
Abstract
Background:
Despite mounting evidence that specialty palliative care (PC) improves patients' symptoms, quality of life, and goal concordant care, these services are likely underutilized.
Objective:
To determine the rate of missed and delayed opportunities for specialty PC in patients with peri-hospital death.
Design:
A retrospective, cross-sectional analysis, using electronic medical records of a state-wide healthcare system in Colorado, was performed. Included were adults who died during admission or within seven days of discharge from January 2015 to October 2018 at an academic medical center and had prior encounters within the affiliated state-wide healthcare system in the last year of life. Excluded were patients with sudden or obstetrics-related deaths. Referral orders from the electronic medical record identified specialty PC consultation. Data from the Colorado Department of Public Health and Environment linked with the medical record determined time from first PC consultation to death.
Results:
The sample included 2088 decedent patients, with most deaths (81%) occurring in the hospital. Only 33% of patients had PC consultation, which was higher for patients with cancer (42%) than for those without cancer (26%). Of patients with specialty PC consultation, the median time from first referral to death was eight days (interquartile range: 3.25–25 days).
Conclusions:
Patients with peri-hospital death have low rates of specialty PC consultation, which, when present, often occurs close to death. This suggests there is a high rate of missed opportunities for specialty PC in this population.
Introduction
The burden of serious illness is tremendous. Conditions such as heart failure, cancer, and dementia account for more than 1.7 million deaths in the United States annually. 1 Morbidity is equally high for these patients who suffer myriad and often debilitating physical and psychological symptoms. 2 Beyond patients, serious illness weighs on caregivers. Half of informal caregivers experience a decline in their own health. 3 All these issues will escalate as the population ages and therapeutic options increase, thereby expanding the incidence and burden of chronic, progressive serious illnesses.
Palliative care (PC) is ideally positioned to address these challenges, as it is a specialty that is aimed at the amelioration of physical, psychological, social, and spiritual suffering at all stages of serious illness. We define serious illness as conditions with a high risk of mortality that negatively impact quality of life and well-being of patients and/or caregivers. 4 PC may include hospice as the final phase of care, prioritizing comfort in the last months of life, yet it also encompasses a broader purview by integrating symptom alleviation with life-prolonging therapies at any point from diagnosis. Specialty PC involves consultation by inpatient and/or outpatient teams separate from hospice services. In contrast, primary PC, delivered by clinicians without specialty PC training, provides a basic level of PC such as initial goals-of-care discussions as well as management of uncomplicated symptoms and patient or family distress. 5 Any remaining unmet needs warrant specialty referral.
Growing evidence demonstrates that specialty PC, especially when initiated early, improves person-centered outcomes, including patients' symptoms, caregiver burnout, and alignment of care with patients' goals.6–8 In particular, quality-of-life benefits of PC extend over three months.6–8 Specialty PC has also been associated with decreased utilization of potentially burdensome interventions at the end of life.6,7,9 Unfortunately, there is a shortage of specialty-trained clinicians, 10 which has prompted re-emphasis on primary PC. However, primary PC is currently constricted by insufficient training and time.9,11–15
In particular, hospital death and hospice referral within seven days of death are common but are generally undesired end-of-life outcomes. 16 Around 30% of patients still die in the hospital, 17 even though it is the least preferred place to die 18 and is associated with more unmet end-of-life needs.19,20 Likewise, 28% of hospice referrals occur within seven days of death. 21 However, both the National Quality Forum and the American Society of Clinical Oncology identify such short duration of hospice as an indicator of suboptimal end-of-life care given worse symptom control and quality-of-life scores when patients receive seven or fewer days of hospice.22–24
Although specialty PC is believed to be underutilized,2,9,14,15 there is a paucity of data on missed opportunities for specialty PC referral. To the authors' knowledge, in the United States, only one study of the Veteran's Affairs health system has investigated the rate of specialty PC referral in patients with hospital deaths. 25
The principal aim of this study was to determine the proportion of patients who died during or within seven days of hospitalization without specialty PC consultation in the last 12 months before death (rate of missed specialty PC). Secondary aims were to (1) determine the proportion of patients who received specialty PC consultation and who died within 90 days of referral (rate of delayed specialty PC), (2) identify the number and type of medical encounters in the past 12 months of life for patients who did not receive specialty PC (missed opportunities for specialty PC), and (3) determine patient characteristics associated with missed PC consultation.
