
Abstract
Background:
Multidrug-resistant organisms (MDROs) are an important health care issue. Patients in Western societies often present an increased morbidity of chronic conditions accompanied by poor immune status and the use of devices. In particular, patients in palliative care (PC) are at greater risk of MDRO colonization, due to accompanying special devices and being hospitalized.
Objective:
To gain an overview of the literature regarding MDROs in PC.
Design
: Systematic review
Data sources
: On the 19th of October 2019 the databases “ PubMed” and “ CINAHL” were used to identify studies reporting on MDROs in PC; the search was updated on 16th of May 2020.
Results:
Seventeen out of 486 articles were included. Six represent qualitative data, 10 quantitative data, and one a mixed methods approach. Prevalence data range from 4.0% to 18%. MDRO colonization has a negative impact on patients and families. It leads to uncertainties and higher workload by staff members. Strategies for the management of MDROs in the field of PC are predominantly available for methicillin-resistant Staphylococcus aureus. Not even half of institutions utilize existing protocols. Recommendations for dealing with MDROs indicate required staff and time resources as well as information, communication, and specific knowledge.
Conclusion:
There is a great need for studies examining the prevalence of all MDROs in the PC setting. Additionally, not only patients but also a public enlightenment on MDROs should be provided to decrease knowledge gaps and therefore reduce transmission on MDROs.
Introduction
Multidrug-resistant organisms (MDROs) are increasingly important in health care settings. The main reasons for the increasing prevalence of patients with MDRO colonization are rising life expectancy, migration and travel attitudes,1,2 and the agricultural use of antibiotics.3,4 Concurrently, patients in Western societies have an increased morbidity of chronic conditions, which are accompanied by a poor immune status and the use of special devices like Percutaneous endoscopic gastrostomy tubes or urinal catheters. These patients are often hospitalized and are more likely to get colonized with MDRO. 5
Clinically relevant MDROs include Methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant Enterococci, and extended-spectrum β-lactamase-producing Gram-negative bacilli such as Escherichia coli and Klebsiella pneumoniae. 6
Dealing with MDROs is a challenge for everyone involved in the process of in-patient care. Staff members often have the dilemma of protecting themselves and third persons, while wanting to provide the best care for each individual patient colonized with MDROs. Inpatients colonized with MDROs are often isolated, or have other special hygiene measures that are applied to prevent transmission of MDROs.7,8 Several studies indicate that precautionary measures have diverse negative outcomes on the patient9–13 as well as on family members 14 and staff. 15 In particular, measures creating barriers between the patient and staff can lead to loneliness, stigmatization, depression, social exclusion, and fear by patients.9–12,16–18 In the field of palliative care (PC), these requirements are discordant to the main goal of PC.
PC is defined as “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness” 19 and intends social participation with the patients. 19 This aim interferes with measures to avoid transmission of MDROs, and discussion about whether precaution measures in end-of-life care are ethically acceptable or not is ongoing in the medical field.20–22
As many of these concepts are contradictory in practice, and no clear and consistent guidelines have been established, the aim of this systematic review is to obtain an overview of the existing literature regarding prevalence and impact of MDROs on PC as well as management approaches.
Methods
For this systematic review, a literature search to identify articles reporting on MDROs in the context of PC has been conducted. The study conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines. 23
On the 19th of October 2019, the databases “PubMed” and “CINAHL” were used to identify studies in English and German language; on 16th of May 2020 the search was updated. The search strategy is presented in Table 1 and was adapted for each database. Bibliographies of included articles were screened manually by two reviewers (A.E. and P.S.) to identify additional eligible studies.
Search Strategy (Exemplarily for PubMed)
ESBL, extended-spectrum β-lactamase; MRSA, methicillin-resistant Staphylococcus aureus.
To be eligible for inclusion, articles had to report on MDROs and PC. Articles reporting on MDROs in intensive care units, nursing homes, or long-term-care facilities; articles dealing with drug resistance in tuberculosis or human immunodeficiency virus; as well as articles reporting on the molecular epidemiology of pathogens or the efficacy of specific antibiotic therapies in patients who are colonized with MDROs were excluded. Conference articles, commentaries, and nonsystematic reviews were also excluded.
