
Abstract
Background:
Delirium is a common debilitating complication of advanced cancer.
Objective:
To determine if a multicomponent nonpharmacological delirium prevention intervention was feasible for adult patients with advanced cancer, before a phase III (efficacy) trial.
Design:
Phase II (feasibility) cluster randomized controlled trial. All sites implemented delirium screening and diagnostic assessment. Strategies within sleep, vision and hearing, hydration, orientation, mobility, and family domains were delivered to enrolled patients at intervention site admission days 1–7. Control sites then implemented the intervention (“waitlist sites”).
Setting:
Four Australian palliative care units.
Measurements:
The primary outcome was adherence, with an a priori endpoint of at least 60% patients achieving full adherence. Secondary outcomes were interdisciplinary care delivery, delirium measures, and adverse events, analyzed descriptively and inferentially.
Results:
Sixty-five enrolled patients (25 control, 20 intervention, and 20 waitlist) had 98% delirium screens and 75% diagnostic assessments completed. Nurses (67%), physicians (16%), allied health (8.4%), family (7%), patients (1%), and volunteers (0.5%) delivered the intervention. There was full adherence for 5% patients at intervention sites, partial for 25%. Both full and partial adherence were higher at waitlist sites: 25% and 45%, respectively. One-third of control site patients (32%) became delirious within seven days of admission compared to one-fifth (20%) at both intervention and waitlist sites (p = 0.5). Mean (standard deviation) Delirium Rating Scale-Revised-1998 scores were 16.8 + 12.0 control sites versus 18.4 + 8.2 (p = 0.6) intervention and 18.7 + 7.8 (p = 0.5) waitlist sites. The intervention caused no adverse events.
Conclusion:
The intervention requires modification for optimal adherence in a phase III trial.
Introduction
Delirium is an acute, distressing and debilitating neurocognitive disorder of physiological etiology for more than one-third of patients with advanced cancer in palliative care units.1–4 Occurrence is higher again for those who die in this setting, with median (range) period prevalence of 75% (58%–88%). 2 The high prevalence contributes to widely held assumptions that delirium is inevitable in people with advanced cancer, especially in the last weeks and days of life. 5 Yet potential to prevent this devastating complication exists, warranting systematic evaluation in oncology and palliative care contexts.6–8
Other clinical settings have decreased delirium incidence and risk in older and seriously ill patients, including intensive care units (ICUs), where it was once thought unavoidable.9–14 Overall, one-third reduction in delirium incidence has been reported for patients in non-ICU settings through multicomponent interventions targeting physical and cognitive activity, sleep, hydration, and vision and hearing.9–11 In a study of over 15,000 ICU patients, complete performance of a care bundle to improve pain, awareness, breathing, use of psychoactive medication, delirium detection, mobility, and family engagement significantly reduced the likelihood of becoming delirious the following day (adjusted odds ratio 0.60 [0.49–0.72]; p < 0.0001). 14
Achieving similar results for people with life-limiting illness in hospital would enable many to maintain mental and physical function and better attend to what and who is most important to them. 15 We therefore designed a program of research to evaluate whether targeting the fundamental care needs of people with advanced cancer in hospital would improve delirium-related outcomes, including for patients in the last weeks and days of life. In line with the Medical Research Council framework for complex interventions, 16 we first developed a multicomponent nonpharmacological delirium prevention intervention for patients with advanced cancer from existing evidence4,7,9–11 and then tested its methods and impact in a phase II (feasibility) trial, before embarking on a phase III (efficacy) trial of the intervention.
Results of the phase II trial are reported here according to Consolidated Standards of Reporting Trials guidelines. 17 The trial was registered with the Australian and New Zealand Clinical Trials Registry 18 and a protocol detailing its justification and methods was published in January 2019. 19
Methods
Design
A phase II cluster randomized controlled trial (RCT). We chose the cluster RCT design because the intervention suited site-level implementation and it reduced risk of contamination. As similar interventions have been effective in other patient populations and settings, site investigators requested that control sites be given opportunity to later trial the intervention. We therefore integrated a “waitlist” option for control sites into the study design, whereby sites randomized to control were given details of the intervention and option to deliver it after initial data collection at intervention sites. 20 Addition of the waitlist option furthermore provided opportunity to refine the intervention and/or study processes if initial data from intervention sites indicated need to do so.