Materials and Methods
Study design
This study is a retrospective analysis of a dataset created by an enterprise that extracts administrative and clinical information from an electronic medical record of a state-wide healthcare system and links this to data from several outside sources. The healthcare system includes one academic medical center and nine community hospitals as well as their associated outpatient specialty and primary care clinics. The academic medical center and three of the community hospitals have multidisciplinary, inpatient PC teams, including social workers, chaplains and physicians, and/or advanced practices providers. The academic medical center provides inpatient and outpatient PC services. The inpatient team maintains Joint Commission Advanced Palliative Care Certification (one of only 81 programs awarded this honor to date). 26 Joint Commission certification, among other metrics, requires the availability of PC services 24 hours a day, as well as collection and use of standardized performance measures to improve care. This clinical PC service is mature, having worked within the academic center for more than 15 years. All hospitals in the system have access to community-based PC.
Patients were included if they (1) died during admission or within seven days of discharge from January 2015 to October 2018 at the hospital of the academic medical center, (2) were ≥19 years old at time of death, and (3) had opportunities for specialty PC consultation in the 12 months before death (defined as at least one hospitalization in addition to the terminal hospitalization, two emergency department visits, or two face-to-face outpatient encounters at any facility within the state-wide healthcare system). A single emergency department or outpatient encounter in one year may be insufficient contact to demonstrate PC needs in many patients, especially those with nonmalignant disease. For this reason, two of either type of visits were required for inclusion. By including patients seen before terminal hospitalization within the system, the risk of receiving PC outside the system was minimized.
Death was identified from the state's Department of Public Health and Environment. Patients were excluded if they had International Statistical Classification of Diseases and Related Health Problems, Ninth Revision (ICD9) or International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD10) codes for obstetric-related problems (O00-O99, O9A, Z03, Z31-34, Z36-7, Z93A, V22-24, V28, 630-679) documented in the electronic medical record during the last 12 months of life. Patients were also excluded if ICD9 or ICD10 codes that are indicative of sudden death (as compiled from several prior studies1,12,27,28) were documented during their terminal hospitalization. Sample size was determined by the number of patients meeting inclusion criteria during the study period. The study was reviewed by the institution's Institutional Review Board and deemed not to be human subject research.
Outcomes
The primary outcome was the rate of specialty PC referral in the last 12 months of life. Specialty PC was defined as the presence of an order in the electronic medical record for inpatient PC consultation or a referral for outpatient PC or home-based PC. Secondary outcomes were the number of days between PC consultation and death, and the number, type, and location of clinical encounters (outpatient appointments, emergency department visits, and hospitalizations) in the last 12 months of life. The former was calculated while comparing data from the medical record with that of the state's Department of Public Health and Environment, and the latter was obtained from the medical record.
Patient factors
Data on patient factors were derived from the electronic medical record, including: age at time of death, sex, ethnicity, race, insurance class at time of death, presence of advance directive (defined as presence of an uploaded document into the category of “Advance Directive(s),” “Do Not Resuscitate Order,” or “Medical Durable Power of Attorney”), intensive care unit (ICU) stay during terminal admission, hospital death, and hospice referral. The presence of medical conditions (cancer, end-stage renal disease, chronic kidney disease, chronic pulmonary disease, cirrhosis, congestive heart failure, stroke, dementia, depression, chronic pain, and drug abuse) was identified by using previously validated ICD9 and ICD10 codes. 29 Frailty was identified for patients with dementia, admission from skilled nursing facility, or frailty-associated ICD9 and ICD10 codes. Variables were only included in the dataset if they could be abstracted from the medical record, so no participants had missing data.
Statistical analyses
Given the degree of right skew in the time between first PC referral and death, medians and interquartile ranges (IQRs) rather than means and standard deviations are reported. To determine which demographic and clinical variables were associated with the presence of specialty PC consultation, chi-squared analysis was performed. Variables associated with specialty PC consultation (p-value <0.25) were fitted into the multivariate logistic regression model. 30 Covariates included in the logistic regression model are gender, age, race, ethnicity, insurance status, comorbidity, admission to ICU during terminal hospitalization, visit with primary care, death in hospital, and presence of advance directive in chart. Analysis was performed by using R i386 3.5.1 software.