After exclusion of duplicate articles, all identified articles were screened independently by two authors (A.E. and P.S.) based on title and abstract for inclusion or exclusion. The full text of all articles that met the inclusion criteria were also independently assessed by A.E. and P.S. In cases where articles could not be accessed, authors were contacted to retrieve the full text. Any discrepancies in the assessment of inclusion and exclusion criteria were discussed until a consensus was reached. EndNoteX8 was used for data management.
All qualified articles were then scanned and rated regarding their quality by the Mixed Methods Appraisal Tool (MMAT), 24 a validated checklist to appraise the quality of studies with a quantitative, qualitative, or mixed methods approach, or the Joanna Briggs Institute Quality Appraisal Tool for studies reporting prevalence data. 25 An overall quality percentage score for each of the included studies was calculated, and the scores were interpreted as “low quality” (≤39%), “average quality” (40–79%), and “high quality” (80–100%).
Results
Seventeen articles met the inclusion criteria (Fig. 1) of which six present qualitative data,26–31 10 are based on quantitative data,14,32–40 and one used a mixed methods approach. 41
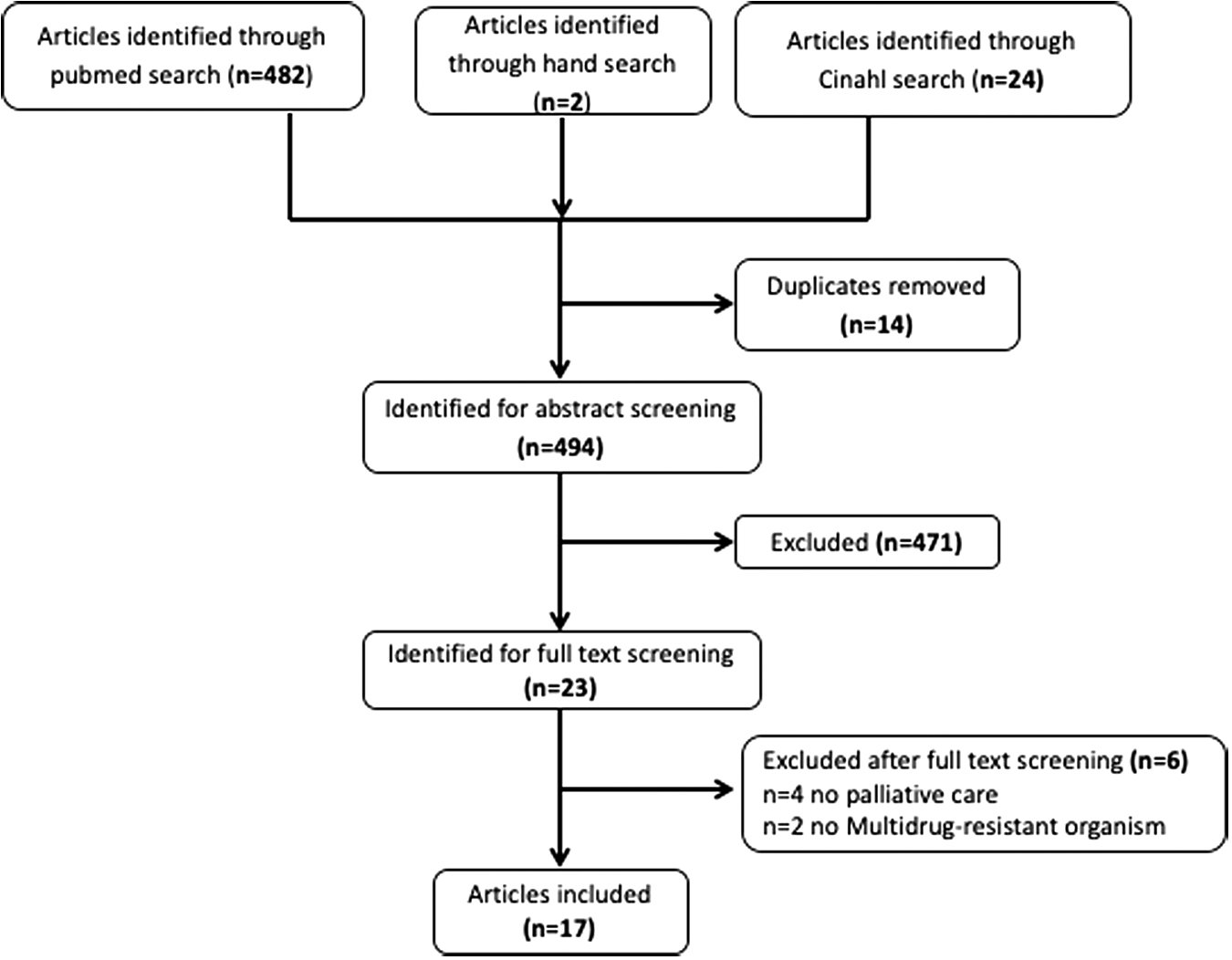
Flow chart of study selection.