We also embedded a qualitative substudy to obtain patient, family caregiver, staff, and volunteer perspectives about feasibility and acceptability of the intervention and study measures, analyzed according to the Theoretical Domains Framework for health-related behaviors. 21 Methods and findings of the substudy will be reported in full elsewhere.
The overall study design is presented in Figure 1.
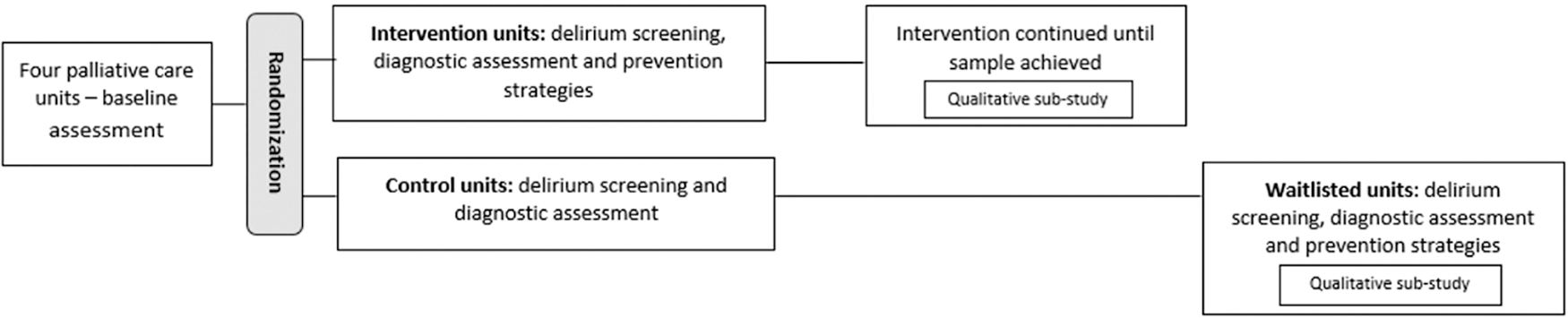
Study diagram standardized delirium screening and diagnostic assessment at all units + delirium prevention strategies at intervention units (May–June 2018); control units were waitlisted to the intervention (August–September 2018).
Setting and participants
Participating sites were four specialist palliative care inpatient units within hospitals in metropolitan Australia. Investigators M.A. and A.H. recruited sites in 2017. Patients eligible for enrolment were adults (i.e., 18 years of age or older) with advanced (stage 4) cancer. 22
Randomization
The trial statistician L.L. allocated sites to intervention or control plus waitlist intervention conditions in October 2017 at University of Technology Sydney (UTS) using a permuted block randomization method. We notified sites of allocation after local governance approvals.
Ethical procedures
Hospital and university Human Research Ethics Committees approved the trial (HREC/17/LPOOL/224 and ETH17-1697). One person per site with requisite authority gave cluster-level consent to participate. Patients and family were informed about the trial through posters and verbal communication, including that they could opt out.
Intervention and control conditions
All sites instituted delirium screening and diagnostic assessment of enrolled patients for the first seven days of admission. Nurses completed the Nursing Delirium Screening Scale (Nu-DESC) 23 each eight-hour shift. Within 24 hours of a positive Nu-DESC (score ≥2) for patients not already diagnosed as delirious, physicians applied Diagnostic and Statistical Manual of Mental Disorders, Fifth edition (DSM-5) diagnostic criteria for delirium 1 and the Delirium Rating Scale-Revised-1998 (DRS-R-98). 24 Except for one site that mandated the Nu-DESC for the first three days of admission, structured delirium screening and diagnostic assessment were new processes and therefore additional to usual care.
