
Abstract
Introduction:
Malignant fungating wounds (MFWs), non-healing wounds caused by aggressive proliferation of malignant tumors, afflict 5%–14.5% of patients with advanced cancer. We conducted an integrative review to evaluate the level of evidence of peer-reviewed literature published from 2000 to 2019 on symptoms of MFWs, and the impact of the symptoms on functional performance among patients with advanced cancer.
Methods:
Four electronic databases were searched and 1506 articles were retrieved. A total of 1056 abstracts were screened for relevance and a full review of the 26 articles was performed. A total of 12 articles met inclusion criteria. An established quality assessment tool was used to rate the quality of the included studies.
Results:
The overall quality of the included 12 studies was adequate. This integrative review of the literature provided strong evidence that patients with MFWs suffered multiple symptoms, including pain, odor, exudate, bleeding, pruritus, perceived wound status, perceived bulk effect and lymphedema. Quantitative research was not able to capture the occurrence and characteristics of all the identified symptoms. There was a lack of quantitative research on the impact of MFWs and symptoms on patients' functional performance. Yet, qualitative studies provided vivid description of how the symptoms negatively affected patients' functional performance. Future research should develop a clinical tool that enables the comprehensive assessment of symptoms of MFWs. Well-designed quantitative research is needed to delineate the impact of symptoms of MFWs on patients' functional performance to ensure quality palliative care.
Introduction
Malignant Fungating Wounds (MFWs) generally occur during the last 6–12 months of life among patients with advanced cancer,1,2 that is, when no medical or surgical intervention can control tumor growth.3–5 MFWs are non-healing wounds due to aggressive proliferation and infiltration of malignant tumors into the skin, blood and lymph vessels, leading to widespread tissue damage, hypoxia, necrosis, as well as sustained polymicrobial proliferation and fungating ulceration of the wound. 6 MFWs disproportionately affect older adults and women with MFWs of the breast as the most prevalent (66%), followed by head and neck (24%), then groin, genitals and back (3%) with all other sites accounting for the remaining 8%.7,8 Given the incurable nature of MFWs and severity and numerous symptoms associated with these complex wounds, palliative care is imperative for this population to prevent and relieve suffering through comprehensive assessment and treatment of symptoms of MFWS, preservation and/or restoration of functional performance, and treatment of psychosocial and spiritual distress.12,13
The unique symptom experience of each patient with MFWs can be subjectively reported or objectively measured through the symptom characteristics of timing, intensity, quality, and, distress.14–18 Patients with MFWs may suffer cancer-related symptoms due to the cancer itself or cancer treatment, such as fatigue or cancer-related bone pain, as well as side effects from palliative therapies (e.g., palliative radiation or chemotherapy).6,11,13
However, the symptoms and symptom characteristics specifically attributed to the MFWs (wound pain, malodor, bleeding) are unique to this population.6,13 Research has shown symptoms can negatively impact individual's functional performance in the physical, psychological, social, occupational, and spiritual domains.19–22 Clinicians and researchers have been aware that symptoms associated with MFWs have a detrimental effect on patients' functions, and negatively impact psychosocial well-being (e.g., positive emotions like hope, and life satisfaction).5,6,9,11
Since 2000, more research has documented symptoms associated with MFWs (e.g., pain, malodor, exudate, bleeding, and pruritus) among patients with MFWs.8–11,23–25 This has made it possible to explore the relationships between symptoms of MFWs and the impact on functional performance through systematically reviewing the existing literature.
The purpose of this article is to evaluate the level of evidence of peer-reviewed literature published from 2000 to 2019 on symptoms of MFWs, and the impact of the symptoms on functional performance among patients with advanced cancer. Specifically, this review aimed to answer the following questions: (1) What were the symptoms of MFWs? (2) What were the symptom characteristics of MFW symptoms? (3) What was the impact of symptoms of MFWs on patients' functional performance?
