
Abstract
Background:
Bereavement programs provide institutions with an avenue for obtaining feedback from family members about their experiences during a patient's illness and end-of-life (EOL) period that can be used to improve both patient care and the care of bereaved individuals.
Objective:
We examined family members' experiences about the clinical care their loved one received at EOL and the perceived effect this care had on their subsequent bereavement.
Design:
Survey.
Setting/Subjects:
One hundred forty bereaved family members from our cancer institute completed a bereavement survey. Of these family members, 67% were female, 66% were 60 years of age or older, and 81% were widowed.
Measurement:
We analyzed open-ended responses using NVivo 11 Plus© that asked bereaved family members about the ways the clinical (oncology) team was helpful or not in dealing with their loss.
Results:
The findings showed that compassionate care, competency, receiving honest facts, and outreach after the death favorably influenced the bereavement experience. Conversely, impersonal contact, lack of contact, including lack of caregiver support, and lack of information about EOL and death were identified as actions taken by the clinical team that were unhelpful in dealing with their loss.
Conclusions:
The feedback from bereaved family members highlights two areas that could benefit from quality improvement efforts: (1) communication skills that focus on enhancing compassionate connection, including conveying empathy, and providing reassurance and guidance to patients and their families and (2) communication skills that focus on delivering information about prognosis and the EOL period in an honest and direct way.
Introduction
As the field of palliative medicine grows, the existence of bereavement programs provides an avenue for clinicians and hospital administrators to learn more about the experience of patients at the end of life (EOL) and their families. Obtaining feedback from bereaved family members or caregivers about their experiences during the patient's illness and EOL period can provide important insights into ways to improve both patient care and the care of bereaved families.1–3
Research shows that the provision of palliative care and hospice services is associated with improved family satisfaction,4–6 improved family-reported quality of EOL care, 7 and better bereavement outcomes.8,9 Roza et al., for example, found that family members of patients who died while receiving care in a dedicated palliative care unit report higher overall satisfaction with the medical care their loved one received and emotional support after the patient's death compared to the consultation service or usual care, defined as those patients who stayed in the hospital for at least 48 hours, but did not receive palliative care. 5 Wachterman et al., reporting on a large Veteran Affairs study of bereaved family members, found that higher rates of palliative care consultation, do-not-resuscitate orders, and fewer deaths in the intensive care unit were associated with better family-reported quality of EOL care, 7 consistent with Wright et al.'s findings from a national study of elderly patients with advanced lung or colorectal cancer. 6 Furthermore, Higgins et al. 10 found that caregivers' assessment of quality of EOL care, and in turn bereavement outcomes, was related to the use of hospice and the place of death, which they argue are potentially modifiable targets for health care providers.
Given that bereavement care is best conceptualized as a preventive model of care where the goal is to identify those individuals potentially at risk of poor bereavement outcomes and intervene early,1,11 developing ways to improve bereavement outcomes for family members before and after the death of the patient is essential. Adopting a quality improvement framework, feedback from bereaved individuals, can help guide the development of targeted interventions to improve care of patients and their families.
In this article, we analyzed open-ended responses about EOL experiences from an earlier survey of bereaved family members whose loved ones had died at our cancer center. 1 Thematic coding was conducted to yield caregiver insights into the clinical care their loved one received at EOL, and the impact it had on their subsequent bereavement. We also assessed the actions taken by the clinical team that caregivers reported either helped or impeded their bereavement experience, underscoring opportunities to improve clinical practice about EOL care and bereavement.
Methods
Sample
In 2014, 815 bereaved family members, whose loved one died in the second half of 2013, were invited to complete a survey describing their experience with the bereavement program at our cancer center. 1 Eligible participants were the family contacts listed in the bereavement program database, who had received the outreach mailing as part of our routine bereavement services. Participation was voluntary, and responses were anonymous. The paper-and-pencil survey, entitled “Dana-Farber/Brigham & Women's Cancer Center Bereavement Program Survey” was mailed to the family contact with a letter outlining the consent process. If the individual agreed to complete the survey, they returned their responses in a self-addressed envelope, and if they did not agree, no further action was taken. The Institutional Review Board of Dana-Farber Cancer Institute (DFCI) approved this study.
