma; HR, hazard ratio.
Multivariable Analysis of Clinicopathologic Parameters in Relation to Postcancer Treatment Survival of Patients Enrolled
Survival analyses using the PS-weighted cohort
Actually, the choice of EOL place is influenced by various physical and socioeconomic conditions. The PS of the EOL place was calculated for each woman based on five clinicopathologic parameters: the age, histological type (HGSC vs. non-HGSC), ECOG performance status (0–1 vs. 2–3), converted maximum opioid intake (<25 mg vs. ≥25 mg), and frequent thoracentesis/paracentesis (presence vs. absence). The weighted baseline characteristics of eligible women, stratified according to the PS of the EOL place (hospital vs. home hospice), are shown in Supplementary Table S3. After IPTW adjustment, all conditioning variables were well balanced. In the IPTW-adjusted cohort, the median PCS was 15.0 and 9.7 weeks in the home/hospice and hospital groups, respectively (Fig. 3). There was a significant difference between the two cohorts (Log-rank: p = 0.040). Furthermore, in a Cox multivariable hazard model using the PS-weighted cohort, the EOL place retained its significance for PCS (IPTW-adjusted: HR [95% CI]: 1.548 [1.009–2.374], p = 0.045, multivariable adjusted with IPTW: HR [95% CI]: 1.670 [1.077–2.588], p = 0.022) (Supplementary Table S4).
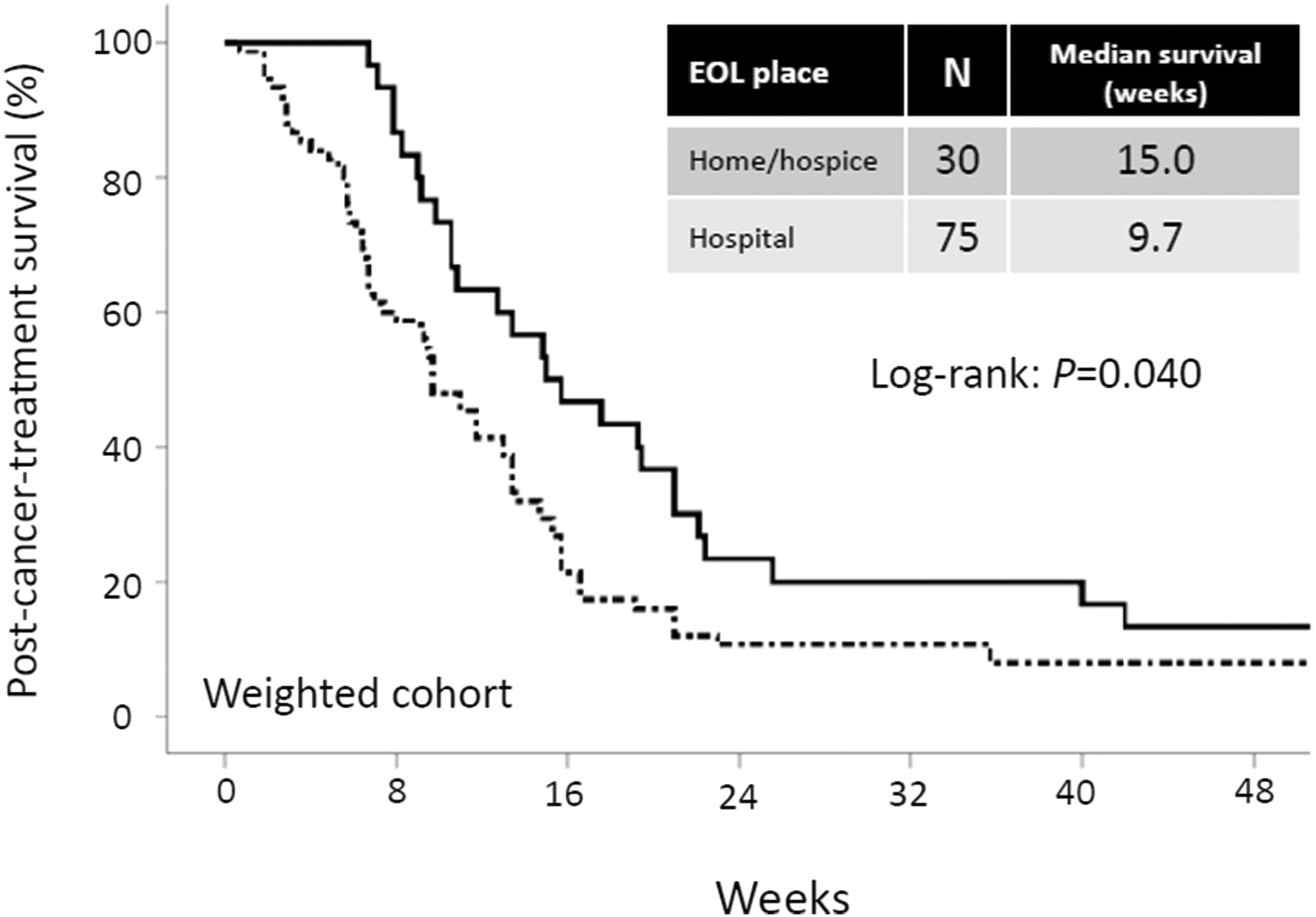
Kaplan–Meier survival curves of PCS on stratification by the end-of-life place (hospital vs. hospice/home care). Solid line: home/hospice group (N = 30), dotted line: hospital group (N = 75). Log-rank: p = 0.040. The IPTW-adjusted cohort. IPTW, inverse probability of treatment weighting.
