
Abstract
Background:
Studies suggest palliative care may be different in cystic fibrosis (CF) than in other conditions. To provide quality palliative care to individuals with CF, unique needs must be understood.
Objective:
To examine perceptions of how palliative care may be different in CF, top palliative needs of individuals with CF, and barriers to palliative care in CF.
Methods:
Online surveys with closed- and open-ended questions about palliative care needs were administered to multiple stakeholders in CF care, including adults with CF, caregivers of individuals with CF, and CF care team members from U.S. centers. We used descriptive statistics to report survey findings.
Results:
A total of 70 adults with CF, 100 caregivers, and 350 care team members completed surveys. While care team members reported they introduce palliative care to patients a majority of the time, adults with CF and caregivers rarely recalled learning about it. Very few reported having seen a palliative care specialist. A majority of participants reported that palliative care is valuable in CF care. Over 80% of participants felt palliative care is different in CF, most often citing the unpredictable disease course. Top palliative care needs identified include emotional support, emotional symptom management, and communication about treatment decisions. Major barriers to palliative care identified include perception that it is for dying people and lack of CF care team knowledge and training in palliative care.
Conclusions:
Participants felt palliative care is valuable in CF and identified many palliative care needs, and also barriers that can be addressed with education and training. Our findings will be used to develop interventions targeting specific needs and inform guidelines to enhance provision of palliative care in CF.
Introduction
Cystic fibrosis (CF) is a life-threatening multisystem genetic disease marked by progressive decline in lung function, numerous distressing symptoms, a burdensome daily treatment regimen, and complex medical decision making, including lung transplantation for some with advanced disease. 1 Evidence from meta-analysis of randomized clinical trials supports that palliative care improves a variety of outcomes, including patient quality of life, symptom burden, satisfaction with care, and health care utilization for those with serious illnesses. 2 Yet, as with many other noncancer illnesses, 3 the evidence base for palliative care in CF is limited. Nevertheless, an intuitive assumption of palliative care's high likelihood of benefit has motivated emerging interest to integrate palliative care into CF care.
Previous reports emphasize that palliative care may be different in CF than in other life-limiting conditions. A variety of reasons may account for differences, including the relatively young age of people with advanced disease, challenges with prognostication for individuals, the availability of lung transplant as a treatment for some people with advanced CF lung disease, and development of disease-modifying therapies that are expected to alter the course of illness for a majority of individuals with CF.1,4 In addition, most individuals with CF in the United States are treated by CF care teams that include clinicians, therapists, and psychosocial providers with diverse professional training who endeavor to provide comprehensive care for all aspects of this serious chronic illness. Potential differences aside, individuals with CF face the prospect of extensive symptom and treatment burden, complex decisions, and uncertain futures.
Although models of palliative care delivery and clinical practice guidelines in other conditions5–7 may serve as templates for developing palliative care in CF, they can only be adapted to best serve individuals with CF once differences and unique needs are better understood. 8 As such, we explored palliative care needs, perceptions of palliative care, and barriers to palliative care in CF from the perspectives of adults with CF, family caregivers of children and adults with CF, and CF care team members as an important step in the development of clinical models of palliative care delivery and clinical practice guidelines in CF.
Methods
Members of the author group, with input from multiple stakeholders including individuals with CF, CF caregivers, CF clinicians and researchers, palliative care clinicians and researchers, and quality improvement experts, developed parallel online surveys for adults with CF, caregivers, and CF care team members. The format was inspired by an international survey that informed development of guidelines for screening and treatment of anxiety and depression in individuals with CF.9,10 This survey was adapted to the subject matter using existing literature on palliative care in CF,11–15 a widely recognized statement on primary versus specialty palliative care applicable to any serious illness, 16 and guidelines for palliative care in other conditions.5–7,17 Demographic information was collected from all participant groups, and survey domains included palliative care needs, perceptions of palliative care, barriers to palliative care, and knowledge of existing resources. Survey questions were both closed (yes/no, scaled, ranked) and open ended. The survey instrument was tested for clarity and face validity by members of the research team and revised with input from representatives of all stakeholder groups.