Methods
Preparation for the search
To prepare for the review, a thorough literature search and review was accomplished to generate key search words or terms based on the concept of MFWs, symptoms, functional performance and quality of life (QOL). Subsequently, additional search terms were identified using the MeSH (Medical Subject Heading) database. To ensure the reliability, thoroughness, and accuracy of key searching terms, we had multiple consultations with the health librarian.27,28
The key terms used for this systematic review included: “malignant fungating wound or malignancy or neoplasm or wound and symptoms, quality of life, psychosocial, functional performance, pain or bleeding or pruritus or odor or exudate or bulk effect or lymphedema, depression or anxiety or embarrassment or sexuality or social isolation or stigma.” Using various combinations of the key terms, the following databases were searched: the Excerpta Medical Database (EMBASE), PubMed, the Cumulative Index for Nursing and Allied Health Literature (CINAHL), and Cochrane Library.
Before the integrative review, we defined key concepts based on extensive review of the literature. Symptoms were defined as subjectively perceived indicators of abnormal biological or physiological changes that may or may not be observed or measured objectively.14–17 We defined physiologic bulk effect as a sign of objective, measurable protrusion of the wound and wound dressing beneath a person's clothing or over exposed skin from side and frontal views. 22 While the symptom of perceived bulk effect is the patient's subjective interpretation of how noticeable the protrusion is and the degree to which patients perceive it alters their appearance and causes distress.9,13 Physiologic wound status is the objective, measurable dimensions and characteristics of the wound (e.g., tissue type, wound edges, presence of infection), while perceived wound status is the patient's perceived meaning of the wound's appearance.9,13,22
Functional performance was defined as the ability to perform activities to meet basic needs, fulfill usual roles, and maintain health and well-being. 22 The impact of symptoms on functional performance of patients with MFWs was operationalized in this review as statistically significant associations between symptoms and functional performance items measured in quantitative studies.16,17,22
Inclusion and exclusion criteria