Results
Our study identified 2928 patients who died during admission or within seven days of discharge from the academic medical center. Of these patients, 39 had insufficient contact within the state-wide healthcare system before their terminal admission so they were excluded. In addition, 801 patients were excluded for obstetric-related or sudden death. This resulted in the inclusion of 2088 patients, of whom 1688 (81%) patients died in the hospital. Patients were 56% male, 66% white, 15% Hispanic, and 11% black. The average age was 64 years old. There was a high level of medical illness, as 45% had cancer, 73% had organ failure (defined as having heart failure, cirrhosis, chronic kidney disease, or chronic lung disease), and 61% had frailty (defined as having dementia, being admitted from a nursing facility, or having ICD9 or ICD10 codes indicative of frailty).
Regarding the primary and secondary outcomes (Tables 1 and 2), only 33% of patients received PC consultation in the 12 months before death and this was higher for patients with cancer (42%) than for those without cancer (26%). The median time from initial PC consultation to death was eight days (IQR: 3.25–25 days). Of patients with specialty PC referral, 47% had consultation within just seven days of death and only 10% had consultation >90 days before death (Fig. 1). During the last 12 months of life, patients without PC had fewer healthcare contacts than those with PC with an average of 1.8 versus 2.4 hospitalizations, 1.5 versus 2.1 emergency department visits, and 9.4 versus 18.2 clinic appointments respectively.
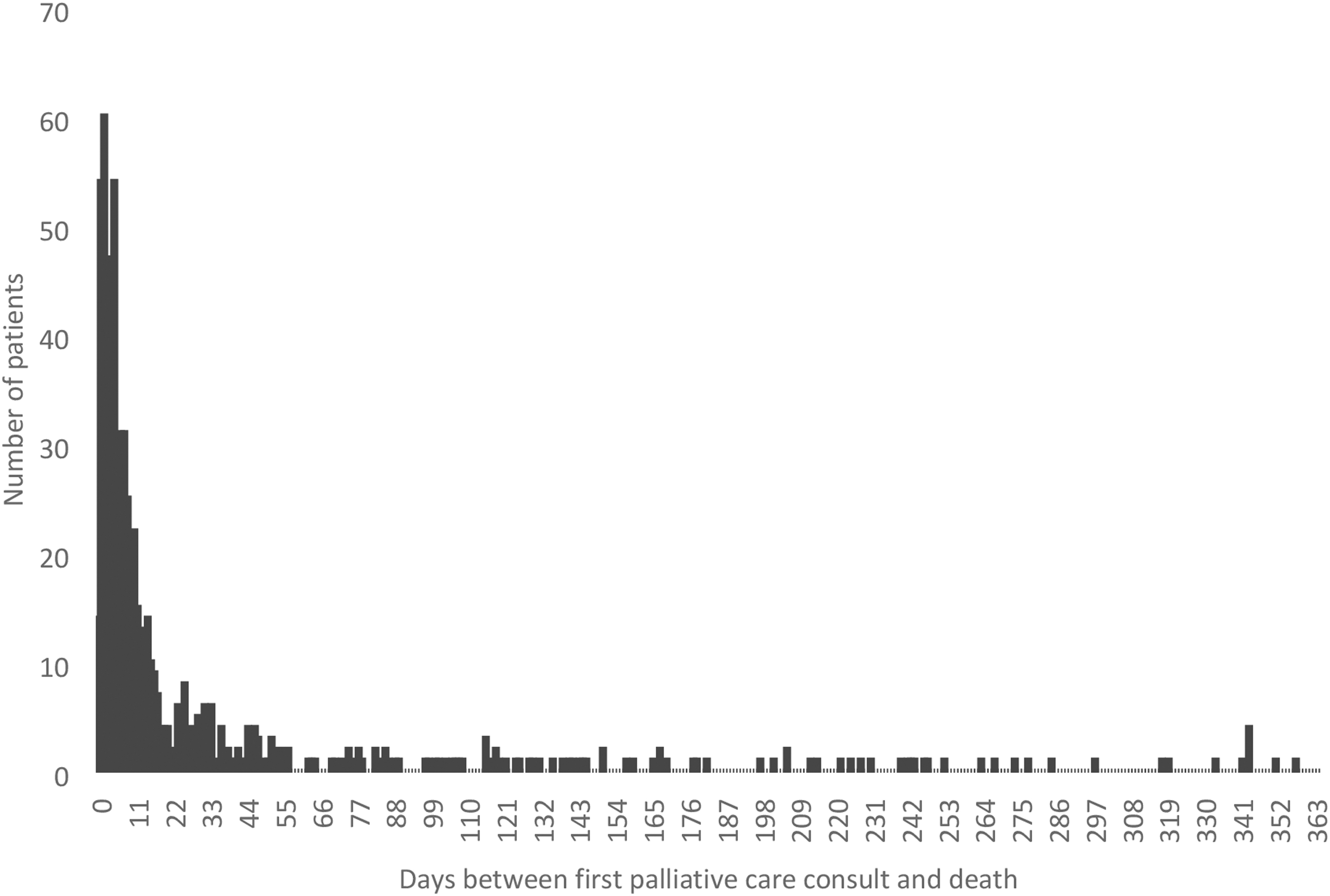
Histogram of patients per duration of specialty palliative care.
Percentage of Patients with Specialty Palliative Care by Patient Variables
ICU, intensive care unit; n, number of patients; PC, palliative care; %, percentage of patients.
Time from First Palliative Care Consultation to Death by Patient Variable
IQR, interquartile range.