The intervention had six domains (eating and drinking, sleep, exercise, reorientation, vision and hearing, and family partnership), containing 36 strategies overall (4–12 per domain) (Supplementary Table S1). We asked team members to enlist family and volunteers and tailor the intervention to patients' needs and wishes. Team members documented delivered strategies on a checklist designed for data collection, plus their designation and reason for nondelivery: “not required,” “patient choice,” “not clinically appropriate,” “not possible with current resources,” and “other.” 19
A two-month site engagement and training period, guided by customized information manuals (available on request), preceded control and intervention conditions. Sites formed working groups of interested team members to plan implementation in line with their resources and systems. University-based researchers attended working group meetings to ensure intervention fidelity, trial integrity, and timely progress (A.H., R.A., J.H., and J.W.). Sites shared meeting records whenever researchers could not attend in person.
We designed and conducted training through four discrete 30–40-minute sessions (i.e., Introduction to the study; Delirium screening using the Nu-DESC; Delirium assessment and diagnosis; Multicomponent delirium prevention intervention) using Biggs' educational model 25 (A.H., R.A., J.H., J.W., site investigators, clinical educators, and nursing managers), delivered multiple times for broadest reach. Learning outcomes were clinicians' understanding of the study processes relevant to their role and achievement of target adherence to study measures. Control sites received information about delirium prevention strategies when they transitioned to the intervention phase, along with a summary of learnings from intervention sites about optimizing trial processes. A key message was that the checklist was not the intervention per se, but essential to measuring the primary outcome of adherence.
Data collection
Site research nurses recorded delirium measures, intervention delivery, and adverse events during enrolled patients' first seven days of admission on Case Report Forms and Excel spreadsheets and uploaded data into REDCap. 26 Project staff obtained site-level patient demographics and functional status for all patients admitted during study periods from Palliative Care Outcomes Collaboration datasets. 27
The schedule of study measures is presented in Supplementary Table S2.
Blinding
The cluster design and nature of the intervention precluded blinding of site teams and data collectors. To minimize ascertainment bias, sites teams provided patients and family caregivers with information about clinical aspects of the trial, but not design or site allocation. We used standardized data collection tools and training to limit measurement bias.
Outcomes
The primary outcome was intervention adherence at intervention and waitlisted sites, according to checklist documentation of each strategy at least once daily for the first seven days of admission. A priori, 60% or more patients having full adherence (delivery of all required strategies within at least four domains for at least five days) was considered minimum evidence that the intervention was feasible without major modification. Partial adherence to the intervention was defined as at least one strategy in at least four domains daily for at least five days.
Secondary outcomes were as follows:
Delivery of care: (i) sample feasibility (percentage of patients with data collected, reasons for noninclusion, and time to achieve sample); (ii) coverage (proportion eligible patients receiving intervention, reasons for nondelivery, and weekend coverage); (iii) compliance with study measures; (iv) methods, areas, and levels of interdisciplinary delivery; and (v) sustainability (adherence to delirium measures and prevention strategies at sites six months after intervention). Delirium related: (i) proportion of patients with a positive Nu-DESC at least once each 24 hours; (ii) delirium incidence (first meeting DSM-5 delirium diagnostic criteria within 24 hours of a positive Nu-DESC); and (iii) delirium severity (DRS-R-98 at first onset). Adverse events: falls, deaths, other, according to National Cancer Institute Common Terminology Criteria for Adverse Events,
28
and complaints, reported as numbers, rates, and descriptively, overall and intervention related.
Sample size
To obtain a sufficient sample size for a pilot study of at least 9% of the sample of the planned phase III trial, we enrolled four sites and 40 patients (10 per site), and then 20 patients at waitlisted sites (10 per site). 29
Statistical analysis
Adherence to the delirium prevention strategies and by whom were computed using conditional counting techniques. Secondary outcomes were summarized using frequency and percentage for categorical variables, and mean and standard deviation (SD) or median and range for continuous variables. Independent sample t-tests, chi-square tests, and Fisher's exact test were used to measure differences between patients' demographic and delirium status across control, intervention, and waitlist sites. Data were managed using Microsoft Excel 2016 and Statistical Package for Social Sciences version 25.