Inclusion criteria for this review were: (1) quantitative and qualitative research on symptoms related to MFWs, and (2) quantitative and qualitative research on functional performance among patients with MFWs. Excluded articles were: (1) any research that focused on other types of wounds, such as pressure ulcers, venous ulcers, and Marjolin's ulcers, (2) any research that focused on microbiome or interventional research, including invasive or topical therapies, (3) individual case studies, and (4) unpublished dissertations and abstracts. 26
Data extraction
In total, 1506 articles were retrieved by applying the key terms to the four databased, after removal of 450 duplicates, 1, 056 articles remained. Inclusion and exclusion criteria were applied to the 1056 articles through a review of the abstracts, 26 articles were deemed relevant. Upon a full-text review of the 26 articles, only 12 articles met inclusion criteria, resulting in five quantitative and seven qualitative studies for this review (Fig. 1).
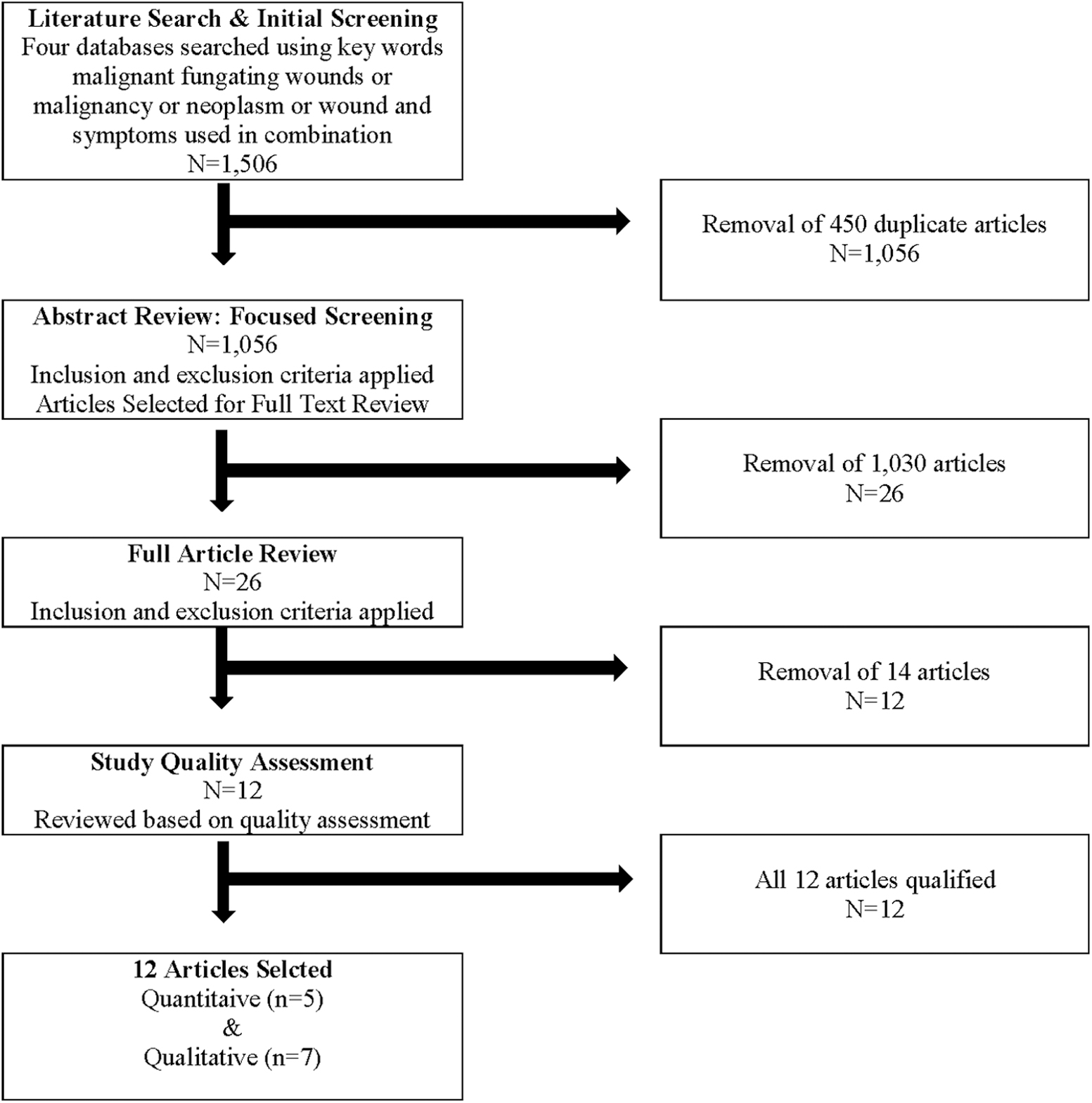
Literature search flow chart. Symptoms of malignant fungating wounds and their impact on functional performance of patients with advanced cancer: an integrative review from 2000 to 2019.
An adapted quality assessment tool using a 14-item index was used to evaluate the quality of the 5 quantitative and 7 qualitative studies identified.27,28 For this integrative review, studies that received an affirmative score of at least 10 out of 14 were considered to have adequate quality.27,28 All 12 articles were deemed adequate and included in this review (Table 1).
Results of Quality Assessment Scores
SD, standard deviation.
Data analysis
Detailed critical appraisal of each included article was performed using an adaptation of the Critical Appraisal Skills Programme (CASP) method.28,29 Using the CASP method, we accomplished data analysis (Table 2).26,30 After completing the evaluation of the 12 articles by the authors, the authors achieved consensus by discussing the results and resolving any discrepancies. A metasynthesis was conducted for the qualitative studies to identify emerging themes regarding the symptoms of MFWs and functional performance as well as descriptors for symptom characteristics (Tables 3–5).26,30
Quantitative Studies of Symptoms of Malignant Fungating Wounds
BWAT, Bates-Jensen Wound Assessment Tool; CVI; ECOG PS, Eastern Cooperative Oncology Group performance status; GU/GYN, genitourinary/gynecologic; MAD, moisture-associated dermatitis; MASD, moisture-associated skin damage; MFW, malignant fungating wounds; MFWAT, Malignant Fungating Wound Assessment Tool; MQOL-TW, McGill QOL questionnaire Taiwanese version; MWAT-R, Malignant Wound Assessment Tool for Research; NR, not recorded; QOL, quality of life; QS, quality score; RT, retention time; SF-MPQ, Short form McGill Pain Questionnaire; SSD, silver sulfadiazine.
