
Abstract
Background:
Fetal malformations are diagnosed prenatally in nearly 3% of pregnancies, and ∼1.2% are major malformations. After prenatal diagnosis, it is imperative to consider families' values and to support their decision-making process. Prenatal palliative care is a growing field mainly based on family conferences. The prenatal care setting is unique and differs from postnatal and adult care. There are no descriptions of family conferences in prenatal palliative care. The descriptions of themes that emerge from the prenatal care conference charts may guide professionals in this delicate task, and help determine the causes of suffering and identify family values before the birth of the infant.
Aim:
To perform a content analysis of medical records of family conferences and to describe the main themes observed during prenatal palliative care follow-up after the diagnosis of a life-limiting fetal condition.
Design:
This is a retrospective study of medical records of family conferences from a perinatal palliative care group, the GAI group, between May 2015 and September 2016.
Setting/Participants:
Families with estimated perinatal mortality >50% and eligibility for follow-up at our tertiary fetal medicine center were enrolled. We included women who participated in at least one family conference with the GAI group and who had given birth at the clinic or delivered at another center and returned for the postnatal family conference.
Results:
Fifty women met the inclusion criteria. Five main themes and 18 categories emerged from the charts and are described in detail. A model of follow-up in prenatal palliative care is proposed based on the themes and categories identified.
Conclusions:
This analysis may guide health professionals who seek to better identify family needs and values and organize follow-up during prenatal palliative care.
Introduction
Since the 1980s, ultrasound and molecular diagnosis have led to a substantial improvement in prenatal diagnosis and the early detection of fetal malformations. 1 Currently, fetal malformations are diagnosed prenatally in nearly 3% of pregnancies, most of which can be diagnosed in the first trimester of pregnancy. Of these diagnosed malformations, 1.2% are severe fetal malformations, which are defined by alterations that will cause serious medical or functional consequences for the child, including death. 2 After the prenatal diagnosis of a life-limiting condition, it is imperative to consider families' values and to support the decision-making process and organization of fetal care in accordance with parental needs and values. 3
Palliative care principles have evolved and been described for adults and children; these principles now include follow-up of pregnant women, fetuses, and families after the prenatal diagnosis of life-limiting conditions.4–6 The first proposal for perinatal palliative care was published at the end of the 1990s in the United States. 7 The application of palliative care concepts to fetal medicine 5 and the first follow-up methods in a perinatal palliative care model were described in the early 2000s 8 . In 2004, the application of palliative care during the prenatal period and in the delivery room was first discussed. 9 Ten years later, the first discussion on perinatal palliative care in Latin America was published, addressing the demand for prenatal care in Argentina. 10
Therefore, palliative care in the prenatal period is a relatively new and growing field, and there are an increasing number of centers offering it. 11 Because follow-up in this setting involves surrogates for the unborn child, the model is based on family conferences12,13 and uses communication techniques that were adapted from the adult setting. To date, no study has described the themes present in family conferences in the prenatal palliative care setting. The description of themes in family conferences in prenatal palliative care may guide professionals in performing this delicate task and allow the investigation of suffering in this context; the data from such an investigation could be used to identify and minimize the suffering inherent in the context of prenatal palliative care. Because prenatal palliative care conferences deal with a very particular situation, namely, discussing issues pertaining to an unborn and unmet child and talking about that child's possible death even before birth, while the child is still fully protected in the womb, it is important to consider that the subjects and content of the conferences are highly unique and differ from those of palliative care conferences performed with the parents or surrogates of children or adults.
Considering the unique participants and circumstances of such conferences, the main objective of our study was to perform a qualitative analysis of family conference charts and to describe the main themes that emerge during prenatal palliative care follow-up after the diagnosis of a life-limiting fetal condition.
Methods
This was a retrospective study of the written documentation of family conferences pertaining to patients followed in the GAI group (a perinatal palliative care group described below) between May 2015 and September 2016.
Inclusion criteria
Participation in at least one family conference with the GAI group and
Delivery at the Hospital das Clinicas da Universidade de Sao Paulo or delivery in another center followed by participation in the postnatal family conference.
Perinatal palliative care group
The GAI group is a perinatal palliative care group that follows families after the prenatal diagnosis of fetal conditions with high mortality. The term GAI refers to Grupo de Apoio Integral à gestantes e familiares de fetos com malformações in Portuguese (in English: support group for pregnant women and families of fetuses with a malformation).