Results
During enrolment periods, the four sites admitted 90 patients and screened all for eligibility (Fig. 2). Seventy-two patients were eligible according to the protocol, with 68 considered eligible by site investigators. Four eligible patients were not enrolled due to the following: “distress on admission,” “patient admitted for terminal care,” and “patient unable to communicate well,” with no reason given for the fourth. Nonenrolment of three patients considered eligible by site investigators was because two patients requested withdrawal and one “other.”
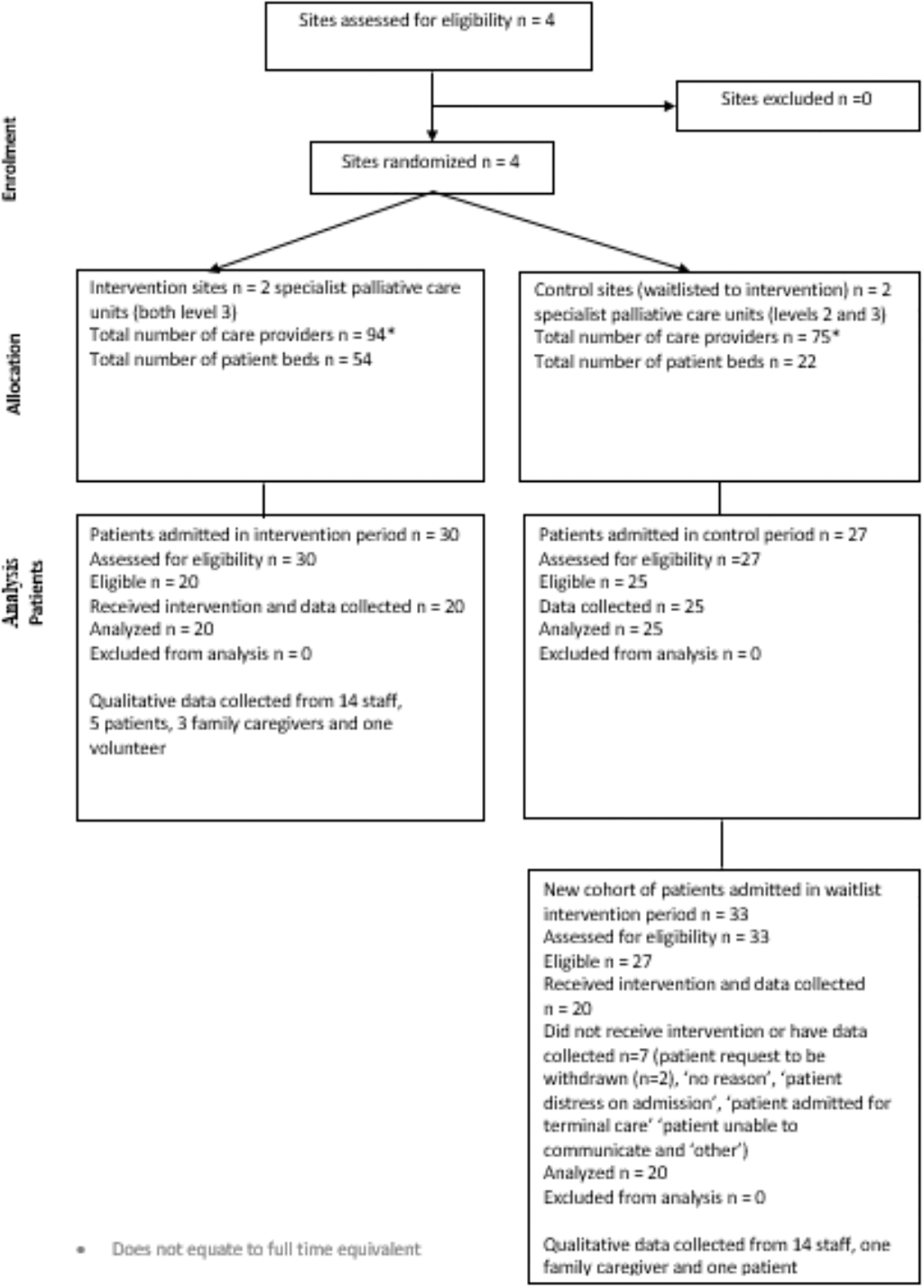
CONSORT flow diagram.