The approved surveys (University of North Carolina Institutional Review Board No. 17-1510) were administered using the Qualtrics online platform (© 2017 Qualtrics, Provo, UT; https://qualtrics.com) using U.S. Cystic Fibrosis Foundation listservs. The Community Voice listserv, available to any adult with CF or family caregiver of children and adults with CF, reached up to 500 subscribing adults with CF (N = 210) and family caregivers (N = 290) at the time of the survey. A total of eleven CF care team member listservs reached up to 3500 CF care team members in a variety of disciplines. Overlap among CF Foundation listserv subscribers makes it impossible to determine the total number of eligible CF care team participants.
Participants were provided with an electronic consent form and were notified that informed consent was implied by completion of the survey. A CF-specific definition of palliative care created by an analogous stakeholder group was provided in the recruitment e-mail and on each page of the electronic survey: “Palliative care focuses on reducing physical and emotional symptoms and improving quality of life for people with CF throughout their lives. Palliative care occurs alongside usual treatments and is individualized according to the unique goals, hopes and values of each person with CF.” 18 Examples and definitions of potentially unfamiliar palliative care concepts and terms were offered in the survey text. The survey remained open for three weeks from July to August 2017, with a reminder e-mail sent 10 days after the initial recruitment e-mail.
Summary statistics was used to report demographic data and responses to closed-ended questions. Comparisons were made among participant groups and within groups, when relevant, using chi-squared tests, with an a priori α-level of 0.05 for statistical significance.
Results
A total of 520 surveys were completed by participants from around the United States, including 70 adults with CF, 100 caregivers, and 350 care team members, with 33% of eligible adults participating, 34% of eligible caregivers, and an unknown response rate for care team members (see Methods section). Participant demographics are detailed in Table 1. As the Community Voice listserv is available to adults with CF regardless of severity or lung transplantation history and to caregivers of adults with CF also regardless of disease severity, we presume that a spectrum of ages and disease severity were represented. While all individuals with CF completing the survey were adults, most caregivers were parents of individuals with CF receiving care in pediatric CF programs. Care team members represented pediatric and adult programs equally, and 11% were also members of lung transplant teams. Very few adults with CF and caregivers reported personal experience with palliative care. While only 3% of care team members reported also being members of a palliative care team, 15% reported having participated in some form of palliative care training.
Participant Demographics
CF, cystic fibrosis.
Experience with and perceptions of palliative care
After reviewing the definition of palliative care in CF, 18 73% of care team members reported their team introduces palliative care to individuals with CF, but only 26% of adults with CF and 12% of caregivers recalled it being introduced by the CF care team, with no difference among adult versus pediatric CF programs. When asked about the value of palliative care in CF, all care team members, 83% of adults with CF, and 67% of caregivers indicated that it is valuable; 15% of adults with CF and 29% of caregivers did not know if palliative care is valuable. There were no differences in ratings of the value of palliative care in CF among caregivers of children versus adults (92% vs. 100%, p = 0.48) or care team members caring for children versus adults (100% reported value) who selected a response option other than “I don't know.”
A majority of participants, including 85% of adults with CF, 87% of caregivers, and 84% of care team members felt palliative care in CF differs from palliative care in other conditions. After reviewing a prespecified list of reasons why palliative care may be different in CF than other serious illnesses, all groups ranked the unpredictable disease course as the top difference. Other key differences identified by all participant groups included shortened life expectancy and CF being a lifelong disease (Fig. 1). Notably, caregivers and care team members placed more emphasis than adults with CF on issues such as relative isolation from CF peers and the complex daily treatment regimen. Care team members were more likely than adults with CF or caregivers to rate the following as top reasons palliative care in CF is different: the option of lung transplant for some individuals with CF, and palliative care specialists not understanding CF.