Leuthner's definition was used to evaluate the prognosis and classify it as a certain prognosis (e.g., anencephaly, which will progress to death regardless of artificial life support) or an uncertain prognosis (e.g., severe diaphragmatic hernia, which will result in the initiation of life support, with the progression depending on the neonatal response). 9 Considering that palliative care is indicated soon after diagnosis whenever a life-limiting condition is diagnosed, we defined as eligible for follow-up all families of a fetus with a major life-threatening malformation. 4
The pregnant women carrying a fetus with estimated perinatal mortality >50%, who are followed at our center, are referred to the GAI group. The estimated mortality is defined in a multidisciplinary meeting that includes a maternal-fetal-medicine specialist, a neonatal specialist, and postnatal physicians (according to the fetal condition; e.g., pediatric surgeon, neurosurgeon, or pediatric cardiologist).
Within the period of the study, the GAI group involved one specialist in maternal-fetal care, one neonatologist, one nurse, one psychologist, and one social assistant. All involved medical professionals had expertise in the field of palliative care.
Family conference dynamics
Each conference was held by at least two health care professionals from different specialties using a semiguided model. The researchers who participated in the family conferences (L.S.B., M.A.B.G., G.R.B., T.A.B., and N.B.N.) were female, had knowledge of communication techniques, and had received palliative care training.
The choice of the different providers depended on their expertise in discussing a given issue on the semistructured form used in the conferences, as well as the needs of the patient and her family.
The pregnant woman could choose any person she wanted to be with her during the conference, and there was no limit to the number of people she could bring with her. The father was always encouraged to participate in the conference.
After the conference, the professionals debriefed the conference and discussed their perceptions of the main issues. After reaching a consensus, the main issues presented in the conference were documented in the patient record.
Data analysis
The information contained in the records of the family conferences was evaluated, and qualitative content analysis with an inductive approach (open content analysis) was used. To ensure a high quality qualitative analysis, the guidelines for qualitative reporting by COREQ (Supplementary Data 1) were used. First, 20% of the written documentation was read, and an initial coding system was created, containing the initial categories. Subsequently, the initial coding system was improved by reading all the records and then removing, including and regrouping the categories according to broad themes.14,15
The triangulation process was performed in a multidisciplinary team meeting, during which all team members discussed the themes, categories, and examples. The final themes and categories are shown and discussed below.14,15
Inter-rater and intrarater reliability agreement analyses were performed on a subsample of 20% of the medical records. 16 For the inter-rater reliability analysis, two raters independently entered the previously constructed categories in the coding units. For the intrarater reliability agreement analysis, the same rater categorized the coding units at two different times separated by a month.
Ethics approval
This study was approved by the Ethics Committee with the number 41506915.5.0000.0068.
Results
From 2015 to September 2016, 50 women met the inclusion criteria. Three pregnant women followed prenatally during this period were not included because they gave birth in another center and did not return after delivery.
The mean number of conferences was 4 (min 1; max 8). The partners of 35 (70%) pregnant women participated in at least one of the conferences, and 43 (86%) of the pregnant women had at least one family member present during the conference. Table 1 shows the sociodemographic characteristics of the women included in the study, and Figure 1 shows the types and frequencies of the fetal conditions.