The survey was developed by 2 of the authors (SM and SB) and consisted of 21 questions assessing which components of the bereavement program family members found most helpful and what other types of support we could have offered. Nine questions included a yes/no dichotomous response and a five-point Likert scale rating asking about the impact of specific components of the bereavement program. Four questions were related to demographic data and the remaining eight questions, including six open-ended questions, asked about follow-up from both the bereavement program and the patient's clinical team. The purpose of this analysis is to examine the responses to four questions, listed in Table 1, which specifically asked the family member about the care provided to the patient by the clinical team and their subsequent bereavement. The first question was a global assessment of the quality of care their loved one received by the clinical team using a 10-point Likert Scale. Three other questions were open ended, asking about the actions of the team and the effect these actions had on their bereavement.
Survey Questions
Data analysis
All open-ended data were de-identified and uploaded to NVivo 11 Plus©. Data analysis was conducted by two study team members (SM and MN), incorporating aspects of grounded theory to better understand experiences of bereaved family members.12,13 A multistage thematic analysis of preconfigured and emergent codes was used. One team member (SM) independently conducted the first round of coding, which was descriptive in nature and identified the coding structure. An inductive approach was utilized in the second round and a broader thematic framework was then applied across all open-ended responses. Both study team members met regularly to develop a codebook, review coding, discuss emergent categories, and reach consensus to finalize the parameters of the categories. A heat map, shown in Figure 1, was created using NVivo 11 Plus© to provide a visual representation of the various thematic codes for each question. The size and color of the rectangles reflect the frequency of coding references. Darker and larger rectangles correspond to the most commonly identified themes by family members. Within some categories, there are several nodes of lighter color, reflecting different subthemes.
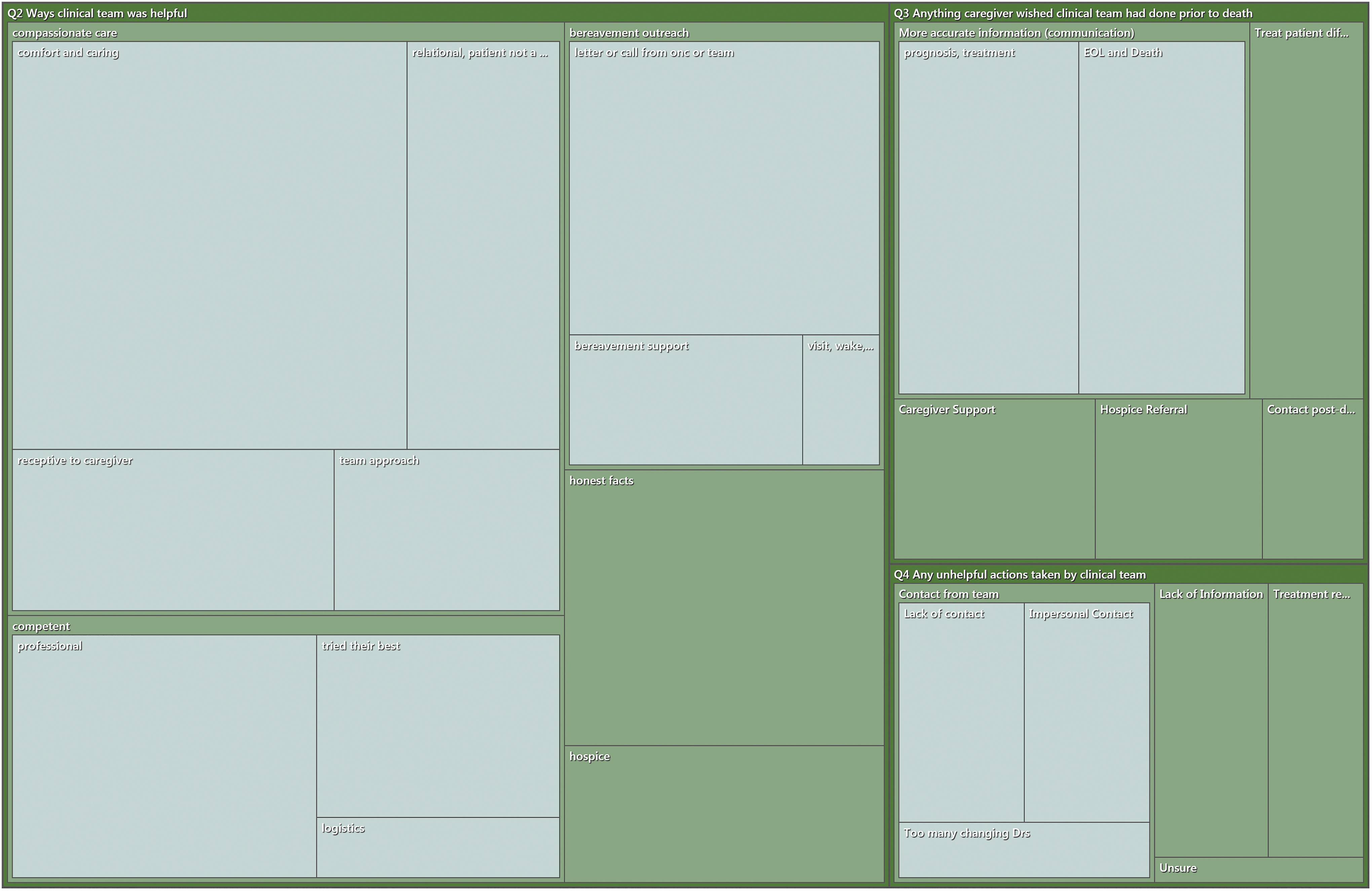
Heat map key. The size and color of the rectangles illustrate the frequency of coding references. Larger and darker rectangles correspond to the more commonly referenced themes.
Results