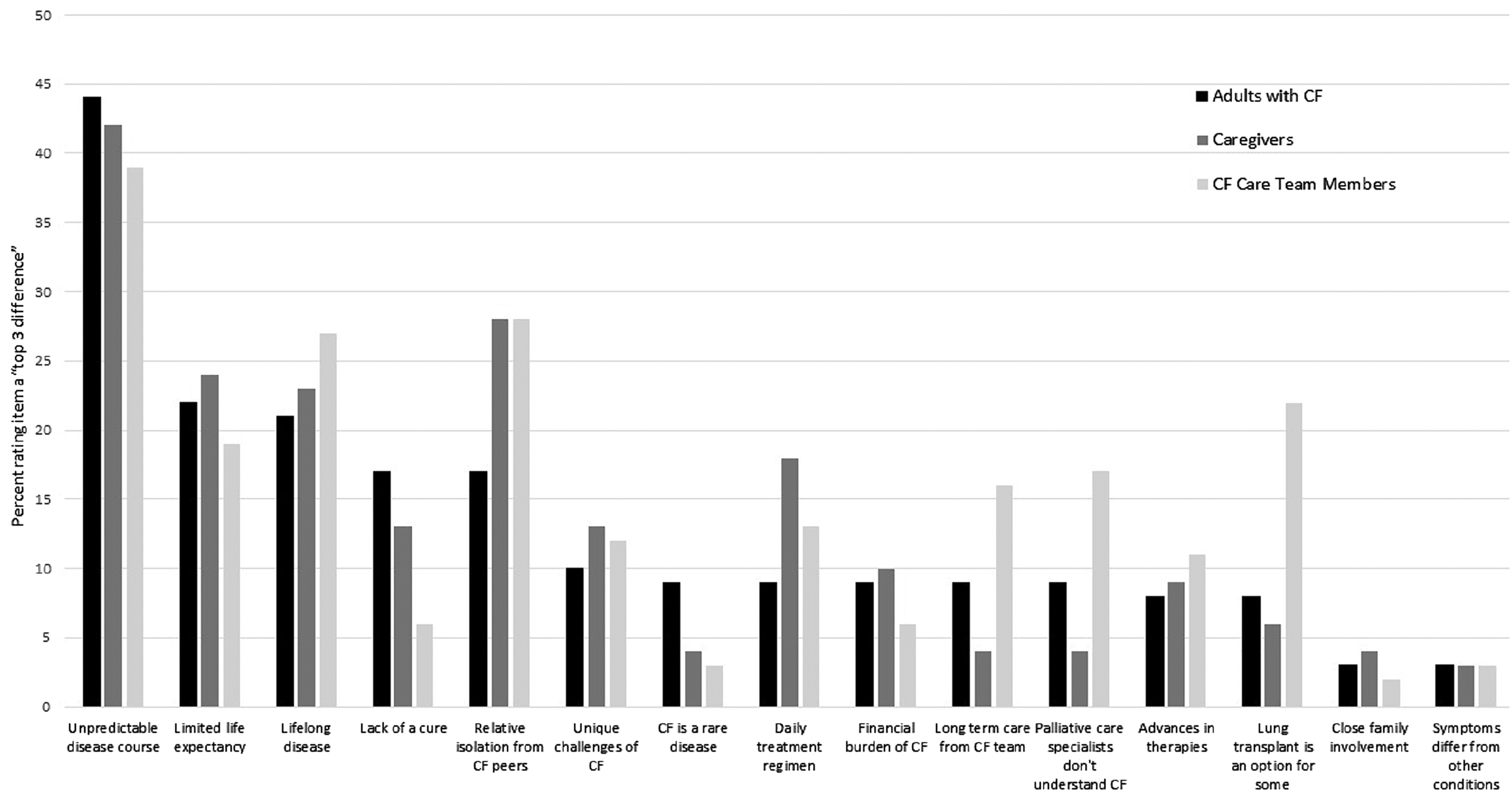
Participant ratings of top reasons palliative care is different in CF. Top 3 choices from a list of 15 options were chosen by participants. CF, cystic fibrosis.