Qualitative Studies of Symptoms of Malignant Fungating Wounds
Malignant Fungating Wound Symptom Descriptions by Patients from Qualitative Studies
Qualitative Themes: Symptoms and Symptom Characteristics
Results
Quality of the included studies
The overall quality of the 12 studies was adequate (mean = 11.58 ± 0.9, range from 10 to 13). The total population of all quantitative studies was 215 (mean = 43 ± 23.6, range from 22 to 70) and qualitative studies 65 (mean = 9.28 ± 4.5, range from 3 to 17). Detailed information regarding the quality of studies are presented in Table 1.
Sample characteristics
Consistent with the incidence of MFWs, this review also found that majority of study samples were women, older adults, and MFWs of the breast. The majority of the 215 participants in the quantitative studies were women (n = 135) and older adults (age >50 years). Three quantitative studies exclusively had women with breast MFWs,32–34 one had a predominance of male subjects with MFWs of the head and neck, 35 and one study had an equal number of male (n = 34) and female (n = 33) participants with mixed MFW etiologies. 36 None of the studies included MFWs from genitourinary cancers. The 7 qualitative studies included 65 participants. The majority of participants were older female (92%), and 94% of participants had MFWs of the breast.37–42
Symptoms of MFWs
Quantitative studies investigated symptoms related to MFWs in terms of symptom occurrence or prevalence of pain, malodor, exudate, bleeding, pruritus, and perceived bulk effect; yet no research investigate symptom occurrence of perceived wound status or lymphedema.31,33,35,41 One qualitative study identified lymphedema and four qualitative studies perceived wound status (wound appearance) as distressing symptoms related to MFWs.36–38,41,42 None of the studies captured all eight reported symptoms of MFWs.
Symptom characteristics of MFWs
While quantitative research did not fully capture the characteristics of symptoms of MFWs, qualitative research provided rich descriptions of symptom characteristics (Table 4) in terms of timing, intensity, quality, and distress (Table 5).
Pain
Pain was the most frequently occurred symptom in patients with MFWs, ranging from 31.3% to 77.3%.33,35 Pain occurrence was examined in terms of temporal characteristics: pain occurred in association with dressing changes; pain occurred either with (cyclic) or between (chronic) wound care or dressing changes. 34 Two studies found significant temporal associations between cyclic pain and wound care: fewer wound dressing changes were correlated with lower pain scores ([r = −0.274, p = 0.043]; 34 [r = −0.428, p = 0.047] 33 ). Pain duration was measured in two studies.33,34 One study found continuous pain in 40.9% of patients with MFWs of the breast. 33
Pain control was measured on an ordinal scale in only one study and found partially controlled to non-controlled pain ranged from 30% to 10%. 31 Three different psychometric instruments were used to measure pain severity (intensity); the Verbal Rating Scale (none, slight, moderate, strong, intense), 31 the Short Form-McGill Pain Questionnaire (SF-MPQ), 33 and the Malignant Fungating Wound Assessment Tool (MFWAT-P). 34 Pain intensity ranged from mild (50%–56%), to moderate (12%–27.3%), to severe (7%–19%).31,33 Pain quality was measured in two quantitative studies utilizing the instrument of SF-MPQ and MFWAT-P and the most commonly occurring descriptors were “throbbing,” “shooting,” and “stabbing.”33,34 Qualitative studies described pain quality as “stabbing,” “shooting,” and “bursting,” with intensity ranging from mild to severe (“terrible”).36,40,41
Malodor
Malodor occurred in 11.9% of patients with MFWs. 31 Malodor intensity ranged from slight (27%–50%), to moderate (25%–34%), to intense (0%–8%). 35 Qualitative studies described the quality of malodor as “garbage,” “rotting flesh,” “putrid,” and “moldy.”36,41,42 Participants in one study likened the smell of the MFWs to a “cadaver.” 41 Malodor is pervasive, caregivers recall altering their breathing patterns to avoid the smell and having vivid memories decades later. 42
Exudate