We collected and analyzed data for 65 patients (90% of protocol-eligible patients and 96% according to site investigators). Of these, 38 patients (58%) had seven days of data collected. Twenty patients died within seven days (31%), four were discharged (6%), one control site patient was considered not well enough to continue, and two patients had data collection ceased before seven days for other, nonspecified reasons.
Patient enrolment took an average of 20 days per site (range 8–36) and the overall sample was achieved in five months (May–September 2018).
Site-level patient characteristics
During study periods, just over half (56%) of all admitted patients were male. Most were 70 years of age or older (59%), with a primary diagnosis of cancer (90%), born in Australia (56%), and had English their primary language (92%). Few were Aboriginal or Torres Strait Islander (n = 2, 1%). There were no significant differences in patients' baseline characteristics at control sites compared to intervention or waitlist sites (Table 1).
Site-Level Patient Characteristics on Admission
Site-level data include ALL patients admitted during study periods.
With Bonferroni adjustment for family-wise corrections (p = 0.05/3 = 0.0167), independent sample t-test revealed statistical significant difference for mean ages (p = 0.001) and chi-square tests revealed statistical significant differences for age >70 (0.008) and genders (0.01) between the intervention and waitlisted sites.
AKPS, Australian-modified Karnofsky Performance Scale; ATSI, Aboriginal or Torres Strait Islander; RUG-ADL, Resource Utilisation Group Activities Daily Living; SD, standard deviation.
Adherence to the intervention
Overall, 40 patients received the intervention for an average (SD) of 5.8 ± 1.8 days. Of these, 14 died (35%) and 2 (5%) were discharged within seven days of admission.
There was full adherence for 5% patients at intervention sites and 25% at waitlist sites. Percentages of patients having partial adherence were 25% at intervention sites and 45% at waitlist sites (Fig. 3).

Adherence to delirium prevention intervention at intervention and waitlisted sites, calculated as either all strategies or any strategy ≥4 domains for ≥5 days.
Per domain, highest adherence was to exercise (59%), then eating and drinking (54%), reorientation (52%), and sleep, vision and hearing, and enabling family (each 41%) (Table 2). There was higher delivery of every strategy at waitlist sites. Overall, nurses delivered most strategies (67%), followed by medical staff (16%), allied health (8.4%), family caregivers (7%), and volunteers (0.5%), with patients themselves recording 1.1%. There was minimal documentation of reasons for nondelivery: “not required” (1.4%), “not appropriate” (1%), “patient choice” (0.7%), “not possible” (0.4%), and “other” (n = 1).
Adherence and Interdisciplinary Delivery of the Intervention
All figures are percentages of patients receiving intervention elements.
Codes for allied health staff and rate of their participation in overall delivery of the delirium prevention intervention: D, Dietician (4.2%); P, Physiotherapist (2.3%); PC, Pastoral care (1.1%); OT, Occupational therapist (0.4%); SW, Social worker (0.3%); SP, Speech pathologist (0.1%).
IDC, indwelling catheter; IV, intravenous line.
Delirium measures
Nurses completed the Nu-DESC at least once per day for 373/379 patient days (98%). Physicians applied the DSM-5 diagnostic criteria and DRS-R-98 within 24 hours of a first positive Nu-DESC for 24/31 occasions (77.4%). There was no significant difference between weekday and weekend completion of delirium measures.