Three articles were conducted in England,14,32,33 2 in the Republic of Ireland,30,36 1 study was conducted in Saudi Arabia 34 and 11 in Germany.26–29,31,35,37–41 Nine of the 15 articles targeted MRSA exclusively, and 8 focused on other MDROs as well. Two of the articles deal with pediatric PC. Table 2 presents detailed information about the included articles.
Characteristics of Included Studies
Joanna Briggs Institute Quality Appraisal Tool for studies reporting prevalence data.
Mixed Methods Appraisal Tool (MMAT).
MDRGNB, multidrug-resistant Gram-negative bacteria; MDROs, multidrug-resistant organisms; MRGN, multidrug-resistant Gram-negative bacteria; PCU, palliative care unit.
Prevalence of MDRO colonization in PC
Prevalence of MDRO colonization has been studied in eight articles.14,32–34,36–38,40 All but one conducted a systematic screening of MRSA only. 40 Two have been done retrospectively based on patient files.14,34 The other six articles are prospective studies, based on screening results at admission. Data of two articles were collected in hospices,14,33 four on PC units (PCUs),34,36–38 one on a pediatric PCU, 40 and one on PCUs and in hospices. 32
Prevalence of MRSA colonization in both adult and pediatric PCUs ranges from 4.1% to 11.6%34,36–38,40 (Table 3). The highest prevalence was found in the Republic of Ireland with 11.6%, 36 the lowest in Germany with 4.1%.38,40 Prevalence of MRSA colonization in hospices was similar to PCU, ranging from 4.0% to 8.0%.14,33 Dand et al. investigated both hospices and PCU and reported an MRSA prevalence of 4.3%. 32 Schmidt et al. 40 additionally reported prevalence data for multidrug-resistant Gram-negative bacteria (MDRGNB) (E. coli: 8.1%, Klebsiella ssp.: 1.6%, Proteus mirabillis: 1.6%, Enterobacter ssp.: 1.6%, Pseudomonas ssp.: 8.1%, Stenotrophomonas maltophilia: 5.4%, Acinetobacter ssp.: 5.4%, and Clostridium difficile: 1.6%) resulting in an overall prevalence of MDROs of 18%. Likewise Heckel et al. 38 reported prevalence data of MDRGNB, although based on an unsystematic screening; only if the MRSA culture of the nasal swab yielded the growth of Gram-negative bacteria, these cultures were also analyzed for MDRGNB and showed a prevalence of 4.1%.
Prevalence Data of Methicillin-Resistant Staphylococcus aureus Colonization
n = 15 admissions were infected with MRSA; because the number of total admission is not reported, prevalence could not be estimated.
Grouped using the classification of the “Association for Children with Life-threatening or Terminal Conditions and their Families (ACT).” ACT I: life-threatening conditions for which curative treatment may be feasible but can fail, in which access to palliative care services may be necessary alongside attempts at curative treatment and/or if treatment fails. ACT II: conditions in which premature death is inevitable, in which there may be long periods of intensive treatment aimed at prolonging life and allowing participation in normal activities, such as cystic fibrosis. ACT III: progressive conditions without curative treatment options, in which treatment is exclusively palliative and may commonly extend over many years, for example, Batten disease and muscular dystrophy. ACT IV: irreversible but nonprogressive conditions with complex health care needs leading to complications and likelihood of premature death; examples include severe cerebral palsy and multiple disabilities following brain or spinal cord insult. Craig F, Abu-Saad HH, Benini F, et al.: IMPaCCT: Standards for pediatric palliative care in Europe. Eur J Palliat Care 2007;14:109–114.
n.a., not available.
