
Abstract
Background:
When the suffering of a terminally ill patient is intolerable and refractory, sedatives are sometimes used for symptom relief.
Objective:
To describe the main principles of revised Japanese clinical guidelines about palliative sedation therapy.
Design:
Consensus methods using the Delphi technique were used.
Results:
The main principles of the guidelines that were newly defined or developed are as follows: (1) palliative sedation was defined as “administration of sedatives for the purpose of alleviating refractory suffering” (excluding the aim of reducing patient consciousness); (2) palliative sedation was classified according to the method of administration of sedatives: respite sedation versus continuous sedation (including (continuous) proportional sedation and continuous deep sedation); (3) a description of state-of-the-art recommended treatments for difficult symptoms such as delirium, dyspnea, and pain before the symptom was determined as refractory was included; (4) the principle of proportionality was newly defined from an ethical point of view; and (5) families' consent was regarded as being desirable (mandatory in the previous version).
Conclusions:
We described the main principles of revised Japanese clinical guidelines about palliative sedation therapy. Further consensus building is necessary.
Introduction
Terminally ill patients with cancer often develop distressing symptoms that are sometimes refractory to standard palliative treatment.1–4 Palliative sedation is one of the therapeutic options for such intolerable suffering. The major target symptoms include delirium, dyspnea, and pain.1–4 Psycho-existential suffering, although uncommon as a sole target symptom, might also become refractory.1–4
The Japanese Society of Palliative Medicine initially developed clinical guidelines in 2005, with a special focus on continuous deep sedation. 5 In this decade, there has been much discussion on palliative sedation,6–12 and we aimed to integrate recent national and international debates in this revision with newly defined palliative sedation therapy and a description of comprehensive responses for refractory symptoms, including state-of-the-art recommended clinical practices.
First, the concept of sedation was introduced from the 1990s by many authorities,6,13–15 and thereafter, academic associations worldwide clarified the definitions with some variations in the 2000s.5,16–25 Common definitions include a statement that the patient's consciousness is intentionally reduced,5,16–25 but there is no consensus on how to measure the physician's intent, and theoretically, we cannot confirm whether the loss of consciousness is a result of the treatment or disease progression26,27; this leads to inconsistencies in empirical studies about which practices are actually palliative sedation.7–9 To clarify the definition, we aimed to exclude the physician's intent from the definition of palliative sedation in this revision.
Second, continuous deep sedation has been regarded as one type of palliative sedation,5,15–25 but it has recently become a focus of debate.7–10 Recent conceptual and empirical studies suggest that there are potentially two different types of “continuous deep sedation” worldwide11,12,28,29: (1) sedatives are progressively increased according to the level of symptom palliation achieved, resulting in unconsciousness in some cases, but retention of the ability to communicate in others; and (2) sedatives are rapidly increased until the patient is unresponsive and then they are maintained at that level until death. We thus aimed to reflect this concept in this revision.
Third, palliative sedation is just one of the options for refractory suffering, and how to respond to such suffering comprehensively is more important. Therefore, we aimed to discuss not only palliative sedation but also general approach to suffering if suspected as being refractory.
The purpose of this report is thus to describe the main principles of revised Japanese clinical guidelines about palliative sedation therapy: the definition and classification of palliative sedation, management of symptoms when suffering is suspected to be refractory, and the principle of proportionality. The original report in Japanese includes the results of a literature review, and examples of communication with patients and families in addition to complete references.
Materials and Methods
The guidelines aim to help clinicians who adequately manage difficult symptoms and ensure better quality care for terminally ill patients. The target population is adult patients with incurable cancer. The targeted users are health care professionals who treat the target population.
Development process
Twenty members of the task force were selected from national distinguished experts and consisted of 11 palliative care physicians, 3 nurses, 3 bioethicists, a psychiatrist, an anesthesiologist, and a lawyer. As the evidence levels of the majority of the articles were low,1–4 we used the Delphi technique so that task force members could arrive at a consensus to revise the guidelines. 30
First, the task force performed a systematic literature search regarding 9 research questions using the database (i.e., PubMed and Cochrane Library) in English, and shared the results and discussed issues to be revised in a face-to-face meeting. Then, one-panel member (T.M.) developed the whole part of an initial draft based on the literature findings and discussed contents.
Second, the draft was divided into 147 parts according to the paragraphs or group of contents, and panel members were independently requested to rate the validity of each part on a 9-point Likert-type scale from 1 (not appropriate) to 9 (appropriate). We defined that attainment of consensus was achieved for a median value of 8 or more and a difference between the minimum and maximum ratings of less than 6 for each part.