One hundred forty recently bereaved family members completed the bereavement survey (17% response rate). Approximately, 67% were female, 66% were 60 years of age or older, and 81% had lost a spouse or partner. The results from four survey questions that inquired about the care their loved one received at EOL and its impact on their bereavement are described below. The heat map (Fig. 1) illustrates the main themes of the data reported in Questions 2–4, and Tables 2–4 list corresponding exemplar quotes.
Ways the Clinical Team Was Helpful in Dealing with Your Loss
Anything That You Wished the Clinical Team Could Have Done Prior to Your Loved One's Death That Would Have Helped You in Dealing with Your Loss
Any Actions Taken by Your Loved One's Clinical Team That Were Unhelpful or Difficult for You in Dealing with Your Loss
Using a Likert scale from 0 to 10, where zero corresponded to “very poor” and 10 to “excellent,” 85% of participants evaluated the care their loved one received from the clinical team very positively, endorsing 8, 9, or 10 on this scale.
In response to question 2, there were 137 references that were categorized into five themes. As shown in Figure 1, Q2, these themes were as follows: “Compassionate Care,” “Competent,” “Bereavement Outreach,” “Honest Facts,” and “Hospice.” Some responses were brief and only mentioned one theme, while other responses were detailed, incorporating several themes that were coded separately. As one spouse wrote, “They phoned, emailed and sent cards. They met with me on May 6… Dr. M. told me about (husband) in a way that meant he was a person to her, not just a patient. She also sent me a beautiful note that she thought I took good care of him—which meant so much to me. DFCI and the BWH Hospital were such places of hope to me during (husband's) illness. I feel everyone did their best for him there. Thank you” (ID-96).
Compassionate Care (60 references)
Compassionate Care was defined by the study team as any response that indicated that the clinical team showed or communicated empathy, caring, and concern. We identified four subthemes:
Compassionate Care: comfort and caring (31)
Comfort and caring included references to the team making the patient's experience more comfortable, the time spent with the patient, or the provider's communication style, indicating that they cared about them.
Compassionate Care: relational, patient not a number (12)
Relational, patient not a number refers to more personalized care, underscoring the importance of the patient being treated as a whole person within the context of a relationship with the provider.
Compassionate Care: receptive to caregiver (10)
This subtheme includes any positive comment that the team was inclusive of the caregiver and understood their role and needs in relationship to the patient's care.