Palliative care needs in CF
From a list of common palliative care needs, emotional support, defined as “help for coping with serious illness, grief, and losses related to CF,” was identified as the top palliative care need of individuals with CF (Table 2; Appendix A1), ranked first by 38% of adults with CF, 45% of caregivers, and 49% of care team members; anxiety and depression management was also a top need as per adults with CF and caregivers. Adults with CF and care team members felt advance care planning is a top palliative care need. This was defined for survey participants as, “planning for future medical care, including wishes for treatments like life support.” One adult with CF spoke of several of these needs by writing, “We [individuals with CF] need to be led. We don't know what we're fighting sometimes, we just keep going. We need support and guidance; we won't be the ones to ask for it.” Another adult with CF wrote, “A lot of times we're too sick to be healthy but too healthy to be sick. The hardest decisions should have time put into them before hand, not in crisis mode.” Caregivers and CF care team members rated physical symptom management, described as “management of pain and other physical symptoms,” as a top need more often than adults with CF (28% and 37%, respectively, vs. 18%), and adult care team members ranked physical symptom management as a top need more often than pediatric care team members (47% vs. 29%, p = 0.001). Adults with CF and caregivers more often identified caregiver support as a top need than care team members, and pediatric care team members identified caregiver support as a top need more often than adult care team members did (28% vs. 16%, p = 0.011). A caregiver of a child with CF wrote, “Simply, it's a scary world for a CF patient and their caregivers. All and any additional support is appreciated.”
Greatest Palliative Care Needs of Individuals with Cystic Fibrosis and Top Barriers to Palliative Care
Percent of each participant group ranking the needs and barriers is indicated in parentheses.
Barriers to palliative care in CF
From a list of common barriers to palliative care (Appendix A1), all groups identified the same top 3: perception that palliative care is only for dying people, lack of access to outpatient palliative care services, and lack of palliative training for CF care team members. In addition, CF care team members identified concerns about how individuals with CF and caregivers would react to talking about palliative care as a top barrier (Table 2). Nearly one-third of care team members felt the reluctance of individuals with CF to engage in palliative care conversations as an important barrier, versus 5% of adults with CF and caregivers (p < 0.01 for both comparisons). Two-thirds of adults with CF and 74% of caregivers were not aware of the availability of palliative care specialists, and 19% of care team members did not know if palliative care specialists were available to their patients. Lack of time to address palliative care needs was more commonly cited by caregivers of adults than children (32% vs. 13%; p = 0.035). Adult care team members more often ranked lung transplant as a top barrier than pediatric care team members, specifically that palliative care is not appropriate for lung transplant candidates (21% vs. 11%; p = 0.015). Adults with CF and caregivers did not endorse this bias in ranking barriers or in open-ended comments. Transplant team members, regardless of the population served, also rated this as an important barrier more often than care team members who do not participate in transplant care (30% vs. 16%; p = 0.03). One care team member said, “It makes the timing difficult; planning for a transplant is creating hope and palliative care often implies lack of hope.” In contrast, another care team member wrote, “[Palliative care] should be ongoing, not just end of life, especially when patients are starting to decline or are having a lot of distressing symptoms. Ideally this would occur regardless of transplant plans.”
Discussion
Our large national survey of key stakeholders in CF care revealed that many adults with CF, caregivers, and CF care team members feel that palliative care is different in CF than other serious illnesses because of the unpredictable illness course, limited life expectancy, and the fact that it is lifelong, yet remains valuable as a means to improving their quality of life. Respondents were able to identify a variety of important palliative care needs, centered on emotional symptoms and communication. Barriers to palliative care, largely reflecting knowledge gaps and societal biases about palliative care being only for those who are dying, were identified. Notably, unlike CF care team members, adults with CF and caregivers did not identify reluctance to engage in conversations about palliative care as a top barrier; this, in combination with agreement across participant groups about the top palliative care needs, invites development of improved palliative care practices for individuals with CF.