In the first Delphi round, the median value was 8 or higher for all parts, but the difference between the minimum and maximum was 6 or higher for 20 parts. The median, minimum, and maximum values were disclosed to each member, and the differences in opinions were discussed and resolved in a face-to-face meeting. After that, the same one-panel member minorly revised the draft intending to attain the consensus of all panel members.
In the second Delphi round, the median value was 8 or higher for all parts, but the difference between the minimum and maximum was 6 or higher for 11 parts. We held a face-to-face meeting again and confirmed that the major difference had been resolved; we determined that attainment of consensus was achieved for the whole part of the draft.
Finally, 16 external reviewers (3 pain specialists, 2 oncologists, 2 palliative care specialists, 2 psychiatrists, 3 home practice physicians, 2 nurses, a surgeon, and a pharmacist), and 2 end-users reviewed the provisional version and provided free-form comments. After dissemination of the comments to all members, we discussed each section and adopted this as the final version.
Results
Definitions
Palliative sedation
Palliative sedation is defined as “administration of sedatives for the purpose of alleviating refractory suffering.” It does not depend on whether the physician intends to reduce the patient's consciousness. To clarify the sedatives, the task force provisionally listed specific drug names, that is, midazolam and other benzodiazepines and barbiturates. We had no recommendation to define whether the use of levomepromazine and chlorpromazine is palliative sedation because they are infrequently used for palliative sedation in Japan: midazolam is the most commonly prescribed drug worldwide.1,2,4,17,31 We clarified that if the patient's level of consciousness decreases after increasing the optimal dose of opioids for pain and dyspnea, it is not regarded as palliative sedation.
While we excluded the physician's intent from the definition, we agreed that it is indispensable as a requirement for palliative sedation (Table 1).
Ethical Criterions for Continuous Sedation
Classifications of palliative sedation
Palliative sedation is classified according to the method of administration of sedatives into two categories: respite sedation versus continuous sedation; and the latter is classified into (continuous) proportional sedation and continuous deep sedation.
Respite sedation is defined as the intermittent use of sedatives for a predetermined period of time to give the patient respite from intractable refractory suffering. This can be called intermittent sedation.
The concepts of proportional versus continuous deep sedation are presented in Figure 1. We decided not to use the classification according to the degree of sedation, for example, mild or deep sedation, because it is unclear whether the degree of sedation reflects the purpose or result of the intervention.
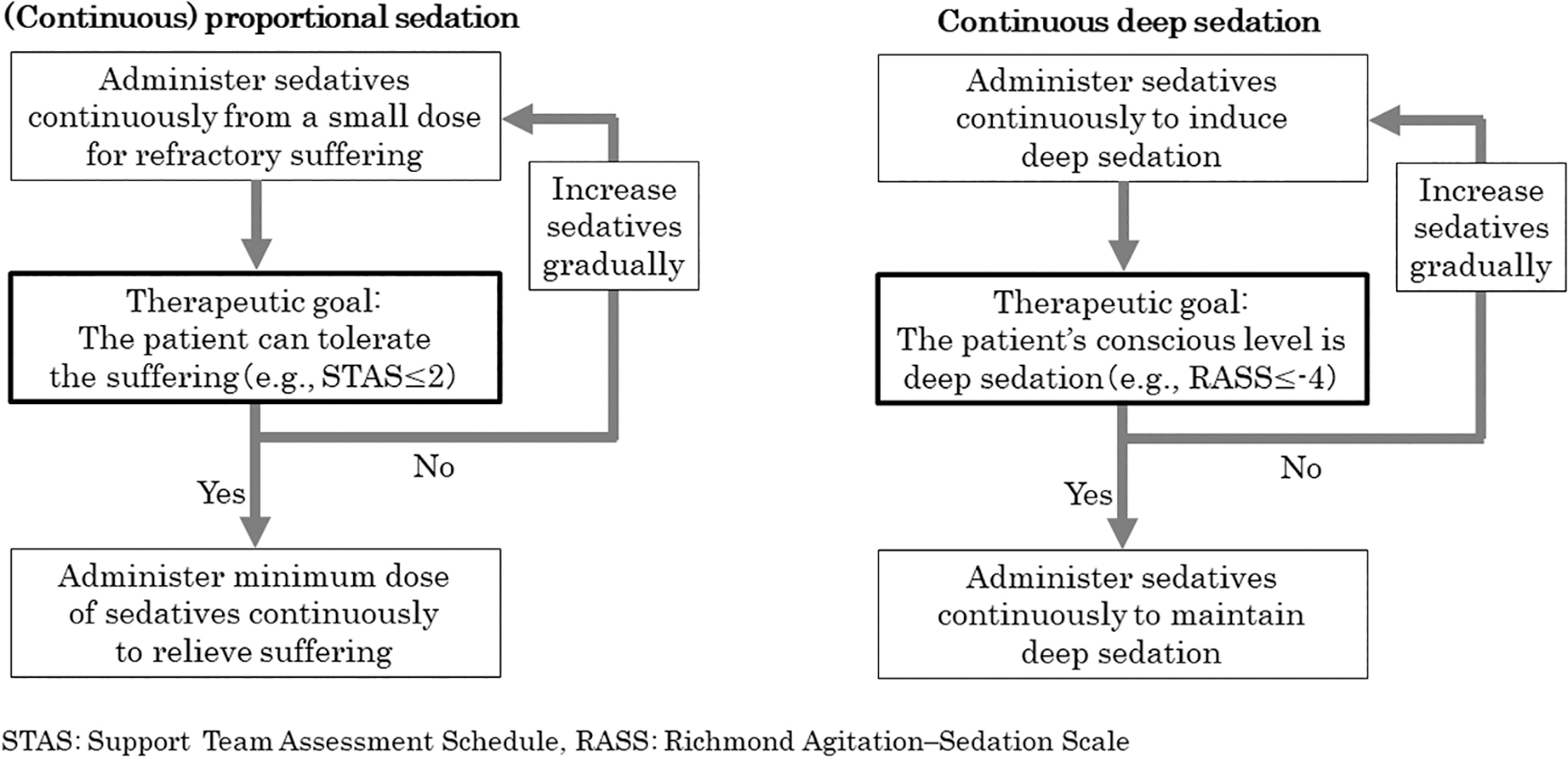