Eight patients developed delirium in the first seven days of admission at control sites (32%) compared with four patients each at intervention (20%) and waitlist sites (20%) (p = 0.5). Mean (SD) delirium severity (DRS-R-98) was 16.8 ± 12.0 for patients at control sites compared with 18.4 ± 8.2 at intervention sites (p = 0.6) and 18.7 ± 7.8 at waitlist sites (p = 0.5) (Table 3).
Delirium Incidence and Severity
Fisher's exact test and Independent sample t-test found no statistically significant difference for any delirium measure across study sites.
DRS-R-98, Delirium Rating Scale-Revised-1998; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth edition; Nu-DESC, Nursing Delirium Screening Scale.
Adverse events
Forty-five patients (69%) experienced a total of 162 adverse events: 15 (60%) control, 14 (70%) intervention, and 16 (80%) waitlist sites (Supplementary Table S3). Site investigators attributed no adverse event to the intervention. Two (8%) control site patients fell, compared with one each at intervention and waitlist sites (5%). Six (24%) patients died within seven days of admission at control sites compared to 7 (35%) at both intervention and waitlist sites.
Sustainability (at six months)
Of 20 consecutively admitted patients (five per site), 2 patients (10%) died within five days, leaving 97 patient days for analysis. In these, there were five instances of delirium screening using the Nu-DESC and one using the Confusion Assessment Method (6%). 30 There was no DRS-R-98 or DSM-5 diagnostic criterion for delirium documented. Adherence to the delirium prevention strategies was not full for any patient and partial for 6 (30%). Almost every strategy was less frequently documented than during the intervention (Table 2).
Discussion
Despite site engagement and training and higher intervention adherence at waitlist sites, the trial did not achieve its primary feasibility outcome. In contrast, secondary outcomes demonstrated feasibility of the sample and delirium measures, no adverse effect, and a nonstatistically significant decrease in the proportion of patients with delirium in the first week of admission when sites delivered the intervention. Adherence was higher at waitlist sites, likely due to the more staged implementation (i.e., delirium measures then prevention strategies), in conjunction with giving waitlist site teams more explicit information about importance of documenting the intervention. Post-intervention, measurement of usual care demonstrated higher adherence to strategies occurred within trial. Taken together, results support the ongoing investigation of delirium prevention in patients with advanced cancer though nonpharmacological means. However, as higher delivery of multicomponent nonpharmacological delirium prevention interventions is associated with greater effectiveness, modifications to optimize adherence in a phase III trial will be required.14,31
Next steps in this staged research program are to integrate qualitative findings with trial results to inform modification of the intervention. Strategies to be retained will be those with highest overall evidence, delivered with higher adherence or underdelivered due to resolvable barriers in this trial, and considered essential by those involved.
An intervention with fewer strategies will also facilitate more precise dose measurement. In this feasibility trial, it was sufficient to measure intervention frequency (24 hours) and duration (one week), whereas determining dose/efficacy ratios will also require measuring the amount patients receive each time. 32 Full dose measurement will require a priori consideration of equivalent strengths of intervention parts and whether to measure these at the domain or strategy level.