Exudate occurrence was 17.9% in patients with MFWs, 35 and exudate intensity ranged from slight (16%–31%), to moderate (61%–75%), to intense (8%–12%). 31 Quality of exudates ranged from serous to purulent,32,35 and amounts from small to moderate or large,32,35 with the latter variable significantly associated with periwound moisture-associated skin damage (χ 2 = 4.41, p = 0.066). 32 Five qualitative studies identified exudate as one of the most challenging and distressing symptoms to manage.36,37,39–41 Four qualitative studies described the feelings of shame and embarrassment due to exudate in patients with MFWs.36,39,40,42 The negative emotions elicited by exudate undermined self-confidence and contributed to social isolation.36,39,40,42
Bleeding
The occurrence of bleeding was 6% among patients with MFWs. 35 Intensity of spontaneous bleeding ranged from slight (3%–8%), to moderate (5%–10%), to intense (0%–11%). 31 Intensity of induced bleeding ranged from slight (47%–60%), to moderate (12%–24%), to intense (0%–6%). 31 Four qualitative studies described challenging personal accounts of bleeding associated with MFWs.36,38–40 One woman recalled spontaneous bleeding during a work meeting, necessitating an impromptu clothing change. 40 Another spoke of bleeding after each dressing change and with “slight exercise,” necessitating constant dressing changes. 36 Bleeding led to uncertainty, lack of confidence, lack of control, avoidance of favorite pastimes, social isolation and feelings of impending death.36,38–40
Pruritis
One quantitative study identified the prevalence of pruritus as 5.2%. 35 Pruritus intensity and quality was not investigated in quantitative studies, yet qualitative studies described pruritus as being extremely distressful, “…I can tell you I would scratch day and night.” 40
Perceived bulk effect and wound status
Only one quantitative study reported that 24% of patients with MFWs had perceived bulk effect that elicited negative emotions. 35 Five qualitative studies found that perceived wound status as a body disfigurement from the MFWs negatively impacted body image and self-esteem,36–38,41,42 leading to grief and loss of normalcy.37,42 Three qualitative studies found that perceived bulk effect and wound status had a negative impact on femininity and sexuality.36,37,40 Women reported a change in their body image (low self-esteem) and an inability to wear feminine clothes and a bra due to the bulk effect of dressings, leading to social avoidance.37,40 Five studies found MFW appearance was a constant reminder of advanced and incurable disease, robbing patients of hope36,38,40–42 “…this wound looks as if death is more and more near me. I can't escape….” 36
Lymphedema
None of the quantitative studies identified lymphedema as a symptom of MFWs nor recorded its prevalence, intensity, or quality. One qualitative study described the distressful experience of a woman with a breast MFW and lymphedema. 41 Lymphedema is known to have negative psychological and social impact on patients. 27 The participant with upper extremity lymphedema reported a sense of compromised normalcy, forcing her into isolation. 41
Impact of symptoms on overall QOL and functional performance
Only one quantitative study examined the relationship between symptoms of MFWs assessed by the MFWAT and overall QOL measured by the McGill QOL questionnaire, however subscales were not reported. 34 This study found that number of symptoms per patient (r = −0.479, p = 0.049), pain (r = −0.479, p < 0.001), malodor (r = −0.293, p = 0.014), and bleeding (r = −0.280, p = 0.035) were correlated with poor overall QOL. 34 Several qualitative studies reported that malodor was the most distressing symptom to patients and caregivers.36,38,39,40,41,42
None of the quantitative studies specifically investigated the impact of MFWs or symptoms of MFWs on functional performance, including dimensions of physical mobility, activities of daily living, participation in social activities. Qualitative studies provided rich data describing the devastating impact symptoms of MFWs on physical mobility, ability to perform activities of daily living, social interactions, and ability to work and participate in usual pastimes.36–42 Table 6 summarizes the themes related to symptoms of MFWs and adverse impact of the symptoms on functional performance in the physical, social, occupational and psychological domains.