In addition, of patients receiving specialty PC, the majority (91%) received inpatient consultation whereas only 20% and 4% had outpatient and home PC referrals, respectively. In comparison to patients without cancer, those with cancer had a higher degree of outpatient referrals (28% vs. 9%) and a lower rate of inpatient consultation (89% vs. 95%). Although 94% had some form of an advance directive document uploaded into the chart, only 10% received hospice care.
We used results from the unadjusted analysis to fit the logistic regression model (Table 3), which found that age <65 years old, age 65–84 years old, self-pay insurance, cancer, stroke, frailty, drug abuse, and presence of some type of advance directive document were positively associated with specialty PC referral and, therefore, negatively associated with missed opportunities for specialty PC referral. Conversely, other ethnicity, chronic pulmonary disease, and admission to ICU during terminal hospitalization were negatively associated with specialty PC referral and, thus, positively associated with missed opportunities for specialty PC referral.
Chi-Squared Analysis and Logistic Regression of Association with Palliative Care Consultation by Patient Variable
CI, confidence interval; OR, odds ratio; X2, chi squared.
Discussion
Absent specialty PC as missed care
The majority of patients with peri-hospital deaths in this sample (67%) did not receive specialty PC. This is particularly true for patients without malignancy (74%) as compared with those with cancer (58%). This proportion is higher than a comparable study of nearly 58,000 U.S. veterans who died in hospitals or nursing homes: This study found that 42% of patients did not receive specialty PC. 25 Although 20% of these veterans died in nursing homes, this is also a population at high risk for unmet end-of-life needs. Although the ideal rate of specialty PC consultation per death is unknown, a referral rate of 58% in patients with high risk for unmet end-of-life needs as seen within the Veteran's Affair healthcare system can serve as a minimal benchmark.