Impact of MDRO colonization/infection on patients and family caregivers in the field of PC
Six articles14,26,30,32,33,35 investigated the impact of MDRO colonization/infection on patients and their families. All but one 26 focus on MRSA. Three articles describe the impact of MRSA colonization/infection exclusively on the patient.32,33,35 One article details the impact of MDRO colonization of a patient on family caregivers 26 and two articles describe the impact of MRSA colonization on patients and family caregivers.14,30
Gleeson et al. 30 and Heckel et al. 26 reported that the reaction of patients and families regarding their MDRO diagnosis range from “not affected at all” to “shocked.” Furthermore, Gleeson et al. 30 identified that delayed information about the patients' MRSA diagnosis leads to dissatisfaction and distrust from patients and families toward physicians. Because medical staff are the main source of information regarding MRSA for patients, 30 timely knowledge of this condition is of great importance. Comprehensive information is especially important if patients do not have any previous knowledge about MRSA. 30 If patients perceive a delay in receiving information regarding their MRSA diagnosis, this leads to feeling that information had been held back. 30 How families deal with a MDRO infection of their relative is further influenced by the mostly negative reports about MDROs in the media.26,30
Isolation is a central strategy to deal with MDRO colonizations/infections. Challenges resulting from isolation measures for patients as well as for family members were described by five articles.14,26,30,32,33 Patients often felt “shocked,” “frightened,” or “distressed” due to isolation measures.14,30,33 Prentice et al. 14 stated that four families describe being “distressed” and one family being “horrified” by isolation measures due to MRSA. Heckel et al. 26 further reported family members feeling “rejected” and “excluded” due to isolation measures. Furthermore, patients and family members were worried about transferring MRSA to third persons.
The uncertainty of patients and families regarding MRSA is also affected by the lack of consistency in handling hygiene measures by different staff members. 26 Daily washing with mupirocin and the use of antibiotic treatment are common hygiene methods which lead to additional burden and cause variable side effects. 33
Being diagnosed with MDROs can have a variety of psychosocial impacts on not only the patient, but also their family and support network. As some patients and family members require psychosocial and emotional support regarding their MDRO colonization. 26 This is in line with results of Bükki et al. 35 and Dand et al. 32 who investigated that staff members of PCUs perceive an impact of MRSA on patients' quality of life. In PCUs, 83% and in hospices 55% of the staff members had the feeling of a decrease in patients' quality of life (social deprivation and emotional barriers) due to MRSA colonization or infection. 35
Impact of MDRO colonization on staff members
Eight articles27–29,31–33,35,41 examined the impact of MDRO colonization on staff members of PC teams. All eight articles concluded that MDROs are a challenge for staff members. Nearly all isolation measures were described as problematic, 28 inappropriate, 33 or in contrast to the aim of PC. 27 Four articles28,32,33,35 indicate increased difficulties regarding contact and communication with the patient, resulting in fewer interactions between staff and patient, 33 social deprivation of the patient, 35 and an emotional barrier. 28 Some staff members adhere to strict isolation measures; others suggest finding individual solutions for each patient, because strict protocols lead to more safety for the staff, but are difficult to define. Schmidt et al. 31 investigated the nurses' attitudes and opinions regarding a new hygiene concept for patients colonized with MDROs on a pediatric PCU, which counters the concept of strict, single-room isolation by means of strict barrier nursing. Results demonstrate that this represents a challenge for nursing staff and triggers ambivalence.
Four studies28,29,31,33 identified the challenge of a higher workload (e.g., putting on the extra gloves and gowns,28,31,33 different—mostly organizational—additional work like preparing a new room for colonized patients 29 ) treating patients with MDROs. Additionally, an emotional impact on staff members manifesting in difficulties in communication 31 and negative emotional reactions by patients and family members to the hygiene measures 28 and a lack of confidence in working with patients with MDROs by the staff 29 is recognized. Fear of transmission, lack of knowledge, and ambiguous opinions within the staff have been pointed out as reasons for uncertainty.
Impact of MDROs on the PC service
The impact of MDROs on the PC service is described in four studies.14,33,35,39 Three studies entitle problems regarding general resources referring to MRSA.14,33,35 If a colonization with MRSA is confirmed before admission, lack of single rooms,14,33,35 personnel shortage, 33 or special cleaning after discharge14,35 are named as reasons for a delay or a barrier to admission. Furthermore, the financial impact as costs for gloves, plastic aprons, antibiotics, special cleaning, and diagnostic test are reported.14,33 There is one study 39 dealing with the financial impact of the occurrence of MDROs on a PCU, which depicts that patients who are colonized with MDROs caused on average higher total costs of 1,228.87€ (US$ 1,361.61) per stay. 39 Particularly regarding the costs for nursing services, higher costs (€463.62; US$ 418.41) were incurred for patients with MDROs. Interestingly they identified higher cost for younger patients (age 25–69).
