
Abstract
Background:
A broad consensus on the optimal structure, intensity, and timing of early specialist palliative care (SPC) intervention is lacking.
Objective:
To evaluate the benefit of an early and systematic palliative intervention alongside standard oncology care compared with standard oncology care alone in patients with advanced solid tumors.
Design:
PALINT, a single-center RCT, conducted at the Masaryk Memorial Cancer Institute, the largest comprehensive cancer center in the Czech Republic (CR).
Setting/Subjects/Measurements:
Patients with newly diagnosed advanced cancer within six weeks from the start of the palliative systemic therapy were randomly assigned to the integration of SPC (intervention; a consultation with a PC physician every six to eight weeks) or to the standard oncology care (control). The primary endpoint was the quality of life (QOL) assessed by EORTC QLQ C30 and Hospital Anxiety and Depression Scale (HADS) at three and six months.
Results:
From 2015 to 2017, a total of 126 patients were randomly assigned to intervention (60) or to control (66) arm. At baseline, at three and six months, the global QOL scores (mean, 95% CI) in the intervention and control arm were 58.6 (53.9–63.3), 61.9 (56.4–67.4) and 66.7 (60.2–73.2) versus 54.2 (49.4–58.9), 59.0 (53.7–64.3), and 62.8 (56.7–68.9), respectively. The prevalence of anxiety (HADS-A; value >7) was 36.7%, 27.5%, and 18.9% versus 34.8%, 23.5%, and 16.3% and the prevalence of depression (HADS-D; value >7) was 28.3%, 25.4%, and 29.7% versus 28.8%, 29.4%, and 27.9%, respectively. There was no significant difference between the two arms. The overall survival was similar in both arms (347 vs. 310 days; p = 0.203).
Conclusions:
A model of early integration of SPC consisting of a consultation with a PC physician alone every six to eight weeks did not increase the QOL of patients with advanced cancer compared with routine oncology care in a center with widely available supportive services. These negative results underline the importance of the multidisciplinary patient centered approach in the early SPC.
Introduction
During the last decade, a number of randomized controlled trials carried out in the United States, Canada, and Europe have demonstrated the benefit of early integration of palliative care (EPC) into standard oncology care in patients with various types of advanced cancer.1–9 The EPC model has shown a positive impact on the quality of life (QOL), satisfaction with care, understanding of illness and prognosis, and it was associated with less caregiver distress, equal or better survival, and equal or lower costs. EPC has been implemented in many international oncology guidelines (e.g., ASCO, NCCN) as a new standard of care.10,11 The type and range of specialist palliative interventions (alongside standard oncology care) varies across the studies: in some studies the interventions are delivered by a multidisciplinary palliative team,1,2 in other studies they are provided by a PC physician alone and other professionals are only involved when indicated by the physician, 12 and in other studies they are provided by a nurse.3,4,9 Palliative intervention primarily consists of an in-person consultation or appointment.1,2 Some studies also include telephone sessions. 3 The frequency of regular visits with a palliative team range from weekly to monthly visits. In addition to these scheduled visits, some studies also enable an on-demand consultation, if requested by the oncologist or other members of primary team, the patient, and/or her family.1,9
In the Czech Republic (CR) pain and nutrition specialists, psychologists, social workers, and spiritual care providers are available to patients and their families at most oncology centers as part of the routine oncology care. These services are usually not looked at as the part of palliative care but as the supportive care. The capacity of supportive/palliative care services and their actual availability to patients varies greatly between the cancer centers. Palliative care is predominantly perceived as end-of-life care, and thus, patients are usually referred to palliative care specialist when all options of anticancer treatment had been exhausted. The concept of EPC has not yet been generally accepted and implemented into oncology practice in the CR.
Masaryk Memorial Cancer Institute (MMCI), the largest comprehensive oncology center in the CR, has 254 beds, 10,580 annual admissions, 161,800 outpatient consultations, and 130 in-patient deaths per year. Psychosocial supportive team has five psychologists, two full-time and one part-time social worker, and one part-time chaplain. Such staffing is above average compared with other oncology centers in the CR. At MMCI, the Outpatient Clinic of Supportive and Palliative Oncology has been operating since 2006 and provides mostly outpatient care. Patients are usually referred to the clinic by their oncologists after the decision to forgo the anticancer therapy had been made. Inpatient consultations for patients still treated by oncological therapy are requested only occasionally. The clinic is run by a physician (palliative care specialist) and a nurse and cooperates closely with psychologists, social workers, and a chaplain.