Contents of continuous proportional sedation versus deep sedation. RASS, Richmond Agitation-Sedation Scale; STAS, Support Team Assessment Schedule.
Proportional sedation is increasing sedatives from a small dose to a minimal dose necessary to provide adequate palliation of suffering. The criterion for adjusting the dosage of sedatives is not the level of the patient's consciousness, but the degree of suffering. As a result, suffering may be alleviated in a state whereby the patient's consciousness is maintained; and in the case of overwhelming suffering, it may be alleviated only when the patient's consciousness is decreased. The measurement tool for adjusting the dose is a symptom assessment tool, such as item two of the Support Team Assessment Schedule.
Continuous deep sedation is sedation whereby a reduced level of consciousness is maintained without specifying plans to discontinue. The criterion for adjusting the dosage of sedatives is the level of the patient's consciousness. The measurement tool for adjusting the dose is the Richmond Agitation-Sedation Scale, referring to −4 (deep sedation) to −5 (unarousable).
The term “until death” is not included in the definition, because the task force agreed that it is inappropriate that the physician explicitly states their intent at the time of starting palliative sedation to maintain deep sedation until death. It is reasonable to consider that if the deep sedation is discontinued, the patient's suffering will recur; therefore, maintaining continuous deep sedation with regular evaluation is maintained until death as a result. Continuous deep sedation may be discontinued in some patients due to recovery from the underlying etiology. This is the rationale for the definition to include: “without specifying plans to discontinue.”
As alleviating suffering with maintained consciousness is generally preferable, proportional sedation should be applied first. Continuous deep sedation may be selected first in specific circumstances whereby the suffering is overwhelming and refractory, death is predicted to occur within several hours or days, the patient's wish is explicit, and the suffering will not be palliated by proportional sedation.
Refractory suffering
Suffering is defined as refractory (1) when all treatments have failed or (2) when, based on the patient's wishes and physical conditions, there are no other methods that will be effective within the allowed time frame, and the possibility of complications and degree of invasion are tolerable for the patient.
Intolerable suffering
Suffering is defined as intolerable (1) when the patient describes it as intolerable or (2), if impossible, when the family and the care team sufficiently assume that the suffering is intolerable for the patient based on his/her values. In principle, intolerable suffering includes both physical and psycho-existential suffering.
Criteria for requirements of palliative sedation
Palliative sedation is ethically justified in the contexts of proportionality, patient autonomy, intent, and judgment by the team (Table 1).