Other factors important to consider for dose potency are who delivers the strategy and how, because fundamental care strategies are delivered through highly interpersonal interactions. Such interactions serve not only visible objectives (e.g., to help the person drink a glass of water) but also to communicate caring, compassion, and respect for an ill person. How fundamental care is delivered is instrumental to maintenance of psychological well-being during advanced illness and dying in hospital, and therefore worthy of closer attention in future delirium research in palliative care contexts.33,34
We explicitly sought to include patients near the end of life in this trial and so it was not surprising that almost one-third of enrolled patients died within seven days of admission. Endeavoring to develop and trial nonpharmacological delirium interventions in the last weeks of life is justifiable, because patients with terminal illness value maintaining cognition and connection with others,35,36 and both delirium and customary pharmacological treatments disrupt this potential.8,37 However, it is not possible to diagnose delirium in an unresponsive person. 1 Therefore, collateral measurement of psychomotor activity and awareness would inform a primary trial outcome of days without delirium or coma, as successfully evaluated in studies in intensive care.12,14 This would be a clinically meaningful palliative care outcome, as it would help determine the extent to which nonpharmacological delirium interventions enable patients to remain more alert and able to attend to important undertakings with those they love in the last days of life. 38
Limitations and strengths
Limitations include lack of blinding, inherently difficult in multicomponent nonpharmacological interventions, and a source of bias in this field of delirium research. 7 The small sample was appropriate for a phase II trial, but precluded definitive determination of intervention effectiveness in reducing delirium incidence or severity. While patients who became delirious continued to receive the intervention, we did not examine delirium treatment or resolution. Strengths include the cluster RCT design, which promoted enrolment of almost all eligible patients and reduced the risk of selection bias. The waitlisted arm facilitated multisite recruitment and engagement. Systematic adverse event measurement ensured close monitoring of enrolled patients for potential harms and was an advancement upon previous similar studies. 7
Generalizability
The study informs future research in delirium prevention in patients with advanced cancer in palliative care units. The study population was representative of Australian palliative care inpatients and sites typified the varyingly resourced units across metropolitan Australia. Intervention strategies addressed fundamental human needs, and prior implementation in many settings underscores their universal relevance for hospitalized patients.15–17 However, results may not be generalized to other geographical regions, health care systems, or patients with other advanced illnesses.
Conclusion
A multicomponent intervention to optimize eating and drinking, sleep, exercise, reorientation, vision and hearing, and family partnership to prevent delirium in patients with advanced cancer was piloted in four palliative care units. Outcomes indicate a phase III trial will be feasible in this patient population and setting if the intervention is modified. Next steps are to integrate qualitative findings with trial results to inform modification of the intervention, and determine dose and outcome measures most fitting for patients with advanced cancer in palliative care units, including those in the last weeks and days of life.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of patients, family caregivers, clinicians, and volunteers at the four participating sites and the Palliative Care Outcomes Collaboration team who provided site-level data.
Funding Information
The trial was funded by an Australian National Breast Cancer Foundation (NBCF) 2017 Pilot Study Grant (Grant code PS-17-030), contact details Level 9, 10 Barrack Street, Sydney, NSW, 2000, Australia; T: +61 2 8098 4800, E: ![]() . The NBCF had no role in the study design, data collection, management, analysis, interpretation, or publication of results.
. The NBCF had no role in the study design, data collection, management, analysis, interpretation, or publication of results.
The trial sponsor was the Palliative Care Clinical Trials Collaborative (PaCCSC) (Level 3, 235 Jones Street, Ultimo, NSW, 2007, Australia; T. +61 (2) 9514 4862 (Sydney)/+61 (8) 7421 9726 (Adelaide), E: ![]() ). PaCCSC supports optimal trial governance through standard operating procedures for electronic data handling, completion of case report forms, monitoring, dissemination, archiving of research materials, and record destruction, and trial infrastructure through Trials Management and Scientific Committees.
). PaCCSC supports optimal trial governance through standard operating procedures for electronic data handling, completion of case report forms, monitoring, dissemination, archiving of research materials, and record destruction, and trial infrastructure through Trials Management and Scientific Committees.
Author Disclosure Statement
Drs. A.H., J.P., L.L., S.K., S.L.C., A.G., and M.A. and Ms. L.B., B.F., L.E., J.H., R.A., T.A., M.G. and J.W. report a grant from the National Breast Cancer Foundation during the conduct of the study. Dr. A.H. also reports personal fees from Medtronic, outside the submitted work. Dr. G.A.C. reports grants from Bionomics Pty Ltd., outside the submitted work. Dr. E.W.E. reports personal fees from Masimo, grants from VA/NIH, personal fees from Pfizer/Orion, and grants from Koheler, outside the submitted work. All remaining authors have no disclosures to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.