The discrepancy in rates of specialty PC referral in our cohort and the Veteran's Affair population likely represents a missed opportunity for care, because peri-hospital death is associated with poor outcomes. First, patients and their families generally prefer to avoid dying in the hospital.1,11,18 In addition, in comparison to home or hospice death, hospital death is associated with more unmet end-of-life needs with worse symptom control, caregiver support, and communication regarding patients' illnesses.19,20 One study of hospital decedents showed that up to 29% of symptoms received insufficient management, up to 57% of their caregivers' needs were inadequately addressed, and up to 33% of these patients received confusing or contradictory information. 31 Importantly, more than half of complaints to hospitals pertain to the dying process. 19
Similarly, dying within seven days of admission to hospice is a risk for poor end-of-life care.22–24 Patients with fewer than seven days of hospice care are more likely to have undertreated pain, worse quality-of-life scores, and discordance between their actual and preferred place of death.22,23 Moreover, caregivers of patients with such short duration of hospice care, compared with those with longer periods of care, have higher rates of depression up to six months after patients' deaths. 24 Because of this and related data, both the National Quality Forum and the American Society of Clinical Oncology identify admission to hospice within seven days of death as an indicator of poor end-of-life care. 22
Patients who did not receive specialty PC had numerous missed opportunities for referral to either outpatient or community-based PC, with an average of nine face-to-face clinical visits and two admissions during the last 12 months of life. The frequency of outpatient visits suggests that the clinic is an opportune setting for interventions to increase PC consultation. Likewise, hospitalized patients and their families may be particularly receptive to PC, as exacerbations of their illnesses can prompt reflection and highlight unmet needs.
Late specialty PC as delayed care
When consulted, specialty PC in our cohort occurred exceedingly close to death. The median time from referral to death was eight days. In previous studies, the number of days from first contact with specialty PC and death is variable, with the median ranging from 10 to 70 days.12,14,32,33 The short time from specialty PC to death implies a delay in care. Although the precise timing of PC is still debated, 34 the body of literature supports positive effects of PC extending to at least three months.6–8 In our cohort, 90% of patients had PC consults less than 90 days before death, suggesting that they did not fully benefit from PC.
Missed and delayed PC as a potential medical error
As we have stated, peri-hospital death is often not goal concordant care and confers a high risk of unmet end-of-life care needs. However, these patients had numerous opportunities in their last 12 months of life for specialty PC referral, which improves concordance of place of death with patient preference and reduces end-of-life hospitalizations.2,9 In other words, peri-hospital death is a poor but potentially preventable end-of-life outcome. Predicting the precise timing of death, even with the best tools, is inherently limited. However, specialty PC can occur at any stage of serious illness, which makes receiving consultation before the last weeks of life much more feasible. Therefore, we argue that the majority of cases of absent and delayed specialty PC in patients with peri-hospital deaths may constitute a medical error. Further investigations of the quality of end-of-life care management in patients with peri-hospital mortality is necessary to confirm and clarify this claim.
Clinician bias, rather than patient and family resistance, is the main source of absent PC consultation. 14 First, clinicians overestimate prognosis (optimism bias) by up to 530%. 35 In addition, there is often a misconception that PC is indicated only when death is imminent (commission bias) and PC is sometimes seen as a personal failure.14,36 The high degree of untimely PC consultation in this study, despite access to highly resourced PC teams, indicates the impact of these biases. As such, a high index of suspicion is often required to recognize the need for specialty PC and there are many tools and triggers to identify patients who may benefit from PC.37,38
Limitations
The retrospective review of data from the medical record carries several limitations, including the inaccuracies of charted information. Although this health care system encompasses a wide network of practices, some patients may have received uncaptured out-of-network PC services. In addition, we do not know the quality of end-of-life care for these patients and their families, so it is possible that all end-of-life needs were met by primary PC and specialty care was not warranted.
Our findings may overestimate the rates of specialty PC in other health care systems that may have fewer specialty PC resources than this academic medical center with a Joint Commission certified inpatient PC team with a low rate of missed consults, 2.4% during the study period (Dr. Jeanie Youngwerth, Director of Clinical Palliative Care, e-mail communication, February 2020). Finally, when to initiate specialty PC services is still debated. Defining delayed PC as consultation within three months of death carries support from several high-quality trials of early PC.6–8 In addition, many guidelines and programs use the “surprise question” to trigger PC before the last six to twelve months of life. 39
Next steps
This study prompts further investigation of missed and delayed specialty PC on a population level in the United States. The proportion of patients with peri-hospital death with absent or delayed PC consultation can serve as an outcome for research on identifying patients with high likelihood of needing specialty PC.
Conclusion
Patients who die in the hospital or shortly after discharge have a high degree of missed opportunities for specialty PC. This may represent a medical error that warrants greater attention, especially given the general preference to die at home.
Footnotes
Acknowledgments
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.