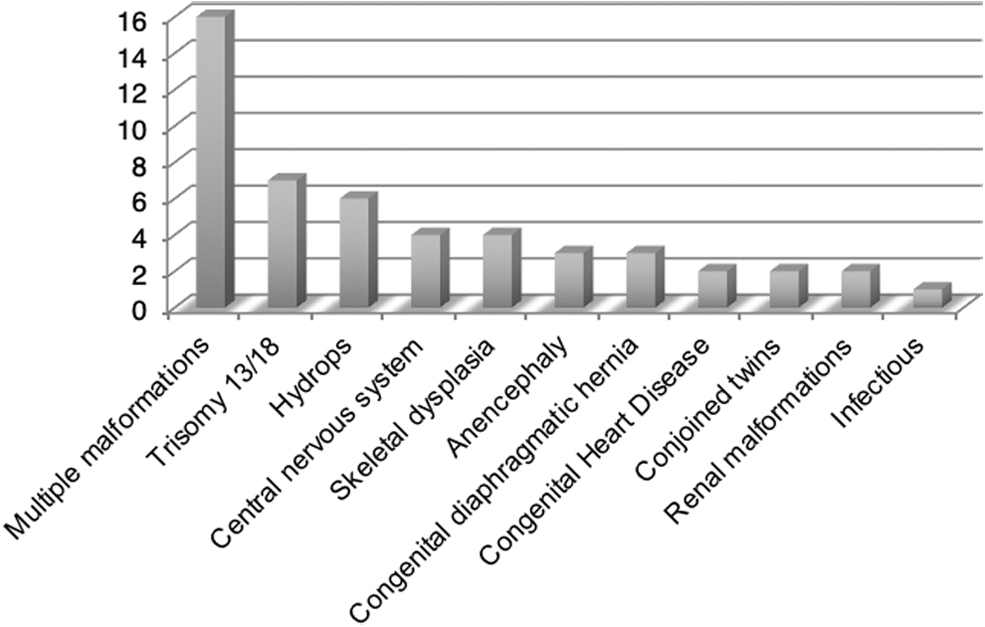
Main fetal conditions of women included in the study.
Baseline Characteristics of Women Followed by the GAI Group from May 2015 to September 2016
A birth plan (generated by the pregnant woman and her family in cooperation with the health team) was formed with 36 families (72%). The birth plan sought to bring together the care goals of the family and the health care proposed for each pregnant woman and her baby. There was a positive relationship between the number of prenatal family conferences and the possibility of jointly constructing a birth plan. Table 2 shows the frequency of birth plan construction stratified by the number of consultations.
Frequency of Birth Plan Construction by Number of Consultations Performed on Pregnant Women Followed at GAI from May 2015 to September 2016
Five main themes emerged from the charts and are described in Table 3.
Main Themes and Categories That Emerged from the Analysis
The interobserver and intraobserver reliability analyses showed excellent levels of agreement (kappa = 0.863 and 0.849, respectively, p < 0.001).
Theme 1: “Talking about the fetal condition”
We observed that the possibility to talk about the fetal condition varied among the families. For some families, it was difficult or impossible to talk about the fetal condition with the health team. Some of the reasons for not wanting to talk about the fetal condition reported in the medical records were the suffering generated by the probable loss of the child, the hope for an incorrect diagnosis, and the desire for a miracle. These were included in category 1.1, “It is hard to talk about it.”
They do not want to talk about the fetal disease (they say they do not want to talk) because ‘everything is going to be alright’.(P2)
Other families wanted to talk about the fetal condition and even sought more information from either our health team or another team (as a second opinion). We also observed that the Internet was often used in the search for more information (Google or Facebook groups of families with children with similar conditions). This was included in category 1.2: “Talking about the fetal disease and searching for information.”
They say that they participate in a Facebook group with parents with the same fetal diagnosis and that it has helped in understanding what will happen after the baby is born. (P17)
Many times, it was hard for families to talk about the fetal condition in the beginning; as more conferences were held, it became progressively easier to talk and organize a birth plan. This is a process that involves family expectations and trust in the health care team, and it may take time for the family to be open to discussing all possible outcomes.
Theme 2: “Understanding the context of the moment”
We observed a need for the health care team to understand all aspects of the familial context to plan the follow-up fetal and neonatal care. Many notes were related to exploring the social, familial, psychological, and spiritual aspects of the family.
There were notes in category 2.1, “Feelings related to the process,” pertaining to the feelings reported by the pregnant women and their partners, such as sadness, suffering due to the possibility of losing the child, and questioning and searching for meaning (e.g., “Why us?”).
The patient, as well as the husband, asks questions about why this is happening to them and states that they are honest, fair people and that they truly wanted the pregnancy. (P50)
Some parents reported guilt. In addition, some notes reported parental concerns about the possibility that the fetus was suffering or would suffer during the process. Preoccupation with the other partner's feelings was also a frequent concern.
Another frequent cause of suffering was “social suffering.” Some notes reported women feeling exposed or uncomfortable when questioned about how the pregnancy was going by strangers in their everyday lives (such as at the market or bus station). Some parents reported feeling like they were lying when they did not talk about the fetal condition to strangers.