Discussion
Therapeutic options for OC are becoming increasingly diverse due to the emergence of many chemotherapeutic agents, leading to higher expectations of medical treatment. Accordingly, numerous women with OC tend to undergo chemotherapy until the EOL stage. 13 As a result of their unrealistic expectations regarding the prognosis as well as physicians' explanations, many patients want to continue chemotherapy, even when the general condition worsens at the EOL stage. In the current investigation, we demonstrated that diverse palliative treatments at the EOL stage included pain control (94.9%), intravenous hyperalimentation (32.6%), frequent paracentesis and/or thoracentesis (26.6%), ileus/nasogastric tube (21.5%), nephrostomy/ureteral stent (12.7%), blood transfusion (10.1%), oxygen inhalation (7.7%), intestinal bypass/colostomy (5.1%), and sedation (2.5%). According to an earlier report including 62 women with OC in their last year of life, few were hospitalized with an unfavorable clinical event (bowel obstruction, pleural effusion, ascites) during the 6–12 months preceding their death; in contrast, during the last 6 months of life, more women were hospitalized for serious clinical events. 14 Actually, the multiple occurrence of those clinical events may be a sign of when to cease chemotherapy. We revealed a median PCS of 10.8 weeks, defined as the time interval from the cessation of anticancer treatment to death. Moreover, through multivariable analysis, we identified two predictive indicators that significantly impacted on PCS. According to our prior report, investigating a cohort of 181 gynecologic malignant tumor cases, patients in a hospice/home care group showed a significantly more favorable PCS than those in a hospital group. 10 However, this previous study included heterogeneous gynecologic malignancies. Since in women with OC, primary therapeutic modalities as well as peculiar tumor-related symptoms have significant effects on the quality of life, we individually need to reconsider the importance of the EOL environment for patients with this tumor. Eventually, women with OC belonging to the home/hospice cohort showed a better prognosis after anticancer treatment than those of the hospital cohort. What is the reason why home/hospice care contributed to survival improvement? Based on a prior report by Keyser et al., analyzing 81 women with recurrent gynecologic tumors, the median survival was significantly longer in 52 hospice patients than 29 nonhospice patients (9 months vs. 17 months, respectively) without any adverse event influencing survival in patients in hospice. 15 In contrast, according to a study by Connor et al. examining the survival of 4493 patients, the mean survival was 29 days longer for hospice patients than for nonhospice patients. 16 Hospice referral is a medical shift from anticancer treatments to holistic care focusing on management of the quality of life and symptoms. Although the nonhospital care aims neither to hasten death nor to prolong life, relevant mental stability and satisfaction may exert positive effects for the improvement of patients' lives.
In general, hospitalized patients are expected to have a poorer and more severe general condition and receive intensive and invasive medical procedures due to disease progression. Even though we conducted multivariable analysis including the ECOG performance status, we could not deny the possibility of a bias related to patients' physical status. Recently, abundant evidence demonstrated the effectiveness of a PS-matching/weighting technique as an alternative to a randomized controlled trial (RCT).11,17–20 In this study, in the IPTW-adjusted cohort, the median PCS was more than five weeks longer in the home/hospice group than in the hospital group (p = 0.040). Furthermore, in a Cox multivariable hazard model using the PS-weighted cohort, the EOL place retained its significance for PCS (multivariable adjusted with IPTW: HR [95% CI]: 1.670 [1.077–2.588], p = 0.022). As a consequence, we re-realized that the EOL place was an independent prognostic indicator for PCS. When balancing the benefits and demerits of total support, we should keep in mind that we can choose the EOL place. At least, we should understand the possible effect of transferring to home/hospice, and should not persist with anticancer treatment when it becomes ineffective and harmful.
Our current study includes several limitations. Initially, because this study was essentially retrospective, many factors relevant to treatment decisions were not as strictly controlled as they would be in an RCT. Subsequently, several critical data, such as on the pre-existing illnesses, duration of prior chemotherapy response, and objective inflammatory biomarkers related to the physical condition, were not provided. In particular, information about duration of prior chemoresponse is important because it might reflect further response of additional chemotherapy, leading to select chemotherapy rechallenge. In addition, this study did not provide the socioeconomic factors, including the presence or absence of their families, location of hospital or hospice in their community, and income, which may influence the placement decision. Furthermore, since death within four weeks after chemotherapy may relate to the toxicities, we could not deny the possibility of the negative impact of anticancer treatment on patients' PCS. In contrast, a strength of our study is that it was based on the same treatment criteria, including chemotherapy protocol, surgical modality, and palliative care of a single institution. Although this study is a hypothesis-generating study with many limitations, the main clinical utility of our study may be perception of the current status of palliative medicine, EOL prognosis, and importance of the EOL place. We hope to reassess and verify the present results in a future trial, shedding light on the optimal palliative strategy to treat patients with this malignancy.
In conclusion, palliative medicine is an essential approach focusing on not only symptom control but also on holistic care for each patient with OC and their family. It is important for us to balance between clinical effectiveness and adverse event of chemotherapy at near EOL stage. However, treatment with chemotherapy in patients with a poor performance status seems apparently inappropriate clinical practice. Nevertheless, when to cease chemotherapy is now inconclusive. Although our current data are preliminary, it is possible that the EOL environment is a crucial prognostic factor for survival after anticancer treatment. The present data are hypothesis generating for women with OC and physicians confronting these important issues. We hope that the current results will be reconfirmed in a future trial to further evaluate the importance of nonhospital care.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.