Qualitative Themes: Impact of Malignant Fungating Wound Symptoms on Functional Performance
ADLs, activities of daily living.
Discussion
This integrative review of the literature provided strong evidence that patients with MFWs suffered multiple symptoms, such as pain, odor, exudate, bleeding, pruritus, perceived wound status, perceived bulk effect and lymphedema. The major limitation of the quantitative studies was that none of the symptom measures used was able to capture the occurrence and characteristics of the totality of the identified symptoms of MFWs. The occurrence of perceived wound status and lymphedema as well as the intensity of pruritus, perceived bulk effect, perceived wound status, and lymphedema were not evaluated. Future research should focus on developing a clinical measure that is able to capture all the identified symptoms of MFWs as well as to assess that characteristics of the symptoms in terms of quality, intensity and duration. Interestingly, both quantitative and qualitative studies provided rich descriptors of pain, including nociceptive and neuropathic descriptors, to describe pain quality, such as “throbbing,” “shooting,” “stabbing,” and “bursting.” 33–34,36,40–41 This may indicate that pain related to MFWs has a mixed etiology. Future research should investigate the etiology of pain related to MFWs.
Qualitative studies have described intense, negative psychological effects from symptoms of MFWs, including; feelings of shame and embarrassment,8, 36,37,41 negative body image and self-esteem,8,36,37,38,40 and loss of femininity and sexuality.36,37,40 These negative emotions undermined self-confidence, invoked anxiety and depression, and contributed to social isolation.36,37,38,41 However, while qualitative studies did provide vivid descriptions regarding the negative impact of symptoms of MFWs on patients' functional performance and psychological well-being, this integrative review revealed a lack quantitative examination on the impact of symptoms of MFWs on functional performance or psychological symptoms.31–35 Such significant gaps have impeded our understanding of symptoms of MFWs on functional performance impairment and QOL to ensure quality palliative care.
Strengths of the review and limitations of current literature
The strength of this literature review is its focus on the symptoms of MFWs in patients with advanced cancer and its quality review process.27,28 Additionally, to limit selection bias, a broad inclusion criteria was established, and a variety of search strategies incorporating multiple data bases was utilized. 26
This review revealed that a variety of instruments were used to measure the symptoms and symptom characteristics associated with MFWs, however none of the tools was able to capture the full spectrum of symptoms identified in the literature.31–35 There was an absence of quantitative research examining the impact of symptoms of MFWs on functional performance to ensure quality of palliative care for this population.31–35
Limitations of the review
The heterogeneity of using different tools to assess MFWs and symptoms in the included quantitative studies limited the ability of the review for a formal meta-analysis. Additionally, the overwhelming majority of female participants, older adults, and participants with MFWs of the breast made generalizability of review findings to other populations impractical.
Conclusion
This review provided strong evidence that patients with MFWs suffer many symptoms, including, pain, malodor, exudate, bleeding, pruritus, perceived wound status, perceived bulk effect and lymphedema. Qualitative studies provided vivid description of the impact of symptoms on patients' functional performance. Methodologically rigorous quantitative studies are needed to comprehensively examine the symptoms of MFWs in terms of symptom occurrence, characteristics, and impact on functional performance. Development of a psychometric tool that is able comprehensively measures MFWs symptom occurrence, characteristics, and impact on functional performance is needed to assist researchers and clinicians to ensure quality palliative care among patients with advanced cancer.
Footnotes
Funding Information
Thank you to the American Cancer Society (ACS) DSCN-18-214-01-SCN.
Author Disclosure Statement
No competing financial interests exist.