Compassionate Care: team approach (7)
Team approach includes comments indicating a more comprehensive approach and the role of professionals from different disciplines.
Competent Care (27)
Competent Care was defined as the care of the patient that indicated the clinical team was competent, efficient, and/or professional, including the following three subthemes:
Competent Care: professional (15)
Responses indicated the team was professional in their conduct, responsive and courteous.
Competent Care: tried their best (9)
Tried their best refers to responses suggesting that the team exhausted all treatment possibilities, met the family's (high) expectations, and they went above and beyond.
Competent Care: logistics (3)
Logistics referred to help by the clinical team with the logistics of treatment, including scheduling and consolidation of appointments.
Bereavement Outreach (26)
Bereavement outreach was defined as contact from the clinical team that occurred immediately post-death up until several months later. This contact included attending the wake or funeral, condolence letters, and calls. It also includes support groups offered by the DFCI bereavement program. There were three subthemes:
Bereavement Outreach: letter or call from oncologist or team (18)
There were 18 references that participants had received a letter or call from a member of the team.
Bereavement Outreach: bereavement support (6)
This subtheme included receiving literature and attending a bereavement support group.
Bereavement Outreach: visit, wake, funeral (2)
Two mentions included a visit by a team member in the hospital at the time of death and attending the patient's funeral.
Honest Facts (16)
Honest facts was coded as receiving information about diagnoses, treatment, prognosis, and that the “end is near,” honestly and in a straightforward manner.
Hospice (8)
This theme includes receiving a hospice referral from the clinical team or accommodating the patient's wish to die at home. It does not refer to the care provided by the hospice team.
This question asked about what the team could have done before their loved one's death, which would have helped them in dealing with their loss. The responses were categorized into five themes as shown in Figure 1 with “More Accurate Information” being the most common, followed by “Treat the Patient Differently,” “Caregiver Support,” “Hospice Referral,” and “Contact Post-discharge.” There were 47 references in total.
More Accurate Information (25)
We defined this theme as the desire for communication over the course of the illness, including more accurate information about treatment options, disease-specific research, prognosis, and death. There were two subthemes:
More Accurate Information: treatment and prognosis (13)
This subtheme includes comments about realistic expectations being set by the team about the course of the illness, information about what to expect during visits, and information about treatment options, and prognosis, leading up to EOL or death.
More Accurate Information: EOL and death (12)
This subtheme includes any response specifically requesting more information about the dying process or expectations about timing of death.
Treat the Patient Differently (8)
This theme included references about treating the patient with more compassion or care, wishing the patient had attended fewer appointments or was not told about their prognosis.
Caregiver Support (6)
This subtheme included acknowledging the caregiver's role in the care of the patient and providing more support for the caregiver, including caregiver support groups and meeting with the family to update them.
Hospice Referral (5)
Five references were made about receiving an earlier or “better” hospice referral.
Contact Post-discharge (3)
A desire for contact from the team after the patient was discharged home was mentioned three times.
The final question asked about unhelpful actions by the team. As shown in Figure 1, 27 responses were categorized into 4 themes, including Contact from the Team, Lack of Information, Treatment Regret, and Unsure.
Contact from the Team (15)
This theme refers to any contact from the clinical team and is divided into three subthemes:
Contact from the Team: lack of contact (6)
Six references indicated that lack of contact post-death was unhelpful to them in dealing with their loss.
Contact from the Team: impersonal contact (6)
Similarly, impersonal contact, referring to the clinician's or team's communication style, was seen as unhelpful.
Contact from the Team: too many changing doctors (3)
Three mentions indicated that too many changing doctors were unhelpful for the family member in dealing with their loss.
Lack of Information (6)
This theme referred to both the lack of information from the team about the patient's prognosis before death and the reason for death itself.
Treatment Regret (5)
Treatment regret referred to the caregivers' regrets about some aspect of the patient's care.
Unsure (1)
One participant said they were unsure.