Proportionality
The principle of proportionality is defined as dealing with something with a certain purpose and to select the least harmful option among those that will achieve that purpose.
Considering the patient conditions, that is, degree of suffering, lack of other methods for palliation (refractoriness), and expected survival, palliative sedation should be the most proportional among all possible choices based on the balance between expected benefits and harm.
Even when palliative sedation is evaluated as a proportionally appropriate choice, sedatives should be administered with the minimum period and dose necessary for the palliation of suffering (the medication, dose, and administration method should be proportional to the aim of sedation). Periodic evaluation and regulation during palliative sedation are essential.
In estimating a patient's expected prognosis, the care team should assess prognostic factors, presence of organ failure, in addition to clinical estimation of survival. To estimate the patient's survival, validated instruments (e.g., prognosis in palliative care study predictor models) may be useful. The estimated prognosis of patients requiring continuous deep sedation is usually a few days or shorter.
Wishes and autonomy of patients
If the patient is competent, they should be sufficiently informed and explicitly request palliative sedation. If the patient is incompetent, the desire for palliative sedation should be assumed based on the values.
The consent of the family is not required, and palliative sedation can be carried out based solely on the patient's explicit or estimated wish. If family consent were an essential requirement, it would be ethically unreasonable not to carry out palliative sedation due to the absence of family consent, regardless of the patient's explicit wish. On the contrary, in Asian society, individual autonomy is usually less important than the family's overall interests, and families are also important targets of palliative care; it is necessary to talk carefully with the family about what is best for the patient and maximize efforts to reach an agreement.
The intent of medical staff
It is necessary to explicitly state that the aim of palliative sedation is not the shortening of life, but the palliation of suffering. It is ethically unacceptable to enforce palliative sedation intended to shorten life, which is different from foreseeing the shortening of life. Medical staff should explicitly share with the patient, family, and medical team members that the purpose of palliative sedation is palliation of suffering.
Judgment by the multidisciplinary team
There should be an agreement among the care team. A multidisciplinary conference is desirable. If there is uncertainty regarding the evaluation of patient competency, refractoriness of suffering, or expected survival, consultation with experts is essential.
Practical aspects
Management of symptoms when suffering is suspected to be refractory
When the patient's suffering is suspected to be refractory, the first thing to do is review whether adequate palliative care is being performed (Fig. 2). The care team should review the treatment for the symptoms that are suspected to be refractory, and simultaneously consider psychological care to increase the threshold of suffering and help the patient find meaning in life. If a temporary relief of suffering is useful for the patients, respite sedation is considered.