In category 2.2, “Family context,” we observed that familial communication may be challenging in the context of the possible death of a child, and some notes pointed to difficulty with effective communication. Other notes reported the possibility of intrafamilial communication and the existence of familial support.
They talk well between themselves and have good contact with family members. They are talking to the grandmothers about the malformations and about the baby being ‘safe in the belly and then being with God.’ (P50)
When there were other children in the family, there were frequent notes related to the other children's feelings. For some families, it was not possible to talk about the fetal condition with the other children, often because they were trying to protect the children from suffering. These notes are in category 2.3, “Other children.”
The pregnant woman informs us that she could not talk about the current pregnancy with the 3 children because she does not want them to suffer. However, she would like to be sincere with them so that everyone can ‘enjoy’ the pregnancy, as well as prepare for all the possible outcomes. (P29)
There were also notes on the health professionals' positions regarding the importance of including the other children in the process and supporting the communication with the other children.
Concerning bonding and the desire for contact, in category 2.4, “Bonding and desire for contact during pregnancy,” we observed that some couples tried not to bond with the baby, believing that bonding would increase their suffering. There were also couples who did not wish to build memories during gestation.
She also refers to caressing her belly and talking to Mary but ‘not too often so she can protect herself.’ (P12)
For other women, bonding was natural and desired, and we observed that many families wanted to participate in pregnancy rituals, such as baby showers.
She reports that she has decided to have a baby shower and wants to donate the diapers to the institution. He also reported that he decided to set up a baby's room, with no set colors, so as not to regret not having prepared for the baby's arrival, even though he knew he would not survive. (P19)
In category 2.5, “Hope and miracles,” we observed that hope was almost always present, and in many families, there was a transformation of hope. In the beginning, there was hope for an incorrect diagnosis that transformed into hope to have contact with the baby or the baby being born alive. In addition, hope for a miracle was frequent.
Right at the beginning, the mother talks about miracles and that they are very keen for a miracle to happen. She affirms that it is now in the hands of God. They understand a miracle to be their daughter being born without any malformations. (P6)
Theme 3: “Preparing Care”
Preparation for birth according to familial values is one of the main objectives of prenatal palliative care. A birth plan in prenatal palliative care is equivalent to anticipated directives in adult palliative care, that is, a document that contains all decisions and values and that guides follow-up by the on-call team.
In the process of discussing birth objectively with the families, there were many descriptions of families' feelings about the proximity of birth. These are included in category 3.1, “Feelings with the proximity of childbirth.” Anxiety due to not knowing the baby's response, fear of childbirth, and familiarity with childbirth was described.
We provided care and talked about the possibility of anesthesia because the patient fears that she might experience pain during childbirth. (P50)
During the process, the possibilities regarding the care of the newborn were discussed. In category 3.2, “Preparing for childbirth and caring for the newborn,” some written documentation described the difficulty of having a conversation with some pregnant women and family members about childbirth and neonatal resuscitation.
I discussed what might happen with each decision (artificial life support or comfort care) (…) and that the goals of care will be centered on the comfort of the newborn and the family. (P12)
We presented the birth plan, and the mother expressed a desire to give birth vaginally and says that she wants monitoring. Why? (I asked) ‘How do we know if the baby is dying if we are not listening to the heart?’ (she asked). (P24)
Category 3.3, “Mementos, contact and rituals,” includes the discussion of mementos, the kind of contact wanted with the child and the rituals that the family might want. There were some notes on women who were worried that they could not predict how they would react to the physical appearance of the newborn (discussing contact). In addition, some notes described women stating that they did not wish to see the apparent aspects of the malformation. Some reported families not knowing if they would like to see and hold their babies after delivery, particularly in cases of fetal death.
She would like to be shown the hands and feet or other parts without visible malformations. She would also like, at the time of delivery, to be asked again if she wants to see the face. In addition, she would like the team to evaluate if it is possible to hold the baby without seeing the face. (P12) (baby with facial malformation)
On the other hand, for some families, it was very important to see the malformation.
The patient wants to see the baby and the malformations. (P23)
The location of care in cases in which artificial life support was not planned (the possibility of caring for the child while the child was held in the laps of the parents or while the child was cuddled) was also discussed with parents.