Discussion
The findings from this qualitative study demonstrate that bereaved individuals can provide important insights into how clinicians can improve the care of patients at the EOL and the care of bereaved family members. One hundred forty bereaved family members, the majority of whom were spouses, completed a bereavement survey about the care their loved one received from the clinical oncology team at our cancer center and the effect this had on helping them deal with their loss. Specifically, they were asked about the ways in which their loved one's clinical team was helpful in dealing with their loss, and the actions that were not helpful. While 85% of participants rated the overall care their loved one received very highly, a qualitative approach to analyzing the responses allowed us to elucidate more clearly the factors that were important to these bereaved individuals. Given the current focus on patient- and family-centered care at EOL and the increasing role that family members play in caring for sick and dying patients, 2 having a clearer understanding of what is important to caregivers not only improves the care of patients but also their bereavement experience. 14
We found that bereaved families most often reported compassionate care by the team as being helpful in dealing with their loss, followed by competence, bereavement outreach by clinicians, receiving honest facts about prognosis, and being referred to hospice. Compassionate care incorporated communication that conveyed empathy, caring, and concern for both the patient and caregiver, underscoring a personal, human connection. Such a connection cannot be minimized, especially in an oncology setting where patients have often been receiving treatment for years and the clinical team is considered to be a “second family.” Several family members acknowledged that it was difficult to suddenly sever their ties with the team after many years and expressed a desire for contact post-discharge or after the death of the patient.
Not surprisingly, receiving a condolence letter or call from the oncologist or team received the most references as being helpful within the bereavement outreach theme. These findings are consistent with those of a recent study by Kentish-Barnes et al. who investigated the benefits of receiving a condolence letter following the death of a patient in an ICU. 15 While the settings and relationships with the providers are different, Kentish-Barnes et al. identified a feeling of support and humanizing the medical system as two of the main benefits of receiving letters of condolence for family members. 15
When family members were asked about actions taken by the clinical team that were unhelpful or difficult in dealing with their loss, participants mentioned impersonal contact, such as the physician being too clinical, too many changing doctors, and a lack of contact after the patient's death. Each of these reflects a lack of connection or distance between the provider and the patient and family. Participants also described a lack of accurate information about both prognosis and treatment, and the EOL period and death as unhelpful.
Taken together, our findings suggest that the actions by the clinical team that were considered helpful by these bereaved family members included those actions that promoted human connection, reassurance, and guidance during a very difficult time. Conversely, those actions that were deemed unhelpful appear to have created emotional distance and a lack of connection, which, in turn, limited the opportunity for patients and their caregivers to receive guidance and information from the providers. These finding are consistent with Higgins et al. who examined factors predicting bereaved caregivers' perceptions of the quality of care at the EOL. 10 They suggest that whole-person physician care is important and that members of the interdisciplinary team, including social workers and chaplains, can coach patients and their caregivers in communicating their needs to their physicians. We would equally argue that these same team members and palliative care clinicians can also play a role in coaching oncologists and other physicians about ways to enhance their communication with patients and families about serious illness,16,17 highlighting compassion and empathy, and the need for accurate information about prognosis, EOL, and the dying process.
Limitations
This study has several limitations. First, the sample is a relatively small convenience sample. Second, the response rate is low, and third, the majority of respondents were bereaved widows older than 60 years. As such, the generalizability of our findings is limited, especially in relationship to other types of losses, notably the death of a child or parent. Future research should target a more varied sample of bereaved family members, including bereaved parents of pediatric-aged children and younger adults. In addition, developing better methods to recruit bereaved family members to participate in bereavement surveys is long overdue, given that response rates tend to be low.18–20
Conclusions
This study demonstrates the value and challenges of receiving feedback from bereaved family members about the care experience of their loved one, and their own experience in the immediate post-loss period. Family feedback highlights two areas that could benefit from more emphasis in quality improvement efforts: communication skills, especially those focused on providing honest and direct information about prognosis and the EOL period, and skills focused on enhancing compassionate connection, reassurance, and guidance to patient and families during this difficult time. New approaches to seeking feedback from bereaved families are needed so that health systems can continue to improve the care they provide.
Footnotes
Acknowledgments
Funding Information
There was no funding for this study.
Author Disclosure Statement
No competing financial interests exist.