
Abstract

As left ventricular assist device (LVAD) technology continues to offer longer and better lives to patients with advanced heart failure, it also redefines how these patients die. This evolving dying process is unfamiliar to many clinicians and can be distressing for patients and their caregivers. No element of this process is more visceral or immediate than the act of withdrawing LVAD support, particularly for a patient who is awake and interactive. Despite ongoing improvement in survival and functional outcomes, LVAD patients frequently experience deaths characterized by distress, confusion, and a lack of control that fail to meet many of the criteria for high-quality end-of-life care. 1
The most recent centrifugal flow LVADs have resulted in 2-year survival >85%, as well as improvements in functional status and quality of life.2,3 Yet, LVADs also cause devastating complications, most notably stroke, bleeding, right ventricular failure, and serious infection. 4 Furthermore, the majority of patients receiving LVADs are now transplant ineligible due to comorbidity and advanced age, which may additionally complicate quality of life and survival after LVAD implantation.
Achieving the right balance between optimizing survival, symptom management, spiritual well-being, and existential concerns at the end of life is a challenge for patients with LVADs and their caregivers. Despite symptom burden and limited prognosis, palliative care involvement and hospice utilization remain low for patients with LVADs, even when compared with the general heart failure population. 5 Caregivers express fear, confusion, and a sense of abandonment surrounding the end of life. 6 It is within this complex context that the question of LVAD withdrawal arises, often following a devastating event or when an LVAD is no longer supporting an acceptable quality of life.
In the October issue of the Journal of Palliative Medicine, Nakagawa and colleagues offer novel insight into the circumstances and decision-making process that precedes LVAD deactivation. 7 They studied 62 patients at a single academic medical center who had LVAD support withdrawn. Specifically, they used the time between initiating a conversation about withdrawal and the actual LVAD deactivation as a surrogate measure for complexity of decision making. In 14 cases (23%), the patients had the decision-making capacity to initiate the conversation about LVAD withdrawal themselves, whereas the remainder of deactivations were initiated by the clinicians or caregivers because the patient lacked capacity. The majority of deactivations (82.3%) occurred while the patient was critically ill in the intensive care unit (ICU). The authors found that the time to LVAD withdrawal was significantly longer for patients outside the ICU and for patients who had capacity to participate in these conversations themselves.
The study deepens our understanding of current LVAD withdrawal as a highly variable and dynamic process with substantial implications for patients' care at the end of life. The challenges inherent to this process can be divided into three categories: ethical, psychological/existential, and logistical.
Ethical Considerations
The ethics of LVAD withdrawal are generally agreed upon within most centers in the United States. 8 The general consensus is that LVAD deactivation parallels the withdrawal of other life-sustaining interventions, such as withdrawing mechanical ventilation in end-stage lung disease patients. 9 A small minority, however, argue that LVAD deactivation is equivalent to euthanasia or physician-assisted death, unless the patient is imminently dying of irreversible LVAD dysfunction or a pathophysiologic mechanism other than left ventricular failure. 10 The tension between these two perspectives might partially explain why so few patients had withdrawal outside of the ICU, and why those who presumably required no additional forms of life-sustaining technology had a significantly longer process of LVAD withdrawal. Among these patients, for example, those whose reason for LVAD withdrawal was “debility,” all went >40 days before LVAD deactivation, compared with only 2 days for the one patient whose reason for withdrawal was “cancer.” Notably, however, ethics consults were not common in the cohort of patients studied (n = 5).
Although it is important to obtain ethical clarity among members of an LVAD team, extended conversations may actually be a disservice to patients who are suffering from severe progressive illness. Protracted deliberation about points, such as those already discussed, risks prolongation of an already unacceptable disease state. In our experience, the general consensus that considers LVAD withdrawal similar to other forms of life-sustaining interventions allows clinicians to honor the wishes of those patients who express a clear preference for withdrawal of LVAD support.