They spontaneously reported a desire to hold the baby on their laps and see the baby independent of whether it was born alive. They talked about the baby staying in their laps after being born or until the last minutes of life and about caring for the baby in their laps if the baby remains alive. (P18)
Theme 4: “Childbirth and the period after birth”
The notes on how childbirth occurred and caring for the baby in category 4.1, “Notes on labor, delivery and neonatal outcome,” allowed the health team to identify possibilities and difficulties in delivering the planned care.
The baby was born well, with good evolution, better than expected during gestation. (P20)
Parental feelings about the follow-up by the on-call team and positive and negative feelings about labor and delivery were described in category 4.2, “Feelings about labor and delivery.”
She says delivery was different than she had imagined. Her evaluation was that she was very well cared for, and despite the suffering due to knowing that her daughter would not be born alive, she had a good delivery. (P23)
Some reports were of ambiguous feelings, with a mixture of security or tranquility and apprehension regarding the loss.
At the time of delivery, she was quiet (showing trust in the team) but apprehensive of the loss. (P8)
In addition, the kind of contact parents had with the baby was described in category 4.3, “Contact with the baby and rituals.”
The three children were able to see the baby, and the priest performed the baptism, and he kept the baby in his lap for approximately 40 minutes. (P18)
She reports that it was important to have seen the baby because in her imagination he was much uglier physically. She found the baby beautiful, ‘proportional’, and different from what she had imagined. (P35)
Mementos that were kept are discussed in category 4.4, “Mementos.”
She kept his cap and the stamp of his foot; she thought it was very important to have kept it. (P38)
In addition, rituals performed, including burial participation, are described in category 4.5, “Participation in burial and procedures after death.”
The patient attended the funeral, but she preferred that the oldest son not participate. (P42)
Concerning the feelings reported, in some written documentation, there were notes on sadness, suffering, and complicated mourning. In other cases, there were reports of the experience of motherhood or parenthood, even if for a brief period. In addition, there were notes on the future plans of the families. These are all included in category 4.6, “Postnatal feelings and grief.”
The patient reports that she has good days and bad days; she would like to have had more time with the baby, but she also wonders if any other time would have been enough. (P37)
Theme 5: “About the GAI group and the importance of the family conferences”
We observed that talking about the fetal disease and the possibility of the death of a child is very painful. Despite this, many notes were on reflections of the families about how the prenatal follow-up allowed them to live each day at a time with the baby and to think beforehand about seeing and holding the baby. Positive feelings were also identified regarding the possibility of obtaining more information, assistance in communicating with family members, and the possibility of preparing for the future.
He reports that it was very difficult to talk about the choices in relation to the possible death of the babies during pregnancy, and at birth, he realized how important it had been to talk about it before, because ‘everything happens very fast’ and it was good to have thought about the possibilities. (P14)
Discussion
For the first time in the perinatology literature, it was possible to describe the themes present in medical records of family conferences. As reported in this study, there is a wide variety of feelings, causes of suffering, and values reported in family conferences during prenatal palliative care follow-up.
The identification of the main themes that emerged during follow-up enabled the health team to create a framework for approaching the patients and families during prenatal palliative care follow-up and supporting them through the identification of values and the creation of a birth plan during this painful time. This framework, called “ACE of Care,” is composed of five steps; each step needs to be explored before the next step is entered. The Figure 2 shows this proposal of a theoretical model for perinatal palliative care.