Managing of MDROs in the PC setting
Five articles target management of MDROs in a PC setting.14,31–33,35 All but one 31 focus on MRSA only. Two studies32,35 carried out a survey aimed to investigate the handling of MRSA in PCU as well as in hospices. More than 90% of the participating PCU and hospices have established MRSA containment guidelines (MRSA protocols)14,35 (Table 4).
In Germany, patients identified with MRSA are isolated in 99% of PCU and 76% of hospices. Twenty-one percent of the hospices stated that they do not isolate MRSA-positive patients due to ethical reasons compared with 1% of the PCU. 35 Additionally, 96% of the PCU in Germany restrict access to common areas for most MRSA-positive patients. Only 66% of the hospices in Germany report such a restriction. 35 Forty-six percent of the responding institutions in England had a similar restriction for MRSA-positive patients. In 12.5% restriction measures apply to all MRSA-positive patients, whereas mostly patients with uncontrolled infection were restricted. 32
Regarding the information and education of the patients in case of an MRSA colonization/infection, 82% of PCU in Germany provided specific background information to the patients (67% oral; 41% written) as did 67% of the hospices (56% oral; 23% written). Dand et al. 32 reported that 84% of the institutions in England provided background information on MRSA to the patients, mostly oral. If patients were infected rather than colonized more information was provided. 32
Treatment regimens vary between institutions. 35 In 71% of the PCU and 57% of the hospices in Germany, treatment was attempted. Dand et al. 32 identified that in 36% of infected patients, treatment was attempted in both PCU and hospices. In another study in three English hospices in England, treatment was attempted in 55% to 67% of admitted patients colonized/infected with MRSA. 14 Both surveys reported on obligatory precautionary measures for staff members while caring for patients who are colonized with MRSA. In 59% of the participating institutions in England, special training for staff was performed. 32 In Germany, in 27% of the PCU and 9% of the hospices, an MRSA screening was offered to staff. 35 The use of precautionary measures for visitors is recommended in 98% of the PCU as well as hospices in Germany, 35 whereas 71% of the participating institutions in England report that visitors must use precautionary measures. 32
Five articles describe recommendations regarding management of MDROsin end-of-life care.26,28–30,41 Heckel et al. 41 identified five themes for managing hospitalized management of MDRO carriers in end-of-life care: (1) strategy for dealing with MDROsat end of life, (2) MDRO diagnostic and therapy, (3) required accommodation facilities, provided material as well as staff and time resources, (4) social inclusion, and (5) information, communication, and knowledge.
Staffing resources and knowledge are a consistent theme. Concerning the adjusted work load in the presence of MDROs, adjusted working routines for the staff caring for patients colonized with MDROs are recommended.28,29,41 One pragmatic strategy for handling MDROs in PC is identifying one staff member responsible for all questions regarding MDROs, 41 especially questions regarding diagnostics and therapy. Heckel et al. 41 and Gleeson et al. 30 also suggest an early identification of colonized patients and a comprehensive elucidation about therapeutic possibilities for patients and families, including consequences, and risk assessment is also suggested.30,41
Social inclusion of the patient colonized with MDROs is also recommended for best management of patients with MDROs in the PC setting. Schmidt et al. 31 describe a hygiene concept, in which social inclusion is a main goal without neglecting infection control. First, MDROs should not be a reason to refuse admission of a patient. Resources, including additional working time, information resources, and single rooms, should be provided. 29 Second, the circumstances in which colonized patients are able to leave the room should be clarified. Affected patients should have all therapeutic possibilities that other patients experience. 31 To avoid stigmatization, information should be provided to patients, families, and staff.29,31 The importance of available information on MRSA and the implications of colonization for patients and families has been pointed out by three studies.26,30,31 Gleeson et al. describe, one third of patient-reported leaflets were a helpful tool in increasing their understanding of MRSA. 30
Finally, studies have identified that it is important to offer all team members the option to discuss their fears regarding managing patients with MDROs. 29 Two studies describe formats for staff training.29,41 A traditional approach of “simplification” of the hygiene rules are seen as necessary to reform the handling of MDROs in end-of-life care. 41 Alternatively, a new format of training for staff—“shared decision making” with the family, the patient, and the staff is suggested.29,41 In addition to these approaches, staff meetings and notes in the patient file are suggested to clarify the identified hygiene measures for each individual patient. 29
Discussion
This systematic review provides an overview of MDROs in PC patients. Seventeen articles of varying quality and with different study designs were eligible for inclusion. Main topics identified were prevalence data of MDROs, impact of MDROs on patients and families, impact of MDROs on staff members, impact of MDROs on the PC service, and managing MDROs in the field of PC.