Psychological/Existential Considerations
Addressing the psychological, existential, and interpersonal elements of LVAD withdrawal deserves substantial investment. This applies to the experiences of patients, their caregivers, and clinicians.
Patients with depression and anxiety raise a unique set of challenges with regard to LVAD withdrawal. Although Nakagawa and colleagues do not report rates of depression in their cohort, the authors do comment that some of the most complex and prolonged cases involved patients with depression. The question of decision-making capacity often arises when a patient with psychiatric illness requests LVAD withdrawal, yet depression is common among patients with severe chronic illness and may not be a separate treatable entity that can be removed from the equation. Further studies on experiences of LVAD withdrawal including rates of depression and psychiatric consultation could further inform our understanding of their impact on the LVAD withdrawal process.
Complementary to psychiatry, palliative care is designed to provide important expertise in illness coping and existential questions that arise near the end of life. For patients and caregivers alike, palliative care specialists can provide valuable assistance in decision making and coping, as well as preparation for the end of life. If there is disagreement within a family, palliative care can help to clarify goals and values. Moreover, palliative care expertise is often helpful for orienting the primary team to the dying process in ways that mitigate the moral distress that might accompany an LVAD withdrawal. In our experience, palliative care involvement improves the LVAD deactivation process for all involved, even when patients themselves are not conscious. In this study by Nakagawa and colleagues, however, palliative care was consulted in 60% of cases when the patient was incapacitated, compared with 93% of cases when the patient had capacity. Given the long time to deactivation for patients with capacity who request it, palliative care consultation in its current form may be insufficient to address many of the challenges patients and caregivers face when considering LVAD deactivation.
Logistical Considerations
Perhaps the death of a patient with an LVAD is most substantially different from other deaths with regard to the logistics required for elegant and compassionate device deactivation. Carefully orchestrated logistics can dramatically improve the experience, whereas unfamiliarity and discomfort with the process can create delay and unintended suffering. Before withdrawal, it is essential to communicate the plan with all elements of the patient's care team across disciplines to assure smooth coordination of logistics and for the sake of clinicians' own well-being. Interdisciplinary checklists can support these efforts. 