In this setting, where standard oncology care includes psychosocial and spiritual support, it is not known whether early and systematic integration of specialist palliative care (SPC) could have added effect on the quality of life of patients. Therefore, we did a randomized controlled trial (RCT).
Methods
Study design and participants
PALINT is a single-center unblinded RCT conducted at the Masaryk Memorial Cancer Institute. PALINT compares the model of early integration of SPC into standard oncology care to standard oncology care alone. The study included adult (≥18 years old) patients, with ECOG performance status 0–2, with newly diagnosed advanced lung carcinoma, pancreatic, gastric, or head and neck cancer who had recently started the first line of nonurative (palliative) anticancer treatment, and patients with colorectal carcinoma treated with the third or higher line of systemic therapy. Patients were eligible within six weeks after the initiation of palliative systemic treatment. Both outpatients and inpatients were considered for inclusion. Primary oncologists were asked to inform their patients about the trial and to refer patients interested in participation to a study coordinator nurse. Several workshops were organized for the oncologists about the concept of EPC and the study design and oncologist were given a special reminder card with summary of the study design and the eligibility criteria before the study initiation. Coordinator nurse (experienced clinical research assistant) checked the eligibility of referred patients and informed them in detail about the study. Consented patients were subsequently randomized by a study coordinator nurse in a 1:1 ratio to the intervention arm (systematic palliative care + standard oncology care) or to the control arm (standard oncology care within a computer-based randomization tool using single sequence of random assignments. The Ethical Committee of the Masaryk Memorial Cancer Institute approved the study protocol; the study coordinator described the study to patients, and all participants provided written informed consent.
Procedures
The palliative intervention consisted of consultation with palliative care physician every six to eight weeks. Consultations included pain and other symptom assessment made by the Edmonton Symptom Assessment Scale (ESAS), assessment of patient's coping strategies and the need for psychosocial support. The average duration of the first visit with a palliative care physician was 45 minutes, follow-up visits took ∼20 minutes. Besides pharmacological symptom management recommendations, a palliative care specialist also explored patient's individual psychological and spiritual needs and referred them to other members of the team (social worker, psychologist, or chaplain) when an unmet need was discovered. In the control arm, an on-demand consultation with palliative care physician as well as other supportive/palliative services requested by the treating oncologist were available. The study appointments with PC physician had usually the character of a consultation (recommendation about symptom management had been given to primary oncologist). In some patients comanagement model had been practiced (PC physician directly prescribed medication for pain/non-pain symptoms).
Study outcomes
The primary endpoint was the quality of life assessed by the European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire Core 30 items (EORTC QoL C30) and the Hospital Anxiety and Depression Scale (HADS) at baseline and three and six months after randomization. Secondary outcomes included overall survival, use of anticancer treatment in the last 30 days of life, enrolment in hospice services, and place of death. Quality-of-life questionnaires were completed by patients alone or with the assistance of a nurse.
Statistical analyses
We planned to enroll 300 patients (150 in each arm). With 25% loss to follow up, this would provide more than 95% power to detect a standardized mean difference of 0.5, which is considered to be a medium effect size. Due to low patient accrual, it was decided to stop the enrollment after 126 patients had been randomized, which would still assure power of 80%. Standard descriptive statistics are used for the description of the data. Continuous variables are described using mean and standard deviation or 95% CI; categorical variables are described using absolute and relative frequencies of categories (percentage). Statistical significance of differences between interventional and control group is tested by Fisher exact test for categorical variables and by t-test for continuous data. Overall survival is presented by Kaplan–Meier curve and difference between groups was tested by log rank test. The results were considered statistically significant at the level of alpha <0.05 in all applied analyses. Analyses were performed using IBM SPSS Statistics 25.0.0 (IBM Corporation, 2017).
This publication discusses the results of PALINT study with regard to its primary outcome, that is, the impact of EPC interventions on quality of life in the first six months of cancer treatment. Follow-up visits and interventions are still ongoing and a detailed presentation of secondary outcomes will be the subject of a separate publication.
Results
Study population
Between September 1, 2015 and December 31, 2017, 156 out of 543 potentially eligible patients were referred by their oncologists to participate. One hundred twenty-six out of 156 patients consented to participate and were enrolled. Thirty patients refused to participate. Sixty patients were randomly assigned to the interventional arm and 66 patients to the control arm (Fig. 1). Gender, age, performance status, and diagnoses were well balanced across both study arms (Table 1)
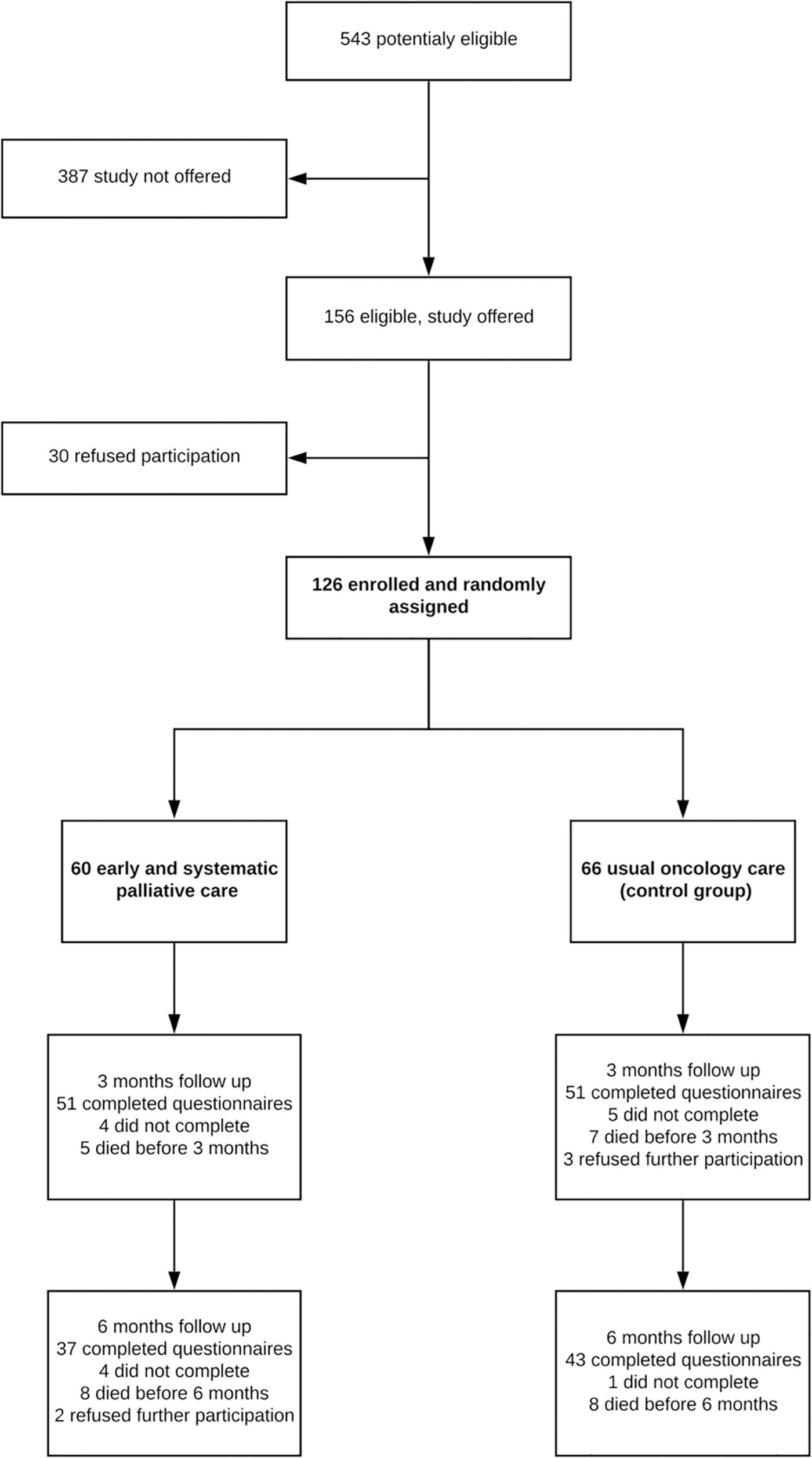
Trial Profile.
Baseline Characteristics of Patients
Categorical data are described by absolute and relative frequency. Age is described by mean and SD.
Statistical significance of difference between groups of patients is tested by Fisher exact test for categorical data and t-test for age.
The adherence to protocol in the intervention arm (number of palliative consultations effectively carried out according to the protocol: number of consultations predefined by the protocol) was 72%, with 50 (83.3%) patients having 100% adherence (Table 2).
Number of Consultations
Categorical data are described by absolute and relative frequency. Statistical significance of difference between groups of patients is tested by Fisher exact test for categorical data and t-test for age.
Bold values indicate that the difference between the study arms reaches the p value inferior to 0.05 (i.e., statistical significance).
The number of consultations with palliative care specialist and social worker was significantly higher in the intervention arm. The number of psychological supportive interventions was similar in both study arms. Thirty one (43%) patients in the control arm had at least one consultation with palliative care specialist during the study period and 12 (18%) patients had even more than 3 consultations (Table 2). The proportion of patients having completed the QoL questionnaires after three and six months was 85% and 61.6% for the interventional arm and 77.3% and 65.2% for the control arm, respectively.
Quality of life
The overall quality-of-life scores at baseline, after three and six months were 58.6 (95% CI 53.9–63.3), 61.9 (56.4–67.4), and 66.7 (60.2–73.2) in the intervention arm and 54.2 (49.4–58.9), 59.0 (53.7–64.3), and 62.8 (56.7–68.9) in the control arm. The effect size was 0.2. The differences between groups were not statistically significant. The analysis of specific subscales of the EORTC QoL C30 questionnaire (pain, dyspnea, fatigue, emotional functioning, social functioning etc.) did not show any significant difference between the interventional and control arm, providing a clinically significant change that is considered to be a difference of ≥10 points on a given scale (Table 3).
Mean Scores in Quality of Life and Functioning Scales of the EORTC Quality of Life C30
EORTC QLQ C30 = European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire version 30.
Variables were described by mean and 95% CI. Statistical significance of difference between groups were tested by t-test.
Patients' overall distress (HADS-total), anxiety (HADS-A), and depression (HADS-D) scores at baseline, three, and six months did not differ significantly between study groups (Table 4). The prevalence of clinically significant anxiety (HADS-A score >7) at baseline, after three and six months was 36.7%, 27.5%, and 18% in the interventional arm and 34.8%, 23.5%, and 16.3% in the control arm, respectively. The prevalence of clinically significant depression (HADS-D score >7) was 28.3%, 25.4%, and 29.7% in the interventional arm and 28.8%, 29.4%, and 27.9% in the control arm, respectively. There was no significant difference in the prevalence of anxiety and depression between the groups (Table 5).
Mean Values (Range) of Hospital Depression and Anxiety Scale
Variables are described by median and rank.
Statistical significance of difference between groups of patients is tested by Mann–Whitney U test.
HADS, Hospital Depression and Anxiety Scale; HADS-A, subscale for anxiety; HADS-D, subscale for depression.
Prevalence of Clinically Significant Anxiety (HADS-A > 7) and Depression (HADS-D > 7)
HADS-A cutoff >7, HADS-D cutoff >7.
Categorical data are described by absolute and relative frequency. Statistical significance of difference between groups of patients is tested by Fisher exact test.
Overall survival
By the end of data collection in December 2018, 98 patients had died (78%), 46 (76.7%) in the interventional arm, and 52 (78.7%) in control arm. The overall survival from the randomization in the intervention and control arms was 347 days and 310 days, respectively. The difference was not statistically significant (p = 0.203) (Fig. 2).
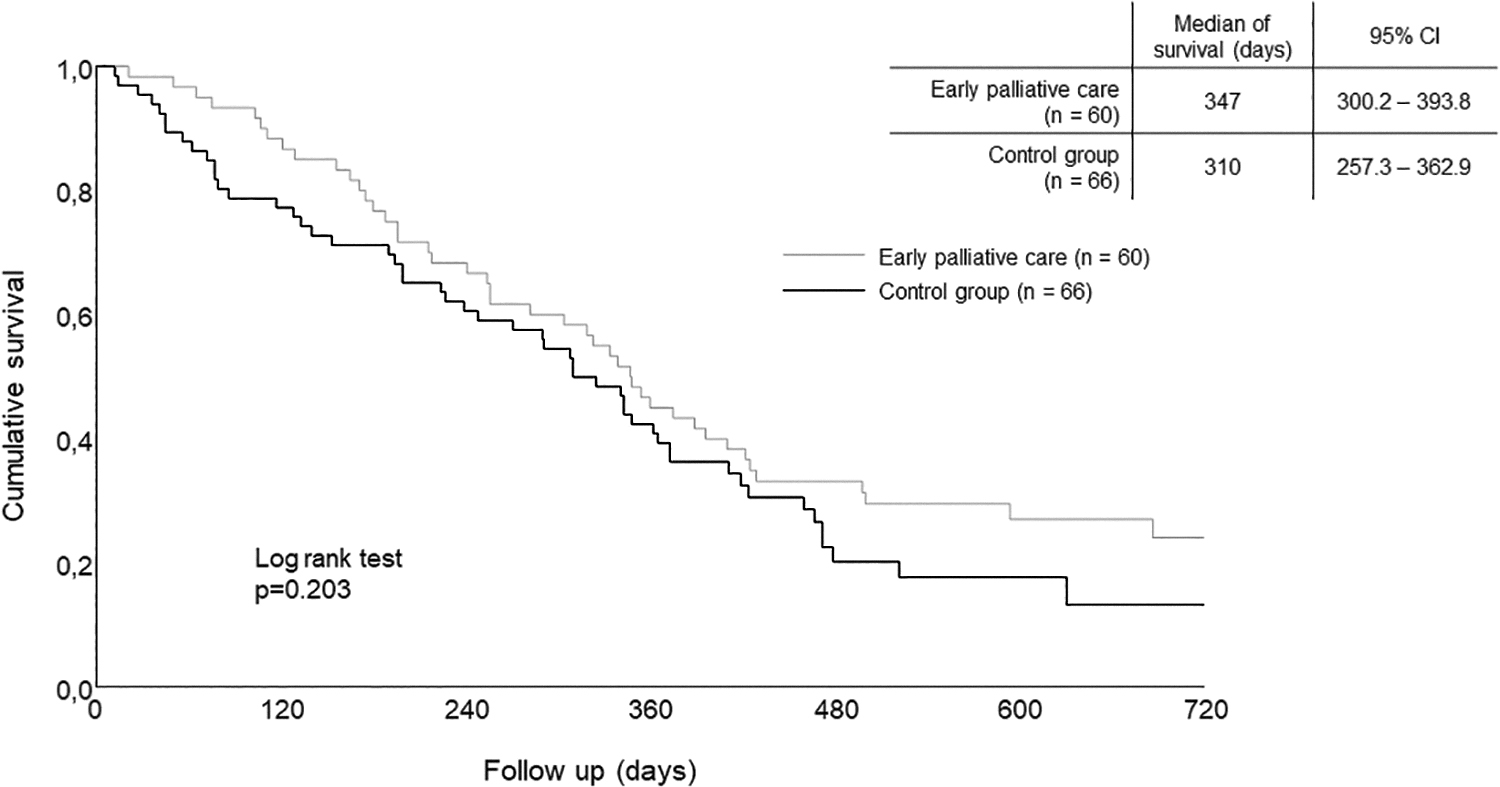
Kaplan–Meier estimates of the overall survival measured since the date of random assignment. CI, confidence interval.
Discussion
The PALINT trial did not demonstrate a statistically significant improvement in quality of life in the arm with early specialist PC integration model compared with the standard oncology care. These findings contrast with several other American studies with similar design that have proved a benefit of early integration of SPC for patient-reported outcomes, including quality of life.1,3 Two major European studies, however, have also yielded ambiguous results. The Danish Palliative Care Trial 8 failed to prove the benefit of early integration of SPC on the quality of life in patients with a predefined level of needs according to specific subscales of the EORTC-QLQ-C30 questionnaire. A Belgian study 9 showed an improvement in the overall quality of life measured by EORTC-QLQ-C30 scale (difference of 7.6, p = 0.03) and better outcomes in particular subscales such as overall physical functioning, fatigue, or cognitive functioning. The study also proved a positive impact of EPC on the existential wellbeing of patients assessed by a single-item MQOL (McGill Quality-of-Life Questionnaire). However, these changes in EORTC-QLQ-C30 subscales did not reach the 10-point difference usually considered as minimal for a clinically significant difference.
There may be several possible explanations of negative results of our study. It might be due to relatively low intensity and comprehensiveness of the chosen form of palliative intervention. The consultation with a palliative care physician alone may not have sufficiently addressed particular determinants of patients' quality of life, such as psychosocial and spiritual needs. It is also likely that the frequency (six to eight weeks) of palliative care visits was too low to achieve any clinically meaningful benefit. From this perspective, palliative intervention in the PALINT study could be characterized as “low dose” in terms of its complexity and frequency. Our results suggest that the intensity and optimal form of integrated SPC into routine oncology practice should be investigated.
Another possible cause of the negative results may be a relatively high quality of supportive and palliative care available within standard oncology care at the Masaryk Memorial Cancer Institute with no major differences it the utilization psychosocial services between the intervention and control arm. Proportion of patients in the control arm who had at least one consultation with palliative care specialist during the study period was relatively high (47%). This may have diluted the impact of our “low-dose” palliative care intervention. Our study has been struggling from the very beginning with low patient accrual and failed to achieve the target number of 300 participants. The proportion of patients referred to the study by their primary oncologists accounted for less than 30% of all eligible patients treated during the enrollment period at our institution. The reasons for oncologists' reluctance to enroll patients were a subject of further inquiry. Palliative care is in the CR predominantly perceived as the end-of-life care. So far, the concept of early PC has not been widely recognized and despite vigorous discussions in the oncology community, it is still far from being unequivocally accepted. Specifically, the debate is often confined to a linguistic aspect of the problem and reflects an earlier controversy over the relationship between the concepts and terms “supportive care” and “palliative care.”13–16
Low accrual was also probably caused by the way of referral we had chosen. Referral was based on the primary oncologists who were asked to inform the patients about the trial and to refer patients interested in participation to a study coordinator nurse. Many oncologists regard discussions about cancer diagnosis, prognosis, and treatment goals, as well as the management of cancer-related symptoms and side effects of anticancer therapy as an integral part of their clinical work. On the other hand, some oncologists consider early communication of unfavorable prognosis and promotion of palliative care during an active anticancer treatment as potentially burdensome and traumatic to patients. This raises the question if those two groups of physicians referred the patients to our project similarly or if there were any differences, which could lead to a specific type of bias. But these are poorly measurable and will be the subject of the further research. Perhaps a system of automatic referrals or triggers for referral could have improved the enrollment and eliminate this potential bias.
There may also have been barriers on the patients' side. A relatively high proportion of patients (30/156) who were referred to the study by their oncologists refused to participate after reading the informed consent. Reasons for refusal included concerns about additional medical visits, waiting time for a palliative consultation, worries that an early onset of palliative care will result in premature withdrawal from anticancer treatment, and also some patients' view that they have no problems that require a palliative care consultation. Our study has confirmed barriers and misconceptions about the concept of EPC on the side of oncologists and patients described by others authors.17–19
Conclusion
Our clinical trial failed to prove clinical benefit of the chosen low-intensity model of early SPC integration. This negative result, however, certainly does not undermine potential benefits of early involvement of palliative care into oncology practice. It indirectly supports the notion that palliative care to substantially improve the quality of life and overall experience of advanced disease needs to be sufficiently comprehensive and holistic and can only be provided by a multidisciplinary team. To find the optimal form of EPC into comprehensive oncology care the future studies should aim at better description of roles and responsibilities among SPC team, primary oncologists, and general practitioners in the management of palliative agenda during the whole advanced disease trajectory.
Footnotes
Funding Information
Supported by the Ministry of Health of the Czech Republic: Grant number 15-33590A and RVO (MOU, 00209805).
Author Disclosure Statement
No competing financial interests exist.