Two important observations were made. First, all but one systematic prevalence study and all but one article dealing with the management of MDROs in end-of-life care, refer to MRSA only. In recent years, the prevalence of MRSA appears to be stable, yet other MDROs, such as MDRGNB, have increased in prevalence. 42 Only Schmidt et al. 40 investigated MDROs other than MRSA systematically. It can thus be assumed that the actual prevalence of MDRGNB is much higher. In 2017, the WHO published a “global priority list of antibiotic-resistant bacteria,” in which the bacteria were classified in “critical,” “high,” and “medium.” 43 Although MRSA is classified as “high” and Pseudomonas aeruginosa, Enterobacteriaceae, Acinetobacter baumanii, or Vancomycin-resistant Enterococcus faecium as “critical,” no studies exist regarding the management of MDRGNB or Vancomycin-resistant Enterococcus faecium in end-of-life care. Second, all studies included in this review were conducted in Europe and Saudi Arabia, with none from North America. The problem of MDROs seems to be well known in this region as the US Center for Disease Control 44 released a guideline on the Management of MDROs in Healthcare Settings in 2006. Nevertheless, no trial or study has been performed in North America regarding the prevalence of MDROs, the difficulties, infection management strategies, or the impact on patients, families, and staff regarding MDROs in the field of PC.
Prevalence data of MDROs in this review ranged between 4.0% and 18%. Due to methodological differences, the data extracted in this review cannot be compared. Most studies screened patients with risk factors only. This may underestimate the prevalence as studies screening all patients reported higher prevalence rates.36,37,40 Time frame, sample size, and type of life-limiting diseases are unclear and lead to discordant data. To get an accurate estimate of MDROs in the PC setting, multicenter studies examining all patients on admission for colonization with MDROs are urgently needed.
Results of this systematic review indicate a great negative impact of MDRO colonization/infection on palliative patients and their families. In particular, as the negative impact of isolation and contact precautions for patients in PC settings is well known,10–12,21 only one 31 of the included articles specify the isolation measures used. Staff members enter isolation rooms less frequently and there is less contact between staff and affected patients. 45 Additionally, patients with isolation management strategies, such as contact precautions, are more often confronted with preventable adverse effects. 46 Moreover, the use of contact precautions is not based on high-quality, evidence-based data,22,47 yet it is recommended by scientific societies and governmental authorities. Accordingly, there is an ongoing discussion in the field of PC whether contact precaution is the most effective and appropriate measure to prevent transmission of MDRO. 46 This discussion appears to be a particular challenge in the field of PC and requires further consideration. The introduction of more liberal hygiene concepts, such as those described by Schmidt et al., 8 will enable patients to participate more in everyday ward life. Even seemingly simple strategies, such as leaving patient doors open and entering the patient room without protective clothing, are seen as a great improvement in quality of life. 31
However, it is difficult to confirm the unique role of contact precautions, 48 as it is usually only one measure in a complex infection prevention program. Accordingly, Landelle et al. 46 suggest “multimodal strategies, variably combined,” including hand hygiene, barrier precautions, and appropriate environmental cleaning. The US Center for Disease Control and Infection considers hand hygiene as the most important issue to reduce spreading of MDROs. 44 Despite this, compliance for hand hygiene remains low.49–51
Special requirements of PC patients need to be included while considering whether contact precautions are a reasonable procedure or not. All isolation measures need to maintain the “dignity and privacy of every patient.” 52
Furthermore, patients colonized/infected with MDROs have economic consequences for the institution. Additional costs for preventing transmission, structural improvement such as single room availability, complicated therapy of MDROs, and nursing care costs have to be covered.9,53,54 Isolated patients had 23% higher cost of care 9 and colonized patients caused higher total costs per stay, 39 as well as younger patients who are colonized caused higher total costs. 39 Unfortunately, reasons for this discrepancy have not been discussed.