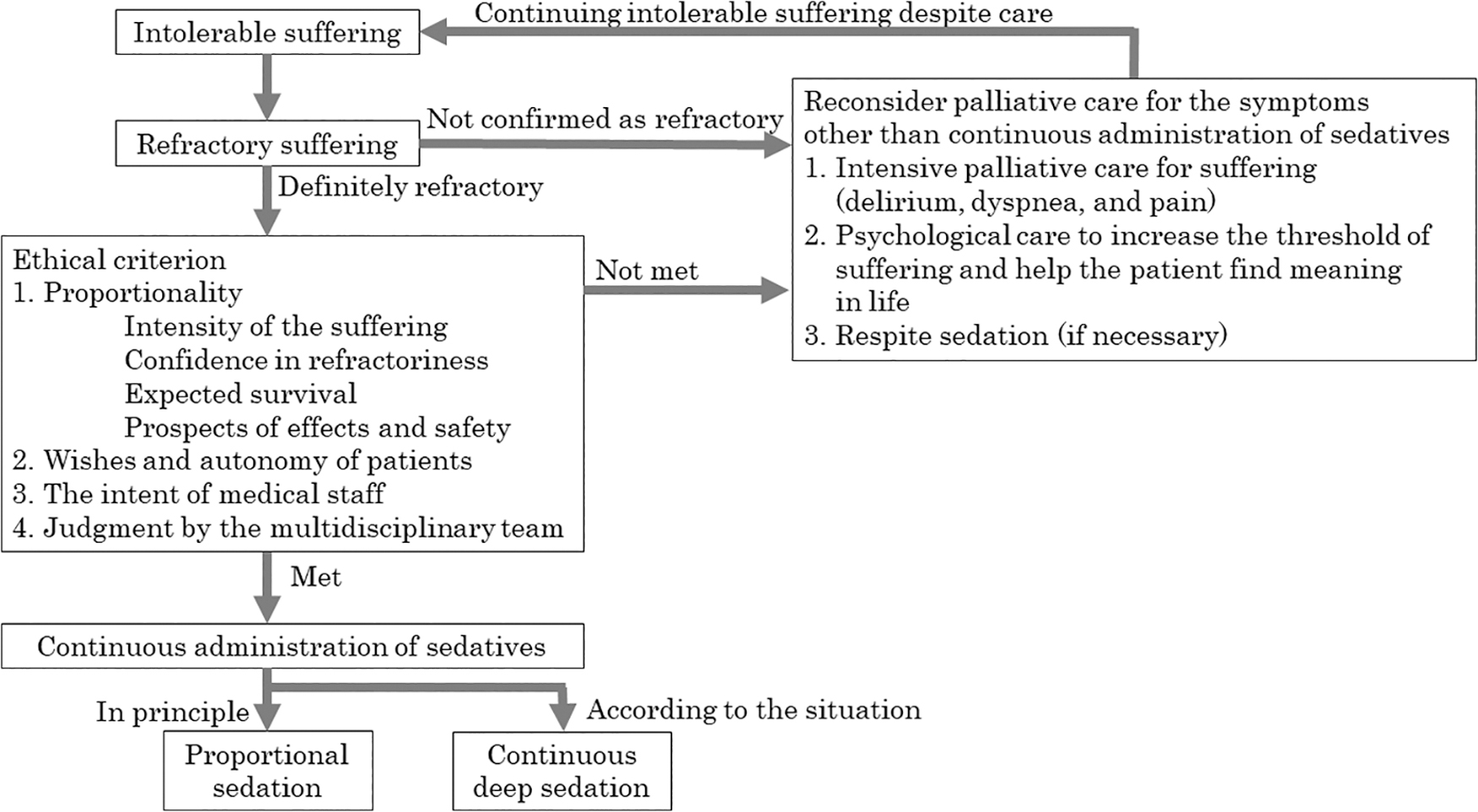
Overview of management of suffering that is suspected to be intolerable and refractory.
Details of intensive palliative care for the symptoms that can be frequently refractory are described in the Supplementary Data.
In general, the care team should assess the treatable components of underlying etiologies, symptomatic treatments, and psychosocial and environmental factors contributing to tolerability. Suffering should not be diagnosed as refractory until thorough assessments are completed. If there is uncertainty about the refractoriness of suffering, time-limited trials of potentially effective treatments should be considered. Consultation for experts is desirable when the suffering is judged as being refractory, such as pain specialists for difficult pain.
Psycho-existential suffering, such as hopelessness and meaningless, as a single indication of continuous sedation are exceptions. The appropriateness of continuous sedation for psycho-existential suffering should be very carefully addressed, and consultation to a mental health professional, such as a psychiatrist, psychologist, and pastoral care worker.
Dose of sedatives
Usually, (continuous) proportional sedation is initiated at a dose of 0.5–1.0 mg/hour with or without a bolus of 0.5–1.0 mg midazolam continuous subcutaneous/intravenous infusion. Continuous deep sedation is initiated at a dose of 3.0–5.0 mg/hour with or without a bolus of 0.5–1.0 mg midazolam continuous subcutaneous/intravenous infusion, followed by a 50%–70% dose-decrease once the desired level of sedation has been achieved. As the dose of sedatives differs greatly depending on the patient's situation, titration with precise observation of individual patient is needed.
Discussion
We revised the clinical guidelines about palliative sedation therapy to help clinicians provide better care for patients with potentially refractory suffering. The guidelines highlighted four issues.
First, we defined palliative sedation excluding the physician's intent. In the (continuous) proportional sedation, sedatives are administered based on the degree of suffering, and reducing the patient's level of consciousness is not intended.
The existing definitions of sedation from many academic associations mainly depend on the physicians' intent.16–25 For example, the European Association of Palliative Care (EAPC) defines palliative sedation as the ‘‘monitored use of medications intended to induce a state of decreased or absent awareness’’; the Royal Dutch Medical Association defines it as the ‘‘intentional lowering of consciousness of a patient in the last phase of life’’.21,23 However, it is difficult to measure the physician's intent: there is a long-continuing debate about what actually intent means (whether foreseeing and intent are distinct) and that it is vague and often contradictory.26,27
Recent reports stated that physicians may apply continuous deep sedation with at least a partial intent to hasten death: physicians in the Netherlands reported that 15% of physicians provided continuous sedation with the full or partial intent of hastening the patient's death. 32 Japanese palliative care specialists reported that 11% of them performed continuous deep sedation with intent to shorten survival to some extent. 33 We thus believe that defining palliative sedation without the physician's intent clarifies the meaning of this medical practice.
