
Abstract

Dear Editor:
Physician orders for life-sustaining treatment offers health care providers information about an individual's treatment preferences to guide medical care. According to the National POLST Paradigm, the POLST is intended for “patients who are considered to be at risk for a life-threatening clinical event because they have a serious life-limiting medical condition, which may include advanced frailty.” 1 However, there are anecdotal concerns that POLST is sometimes used in a healthier population than intended. 2
The Colorado version of POLST is called Medical Orders for Scope of Treatment (MOST). 3 Our objective was to explore whether the Colorado MOST was completed during primary care visits for potentially inappropriate patients. Specifically, we assessed whether patients who had a completed MOST in the electronic health record (EHR) within seven days of an outpatient visit where an advance care planning (ACP) billing code (CPT code 99497 or 99498) was submitted had a serious life-limiting medical condition.
From July 1, 2017 through March 31, 2019, 390 UCHealth (Colorado) patients had an ACP billing code associated with an outpatient visit. Of these, 97 patients had an ACP document (e.g., advance directive or MOST) added to the EHR within seven days; and in 63 patients, the ACP document was a MOST. To adjudicate potentially inappropriate use of the MOST, we operationalized the National POLST guidelines as follows: diagnoses including advanced organ failure, metastatic cancer, advanced dementia (based on clinical documentation of moderate or severe dementia), or age ≥90 years. Charts were reviewed by two researchers who discussed discrepancies with a third researcher to reach consensus. The Institutional Review Board approved this research.
Forty-four of 63 (70%) patients were judged to be appropriate for MOST use based on diagnosis of advanced organ failure, metastatic cancer, advanced dementia, or advanced age (Fig. 1). Patients who were appropriate for MOST use were older (81.5 years vs. 74.4 years, p = 0.013), more medically complex (Hierarchical Condition Category score 1.65 vs. 1.10, p = 0.047) and more likely to have had an emergency department visit or hospitalization in the 30 days before the ACP billing encounter (20% vs. 0%, p = 0.033) compared with patients for whom the MOST was potentially inappropriate based on diagnosis.
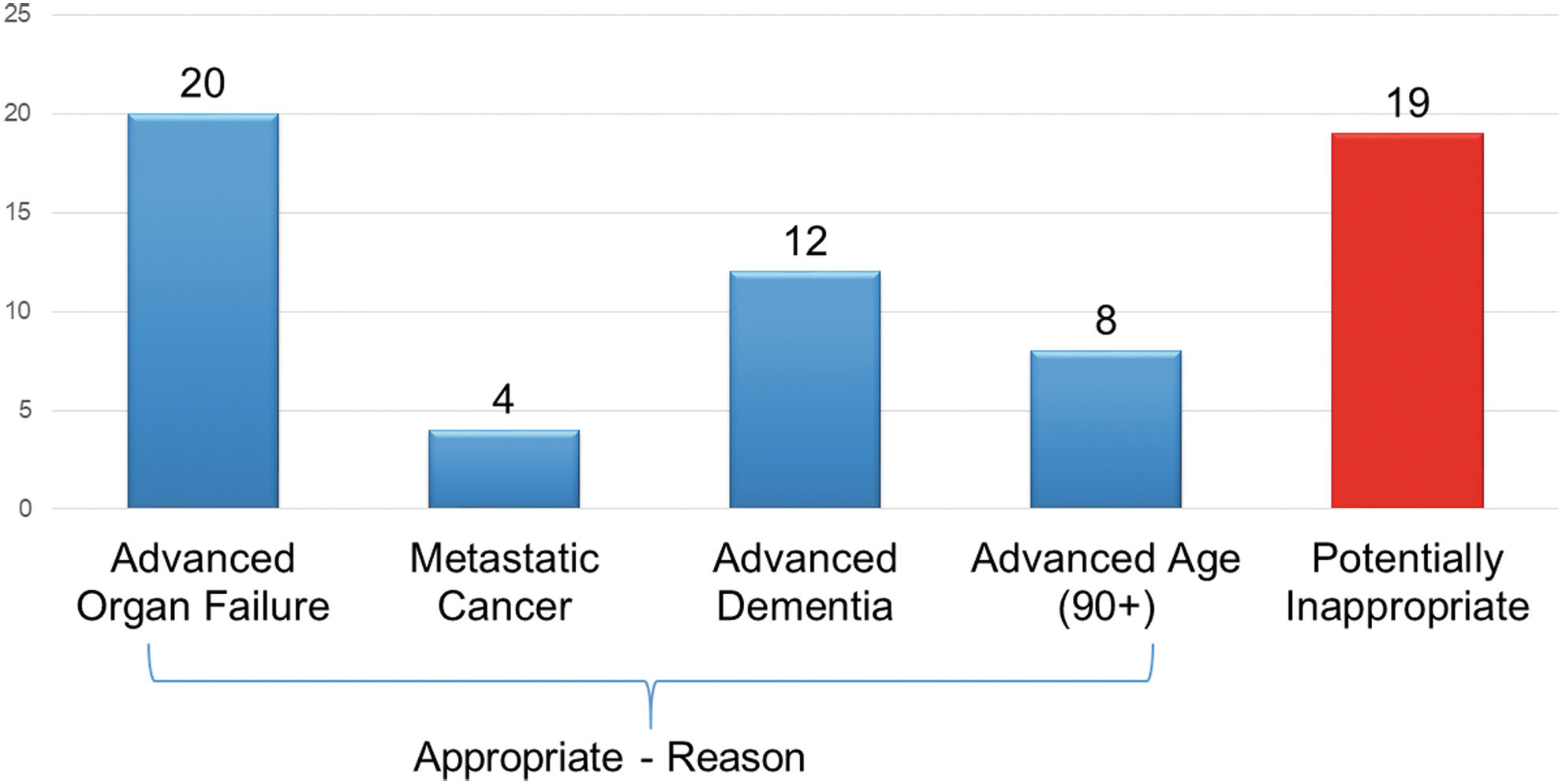
Appropriate use of POLST during an outpatient advance care planning billing visit (n = 63). Color image is available online.
In conclusion, among patients with an outpatient visit with ACP billing and a subsequently completed MOST, MOST utilization appeared appropriate for 70% of patients. These patients were older, more medically complex, and more frequent health care utilizers than individuals who were assessed as potentially inappropriate for MOST use. It is unknown whether the patient or provider initiated MOST completion. To our knowledge, this is the first attempt to operationalize criteria for potentially inappropriate use of a POLST Paradigm form. More research is needed to assess whether individuals with a MOST but without documentation of serious life-limiting medical conditions receive medical treatment that is discordant from their preferences or discordant from the MOST. Ongoing quality improvement efforts should also target provider education for appropriate use of the MOST.