Results further identified a lack of information provided to patients with MDROs and their families. In cases where information was provided, a knowledge gap about MDROs26,30 as well as different handling of the hygiene measures by the staff leads to uncertainty in patients, family, and staff alike. 26 Due to the fact that several international studies show a general lack of knowledge and understanding of antibiotic resistance,55–59 this is not likely due to specific circumstances within the PC setting. A recent study from the US National Science Board illustrates that only 51% of US Americans and 46% of Europeans answered the question, “Antibiotics kill viruses as well as bacteria”correctly. 60 Santos et al. 52 indicate that there is a need for clear communication and education of staff and the patients colonized or infected with MDROs. Furthermore, public education on MDROs would reduce transmission of MDROs more broadly.
Significant uncertainty by staff members regarding MDROs28,31–33,35,61 has also been identified. Herbst et al. 29 and Heckel et al. 41 recommend a “simplification” of hygiene rules, however they do not describe what the simplification should entail. At the same time, both studies show a wide difference in the perception of hygiene rules and patient care perceived by staff members. On the one hand, there is a need for precise hygiene rules to simplify the implementation. On the other hand, due to precise hygiene rules, individual patient care will be hindered.29,41 Schmidt et al. 31 depict that, although it is challenging and triggers ambivalence by the nurses, the implementation of a complex hygiene concept which counters the concept of strict, single-room isolation and allows social participation, is feasibly; not least due to the advantages of the hygiene concept that can be easily integrated into the daily routine of the unit (e.g., possibility to leave a patient's room doors open despite MDROs).
Regarding the management of MDROs in the PC setting, it is alarming that not even half of the institutions utilize existing protocols. 35 This might indicate that there is a need for individual solutions regarding contact precautions for PC patients colonized with MDROs 52 as well as for a reporting system to have more data.
One reason why treatment regimens for patients with MDROs vary widely between PC institutions might be the direct link between workload and bed occupancy. 62 Diagnostic testing and antimicrobial therapy are further described as great risk factors for MDROs in the PC setting.20,63 Likewise, Landelle et al. 46 assume the high rate of MDROs to be a consequence of inappropriate antimicrobial prescription. Therefore, the decision to initiate an MDRO therapy with antimicrobials is challenging. First, diagnostic data are often difficult to obtain and interpret and it may be more appropriate to avoid sending microbiological specimens in the PC setting. 20 Second, for frail patients with advanced disease, the risk of antimicrobial therapy is not trivial. Adverse outcomes may include drug reactions, drug/drug interactions 63 and side effects, such as nausea or neurotoxicity. 20 Third, the administration of antimicrobials is burdensome, leads to further discomfort of the patient, and is discordant with the goal of PC to maintain quality of life. 20 The goal of care should be discussed with the patient20,63 and family members and patients should be educated about potential benefits as well as risks and burden of treatment. 63
Concerning the recommendations for dealing with MDROs in the PC setting, it is suggested to provide staff training and education for everyone involved in the care process as well as an annual summary of the experiences with MDROs and a standardized reporting system.30,41,44 Additionally, education is required to both disseminate basic information and to encourage compliance with infection-control measures. 64 Contrary to this, Datta and Juthani-Mehta 20 recommend infection prevention groups to consider the removal of contact precautions from PC settings altogether to avoid social exclusion for patients facing the end of life. While this suggestion has a strong focus on the ethical consequences of isolation, patient safety also needs consideration. Therefore, a balanced concept avoiding isolation but also guaranteeing patient safety would be desirable.
Strength/limitations
The main strength of this systematic review is its novelty and its relevance for patient care. However, the findings should be interpreted in light of the following limitations. The identified studies were of varying quality and used a wide range of study designs and research objectives, restricting analysis to a qualitative format. Additionally, only studies published in English and German were included, resulting in relevant studies published in other languages not being considered.
Conclusion
There is an urgent need for (1) studies examining all patients on admission to obtain exact prevalence rates of MDROs in the PC setting, (2) recommendations about how to best deal with MDRO-colonized patients receiving PC at home, in hospices, and on PCUs, and (3) a public education about MDROs, transmission and protective strategies to decrease knowledge gaps and, therefore, reduce transmission on MDROs.
Data Management and Sharing
The datasets used and analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgment
The authors thank Donnamay Brown for English editing.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Disclosure Statement
No competing financial interests exist.