On the contrary, we agreed that the intent is important when considering the indications for sedation, and needs to be stated clearly the purpose of sedation was symptom relief, not hastening the patient's death; thus, physician intent remained to be an important element in the indication criteria.
Second, we classified continuous sedation into (continuous) proportional sedation and continuous deep sedation based on the difference in indicators for achieving the goal.11,12,28,29,34
Some may disagree with this distinction, because all palliative sedation should be performed to palliate symptoms (not reducing consciousness itself), and, any decrease in consciousness is a proportional result. 35 On the other hand, some empirical research demonstrated that physicians sometimes intended to reduce consciousness and suggested that there are two types of sedation worldwide.11,12,28,29
A preliminary study also suggested that the two types of palliative sedation defined using intervention protocols well-reflected the treatment intervention and expected outcomes, 34 and we believe that this distinction reflects the clinical practices and contributes to a better understanding of the use of sedatives in palliative care.8,11,12,28,29
Third, we concretely described comprehensive state-of-the-art practices recommended for distressing symptoms in the revised guidelines. This is because we agreed that what is important is not clarifying the patient criteria and applying practical procedures for palliative sedation but clarifying how clinicians manage such suffering. Through international efforts, we hope that more research will be performed on how to manage difficult or refractory suffering, not just palliative sedation itself.
Fourth, we clearly defined the principle of proportionality from an ethical point of view. Proportionality refers to two aspects of palliative sedation.
First, it refers to the balance between beneficial and harmful outcomes.10,20,36–39 This is consistent with the European Society for Medical Oncology (ESMO) guideline stating that the risks of treatment must be proportionate to the gravity of the clinical indication. 20 Lo and Rubenfeld maintained that proportionality is established by the terminal condition of the patient, the urgent need to relieve suffering, and the consent of the patient or proxy. 36
Second, it refers to the level of sedation applied, and this level should be proportional to the severity of the symptoms.7,10,12,28,36–39 Miccinesi et al. described palliative sedation as proportional to the refractory symptoms, that is, keeping the loss of personal values as low as possible is an ethically justified medical act. 37 In continuous deep sedation, it is ethical not to intend to maintain deep sedation until death, but discontinuing the sedation or reducing the dose of sedatives should be considered if deemed appropriate.7,10,12,28
Finally, consent from the family was changed from mandatory to desirable. In general, Asian culture places greater weight on the family decision rather than the patient's decision alone.40–42 Consent for palliative sedation from the family was required in the previous guidelines. 5 In this revision, the task force concluded that it is ethically unreasonable not to carry out palliative sedation due to the absence of family consent.16,19–21 A cultural consideration is important, 21 then future studies to clarify the adherence to this statement will be of value.
There are several important issues not addressed in this revision, and they need to be further explored. Most importantly, we did not conclude whether levomepromazine and chlorpromazine should be handled as sedatives. It is the same as whether low-dose midazolam as a therapeutic drug for dyspnea should be called proportional sedation or standard symptom palliative care. Second, further consensus is needed to be explored about the distinction of the concepts of two types of continuous sedation, that is, proportional sedation and continuous deep sedation.
Conclusion
The task force revised the Japanese guidelines on palliative sedation using the Delphi technique. The guidelines challenge five issues: (1) the definition of palliative sedation without the physician's intent, (2) classification of continuous sedation ([continuous] proportional sedation vs. continuous deep sedation), (3) the principle of proportionality, (4) family consent is not mandatory, and (5) management of symptoms when suffering is suspected to be refractory. Further discussion at an international level is urgently needed.
Footnotes
Acknowledgments
We thank Japanese Society of Cancer Nursing, Hospice Palliative Care Japan, the Japanese Association for Clinical Research on Death and Dying, Japan Psycho-Oncology Society, Japan Society of Clinical Oncology, Japanese Society of Medical Oncology, Japanese Society for Radiation Oncology, Japan Society of Pain Clinicians, Japanese Association of Supportive Care in Cancer, the Japanese Academy of Home Care Physicians, Japan Primary Care Association, the Japan Geriatrics Society, Japanese Society of Pharmaceutical Oncology, Japanese Society for Pharmaceutical Palliative Care and Sciences for their cooperation and advice in establishing recommendation statements.
Funding Information
This work was funded by the Japanese Society for Palliative Medicine.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.