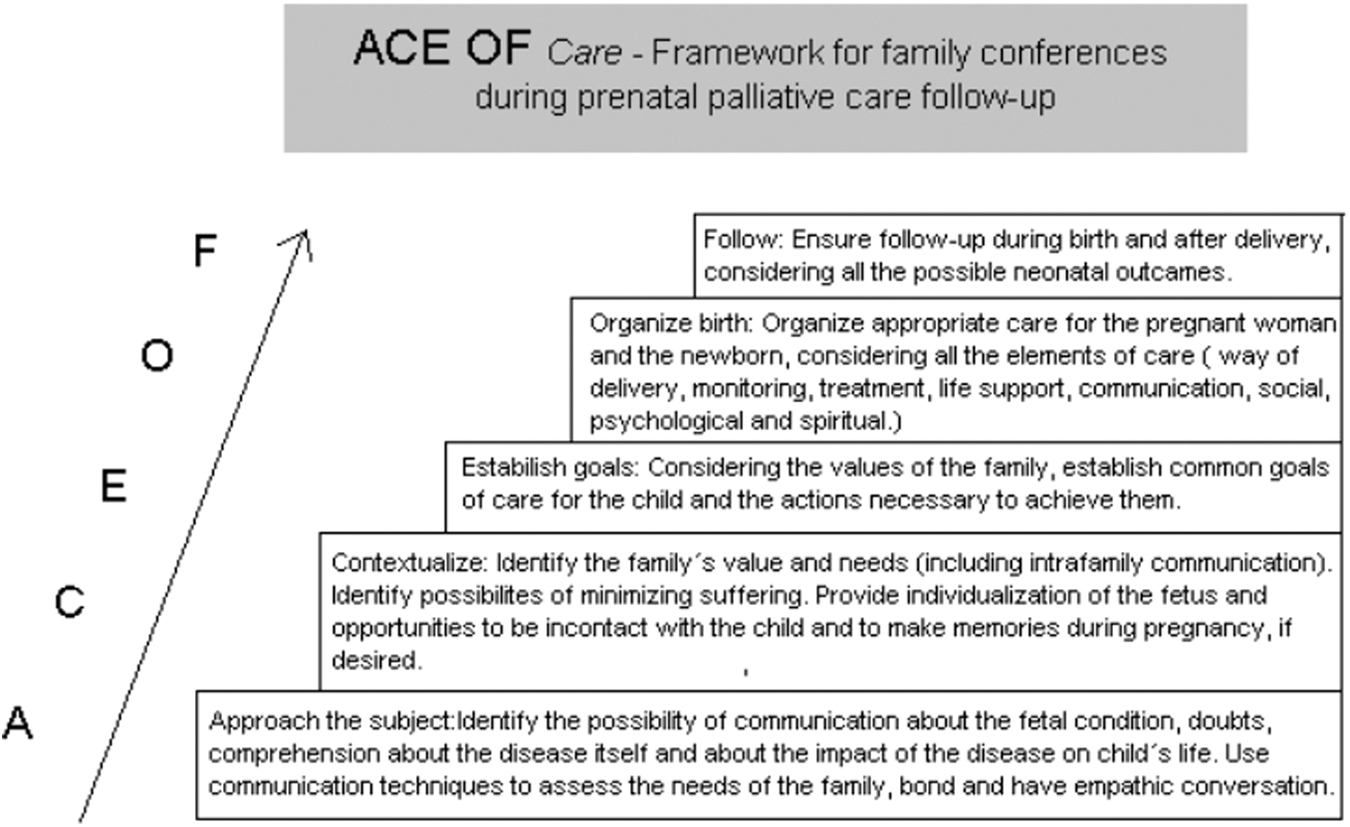
Proposal of a theoretical model for perinatal palliative care.
In this model, the first step (approach the subject) is to obtain knowledge of how the family understands and perceives the fetal condition. It is important for the team to have a clear picture of the familial comprehension of the fetal condition and prognosis. In addition, it is important to evaluate the whole familial situation (considering the physical, psychological, social, familial, and spiritual issues). The second step (contextualize) involves the identification of the family's values and needs, minimizing suffering when possible, and encouraging family and fetal bonding. The third step (establishing goals) is intended to establish the care objectives and the necessary actions. Only when the setting has been fully understood does the preparation for birth occur in the fourth step (organize birth). Finally, in the last step of this framework (follow-up), the team ensures follow-up after birth, in the neonatal period and beyond.
Limitations
The main limitation of the study was the use of a retrospective chart analysis instead of a prospective analysis of recorded conferences. The analysis of recorded conferences in the future may allow for the identification of a larger spectrum of familial needs and reactions during prenatal palliative care. However, because professionals discuss conferences immediately after they take place and try to take extensive notes, the main issues identified by health professionals are present in this study.
Conclusion
The description of a palliative care model is extremely useful for patients who choose to continue their pregnancies, as well as for patients living in countries in which the laws do not allow the termination of pregnancies. In Brazil, pregnancy termination is allowed in cases of anencephaly, risk posed to the life of the mother, and pregnancies resulting from sexual abuse. In other cases with lethal prognoses, termination is allowed after a court order. Pregnancy termination is systematically discussed with parents when it is legally possible.
This analysis and proposal of a framework may guide health professionals to better identify family needs and values and to better organize follow-up during prenatal palliative care for fetuses with life-limiting conditions.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.