11 Training for frontline clinicians in the various LVAD devices and consoles is necessary as the deactivation processes differ and error can result in alarms that are highly distressing. It is also necessary to decide who will be present, including family and caregivers. With appropriate counseling, for example, a patients' close relations may benefit from being present for LVAD deactivation, similar to how family presence during cardiopulmonary resuscitation (CPR) can result in lower rates of post-traumatic stress disorder. 12 Comfort-directed medications should be delivered as boluses, rather than drips, before deactivation given the possibility that circulation may cease precipitously. Afterward, it is helpful to conduct a debrief with staff and family. The coordination of these logistics is assisted by checklists or frameworks (Fig. 1).
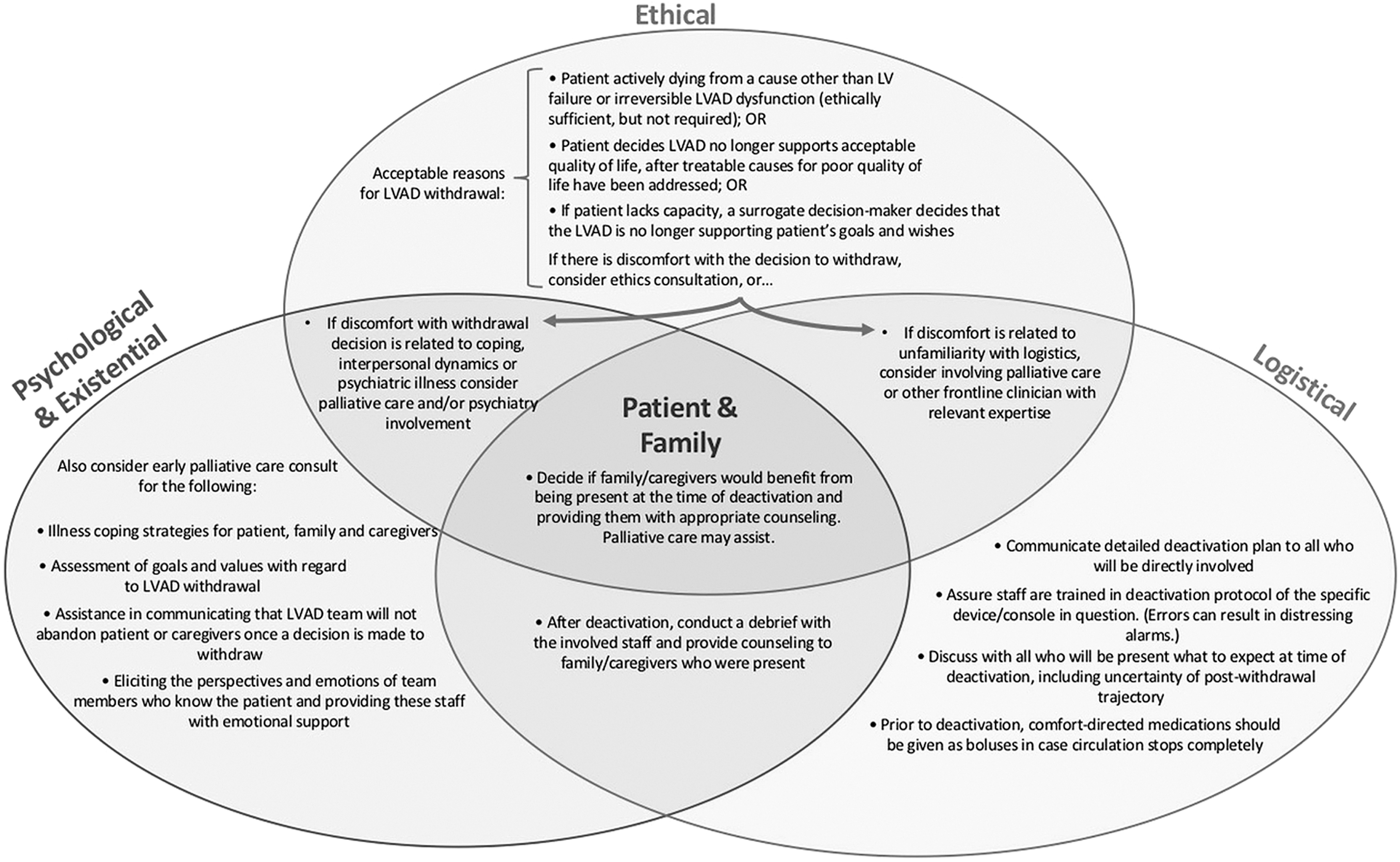
Ethical, psychological, and logistical challenges arising when LVAD withdrawal is considered. LVAD, left ventricular assist device.
Finally, many patients with LVADs would be appropriate for transition to hospice, yet hospice providers are often unfamiliar with the logistics of LVAD management and, therefore, unable to accept these patients. The lack of hospice options may partially explain why so many patients continue aggressive measures in the hospital setting until they are incapacitated before LVAD withdrawal. Increasing the ability of both inpatient and home hospice to accept LVAD patients could change the nature of dying with an LVAD by giving these patients the option to choose a more comfort-oriented approach earlier in the illness trajectory with time for patients and families to plan for withdrawal together.
Conclusion
Offering LVAD patients the possibility of a death on their own terms will require an intentioned approach integrating ethical clarity, psychological and existential sensitivity, and logistical finesse. Practically, this will mean (1) early resolution of ethical concerns to avoid prolonged suffering; (2) improved understanding of how best to involve palliative care, psychiatry, and ethics consultants; and (3) intensified training for frontline clinicians, including hospice providers, in the logistical mastery needed to support patients, caregivers, and medical staff through an elegant withdrawal of LVAD support.
Author Disclosure Statement
No competing financial interests exist.