Major challenges for the field and practice of palliative care include defining it in the context of serious illness care and addressing misperceptions and anxiety around palliative care being just about death and dying. As CF care team members become more familiar with palliative care through education and training, they may feel more comfortable introducing concepts to individuals with CF and even identify what they are already talking about as “palliative care.” Then, individuals with CF and caregivers may better recognize that they are actually having palliative care conversations and receiving primary palliative care from their CF teams. In addition, they may feel empowered to share concerns about unmet palliative care needs, but needs must be proactively explored to be appropriately addressed. Screening for palliative care needs and then implementing appropriate interventions to address unmet needs, both within the CF care team and through appropriate referral to palliative care specialists, are avenues to improving care. Screening and implementation of specific interventions are likely to differ across pediatric and adult settings, when transplantation is a consideration and transplant care teams are added to the provider mix, and of course as outcomes such as survival and quality of life continue to change with advances in CF therapies. The impact of lung transplant on palliative care in CF also warrants further exploration. Palliative care clinical practice guidelines specific to CF could aid CF and palliative care clinicians in their practices and help overcome barriers.
Limitations of this study include use of a nonvalidated instrument to assess palliative care needs, offering prespecified lists of needs and barriers as response options, recruitment of a convenience sample of participants who may be biased for or against palliative care and/or have greater knowledge than the overall CF community based on decision to participate, omitting adolescent participants by nature of the stipulations for listserv participation, and an indeterminable CF care team member response rate due to an uncertain total number of care team members receiving the survey. Clinical experience in both CF and palliative care among members of the research team support face validity of the survey instruments. Offering prespecified response options likely enhanced participation among those who would be deterred by a large number of open-ended questions, and may result in participants considering responses they would not have offered without prompts. Responses to questions about palliative care experience as well as comments about open-ended questions suggested baseline low knowledge of palliative care among all participant groups. The large, heterogeneous sample should help minimize biases and enhance generalizability of our findings. While data are limited to U.S. CF care centers, international studies indicate the need for a more comprehensive and systematic approach to palliative care in CF.14,19–23
Conclusions
We found that many gaps in knowledge about palliative care exist among adults with CF, caregivers, and CF care team members. While key stakeholders feel palliative care is valuable in the context of CF and agree on the top specific palliative care needs of individuals with CF, there are varying perceptions of palliative care as a part of CF care. The most common barriers to palliative care reflect gaps in knowledge, anxiety about the topic of palliative care, and societal biases, and could be addressed with palliative care education for the CF community, interventions targeting specific palliative care needs of individuals with CF across the spectrum of the disease, and guidelines to assist CF care teams, transplant teams, and palliative care specialists in providing palliative care to individuals with CF.
Footnotes
Acknowledgments
The authors thank the Cystic Fibrosis Foundation for facilitating this research through care team listservs and Community Voice. They are particularly grateful to the adults with CF and CF family members across the United States for sharing their insights through Community Voice.
Data presented at the North American Cystic Fibrosis Conference, Denver, CO, October 2018, and the American Academy of Hospice and Palliative Medicine Annual Assembly, Orlando, FL, March 2019.
Funding Information
This research was supported by the Cystic Fibrosis Foundation.
Author Disclosure Statement
No competing financial interests exist.
Appendix A 1. Selected Survey Items
What do you feel are the greatest palliative care needs of individuals with cystic fibrosis (CF)? (Select top 3):
Advance care planning: planning for future medical care, including wishes for life-sustaining treatments. Support for decision making about complex medical treatment such as feeding tubes and lung transplant. Defining goals for medical care. Emotional support: help for coping with serious illness, grief, and losses related to having CF. Spiritual support. Management of pain and other physical symptoms. Management of emotional symptoms such as anxiety and depression. Planning for end-of-life care. Creating advance directives (living will, health care proxy/power of attorney). Emotional support needs of family members/caregivers.
Please select the top 3 reasons why palliative care is different for individuals with CF than for people with other serious medical conditions:
What do you see as the barriers to accessing palliative care for individuals with CF? Please select the top 3: