
Abstract
Background:
Early integration of palliative care (PC) for patients with heart failure (HF) improves patient outcomes and decreases health care utilization. PC provided outside of an acute hospitalization is not well understood.
Objective:
To synthesize the literature of outpatient PC in HF to identify the current landscape, the impact on patient health outcomes, key stakeholders' perspectives, and future implications for research and practice.
Design:
A systematic search of PubMed, Embase, CINAHL, Cochrane, and Web of Science was conducted from inception to February 2019 for studies of outpatient PC in adults with HF. Each study was analyzed to describe study characteristics, location of PC, types of providers involved, participant characteristics, and main findings, and to characterize domains of PC addressed.
Results
: Most studies (N = 19) employed a quantitative design and were conducted in the United States. The most common locations of PC were the home or PC clinic and providers were mainly PC specialists. Outpatient PC improved quality of life, alleviated symptoms, and decreased rehospitalizations for patients with HF. No study addressed all eight domains of PC. The structural, physical, and psychological domains were commonly addressed, whereas, least commonly addressed domains were the cultural and ethical/legal domain. Women and ethnic minorities were underrepresented in the majority of samples.
Conclusions:
This integrative review highlights the need to promote primary PC and future PC research focusing on a holistic, integrated, team-based approach addressing all domains of PC in representative samples.
Introduction
Approximately 6.2
Palliative care is an effective approach to manage symptoms, improve quality of life, decrease health care utilization, and increase communication regarding care planning in serious illnesses such as HF.9–13 Integrating PC enhances traditional HF management by addressing psychosocial, emotional, and spiritual needs, care coordination, and family involvement in care.9,14 PC is categorized as primary PC, specialty PC, or a collaborative approach between primary and specialty providers. Primary PC is provided by all health care professionals without a PC specialty certification while specialty PC is provided by a certified or specially trained provider. 15 A collaborative approach involves providers with specialty certifications collaborating with other providers, such as cardiologists or HF nurses.
Although PC is known to improve outcomes, HF patients rarely receive PC or it is integrated late in the disease trajectory.3,16–18 Common reasons for late referral are due to the unpredictable nature of HF, stigma about end-of-life care conversations and misunderstandings of the benefits of PC by providers, patients, and family members.3,19 In addition, PC is mainly provided in the inpatient setting 4,20,21 even though patients spend the majority of their life in outpatient and community settings. Due to the chronic and unpredictable nature of HF, early integration of PC in settings outside of the hospital is essential, however, few hospital systems can accommodate this need and limit the use of PC to hospice referral.4,21,22 Little is known about PC of HF patients in the outpatient setting such as in ambulatory clinics or the home. Therefore, this integrative review will synthesize the evidence to identify: (1) the current landscape of outpatient PC in HF, (2) the impact of outpatient PC on HF patient outcomes, and (3) key-stakeholders' perspectives of outpatient PC in HF. The framework of the eight domains of PC delineated by the 2018 National Coalition of Hospice and Palliative Care guidelines 9 was used to identify the components of PC that have been used in outpatient PC for patients with HF.
Methods
Framework
Through in-depth interviews with patients and families, the National Coalition for Hospice and Palliative Care developed an eight domain framework (Fig. 1) to shape the Clinical Practice Guidelines for Quality Palliative Care. 9 This framework describes core concepts, structures, and processes necessary for quality PC. By using this framework to synthesize the literature, we can examine the extent to which the eight domains are being addressed in current PC research.
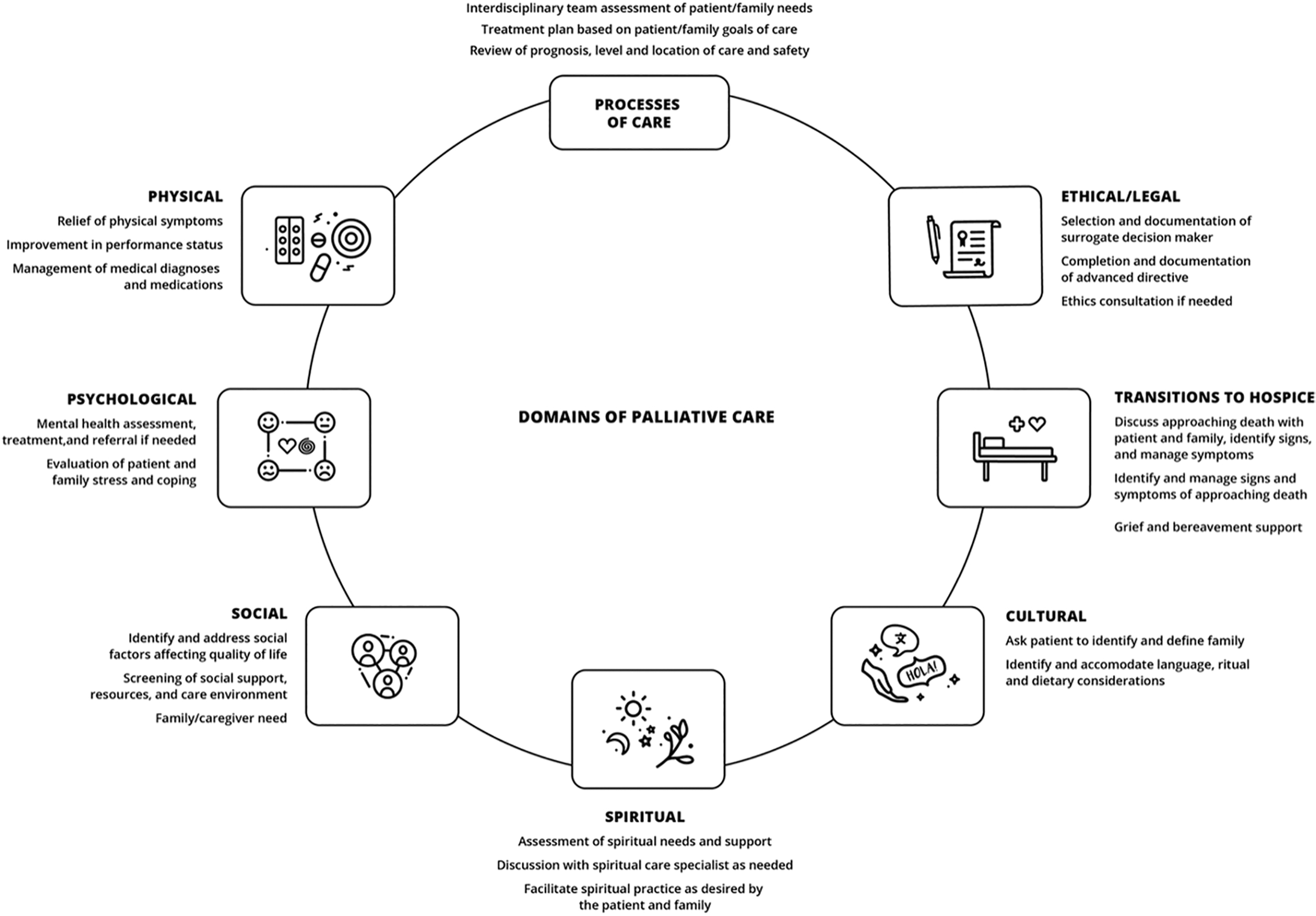
Domains of palliative care.
Search strategy
Following consultation with a library scientist we developed a search strategy and finalized search terms. PubMed, Embase, CINAHL, Cochrane, and Web of Science were searched from the database's inception to February 2019 using medical subject headings, indexed terms, key words, and free text to capture articles related to PC in the outpatient setting for patients with HF. We focused on main search terms of “heart failure,” “palliative care,” “palliative medicine,” “palliative therapy,” “outpatient,” “ambulatory,” “community-based,” “home-based,” and “primary health care.” Table 1 provides the PubMed search strategy used to demonstrate Boolean/Phrase and limits used. When applicable, the PRISMA guidelines and recommendations for integrative reviews were used to guide and write this review.23,24
Search Strategy
Inclusion and exclusion criteria
Studies were selected based upon inclusion and exclusion criteria determined a priori (Table 2). Including qualitative, quantitative, and mixed methods designs provided an opportunity to synthesize diverse perspectives and enhance our understanding of the state of outpatient PC for adults with HF. Studies which focused on providers, caregivers, or patients were included to allow for a holistic perspective. Articles were excluded if they included other diseases without separate results for HF. PC interventions in inpatient setting or skilled nursing facilities were also excluded. In addition, articles which only focused on hospice or advanced directives were excluded. Abstracts, dissertations, case studies, and non-English articles were excluded.
Inclusion/Exclusion Criteria
HF, heart failure; SW, social worker.
Data extraction
The initial search returned 1543 articles. After removing duplicates, a single reviewer screened 1083 articles based on title and abstract using the defined inclusion and exclusion criteria (Table 2). Following title and abstract screening, 70 articles were included in a full-text review and 19 total articles were selected for data extraction by two reviewers (Fig. 2). Data were extracted in a table from all studies regarding study characteristics, providers involved in the intervention or service, location of the study, and key outcomes or themes. Additional data regarding study limitations and demographics of participants are incorporated in the results.
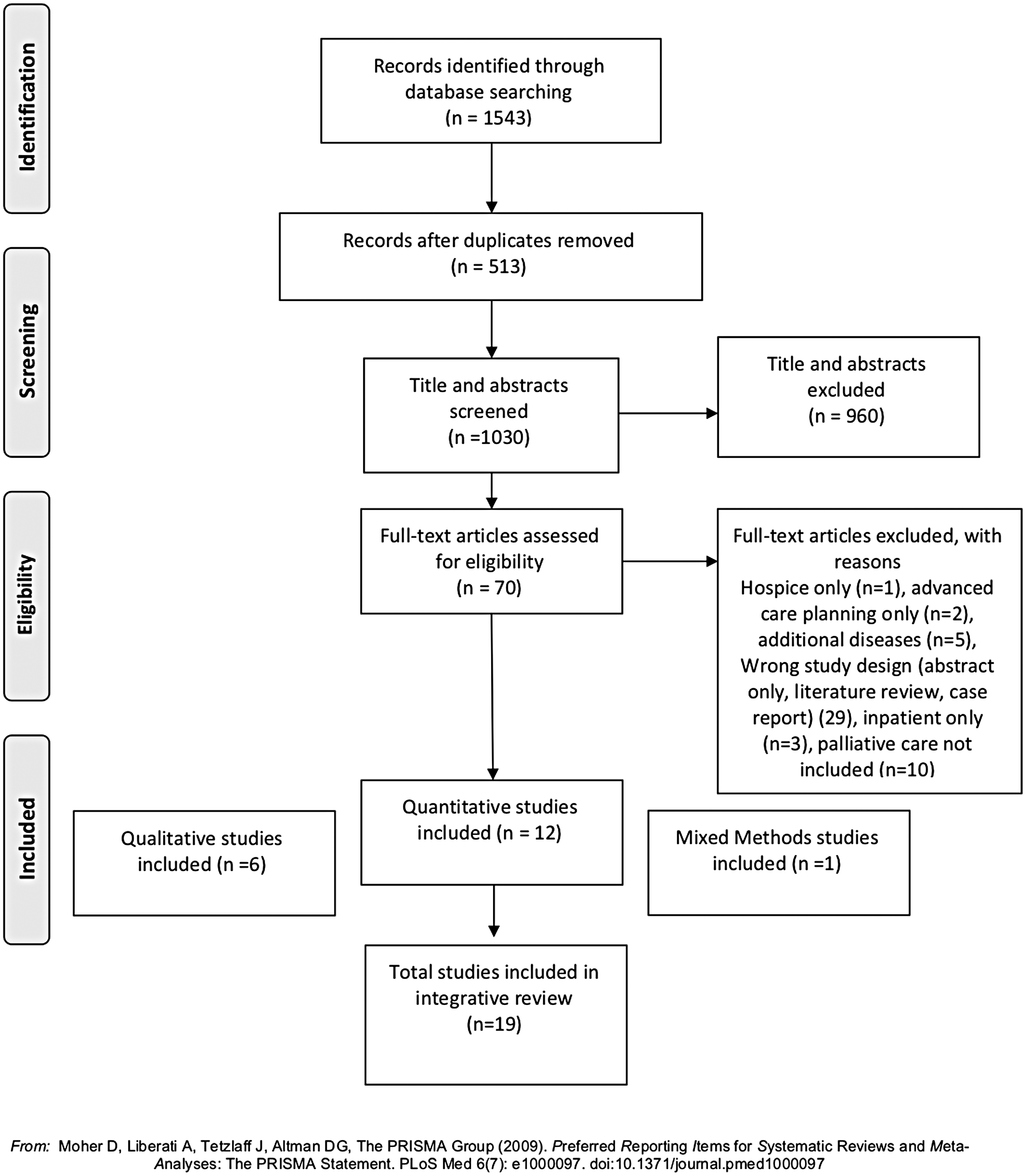
Prisma diagram.
Using the conceptual framework detailed above, each study was assessed for the presence of the eight domains of PC through careful appraisal, multiple readings, and key word searching. The studies were classified as primary PC, specialty PC, or a collaborative model of primary and specialty PC based upon the description of the PC service or intervention.
Each article was appraised for evidence level and quality using the Johns Hopkins Nursing Evidence-Based Practice Appraisal tools. 25 Each study was given an evidence level between I and V and an evidence quality grade of either A, B, or C. Evidence level grades were assigned to each article of either high quality (A), good quality (B), or low quality (C) based on the consistency of findings, generalizability of results, adequacy of sample size, presence of a control group (if applicable), and whether definitive conclusions could be drawn from the data presented.
Results
Among all the studies (19), the majority discussed the delivery of PC (16), while others qualitatively explored provider, patient, and/or caregiver attitudes and knowledge of PC (3). Table 3 provides a summary of study characteristics and key findings. There were 12 quantitative studies, 6 qualitative studies, and 1 mixed methods study. Of the 12 quantitative studies, 6 studies were randomized controlled trials. Most studies (10) were conducted in the United States but other global perspectives were from Sweden (6) and China (3). The average sample size for quantitative studies was 89 participants (range 29–314) and 12 participants for qualitative studies (range 2–36). Of studies that reported age of HF patients (10), the average age (weighted by sample size) was 73.8 years. Thirteen studies reported New York Heart Association (NYHA) functional class, including a large percentage (74.1%) of study participants with advanced HF (NYHA class 3 or 4).
Summary of Synthesized Studies and Key Findings
HF, heart failure; MM, mixed methods; NP, nurse practitioner; OT, occupational therapy; PC, palliative care; PT, physical therapy; RCT, randomized control trial; RN, registered nurse; SW, social worker; Qual, qualitative
Among included studies, the majority were of good (12) or high (6) quality based on the Johns Hopkins Nursing Appraisal Tool. Only one study was the lowest quality of grade C (Table 4).
Quality Appraisal of Included Articles
Current landscape of outpatient PC
Location and type of outpatient PC
Among studies describing a PC service or intervention (16), the majority of PC interventions or services took place in the home (7) or a PC specialty clinic (4). Only one study described integration of PC services in a HF clinic or cardiology practice. Three studies included multiple locations of PC delivery.
Primary PC, delivered by a provider without specialty PC training, was only described by one study. Specialist PC was the most common type of PC described in the studies (12). Several studies (3) utilized a collaborative model of primary and specialty PC. In these studies, the specialty PC provider was responsible for the majority of care and shared details with the HF team through informal discussions, documentation in the electronic health record, or regular interdisciplinary meetings.
Domains of PC addressed
Using the framework of the eight domains of PC delineated by the Clinical Practice Guidelines for Quality Palliative Care, 9 the most commonly addressed domains in interventions, services, or interview guides were the physical, structural, and psychological domains. Over half of the studies addressed the end of life, social, and spiritual domains. The least commonly addressed domains were the cultural and ethical/legal domains. No studies addressed all eight domains.
A subset of quantitative studies (12) described PC interventions or services, with most focused on physical symptom assessment and management (11). Psychosocial assessment or management was described by seven studies and care coordination was described by eight studies. Goals of care or treatment preference discussions were components of seven studies and conversations regarding end-of-life preferences or advanced directive documentation were included in six studies. Few studies (3) included spiritual or existential care and no studies mentioned cultural considerations of care.
Impact of outpatient PC on patient outcomes
Outcome measures of quantitative studies
Of the 12 quantitative studies, the most common outcome measure was the Edmonton Symptom Assessment System (ESAS), a validated measure of the patient's perception of physical symptom severity. Few studies (2) measured other physical outcomes such as functional status. Half of quantitative studies used a quality-of-life measure, including the McGill Quality-of-Life questionnaire (2) and Kansas City Cardiomyopathy Questionnaire (2). Few studies (4) measured psychological outcomes, such as depression or anxiety. Two studies reported documentation of an advanced directive or advanced care planning conversation. It is important to note that the quality-of-life measures often include multidimensional assessments of wellbeing, which may include psychological, social, spiritual, and physical wellbeing.
Quantitative findings of randomized controlled trials
Among the randomized controlled trials (6), five focused on patient-reported outcomes and reported statistically significant improvement in symptoms, including depression, anxiety, shortness of breath, fatigue, and overall symptom burden. Among the four studies which measured quality of life, all four studies found statistically significant improvement in quality of life following PC interventions. The sixth RCT, by O'Donnell et al. (2018), 51 focused on provider documentation of advanced care planning preferences with statistically significant increases in provider documentation after a social worker-led intervention focused on increases in frequency of advanced care planning discussions between patients and providers
All studies, which measured hospital readmission rates (3), found statistically significant reductions in hospitalizations following PC intervention. The interventions described by two of these included a variety of intervention components, including physical, symptom, and psychosocial assessment, social and spiritual needs assessments, and care coordination.26,27 The intervention for the third included fewer components, including symptom assessment, medication management, and HF education. 28
Quantitative findings from non-RCTs
Although outcome measures varied widely among the six quantitative studies, which were not RCTs, physical symptom burden, quality of life, patient activation, and perceived control significantly improved among those receiving PC. One chart review reported significant reduction in all cause and HF hospitalizations following PC. Divergent findings in one chart review showed no statistically significant differences in any outcome measures between the patients with PC consultations and those without.
Key stakeholder perspectives on outpatient PC
Qualitative and mixed methods findings
Qualitative articles included in-depth interviews with HF patients, caregivers, and a variety of providers. A common theme in all qualitative studies was uncertainty, including the unpredictable nature of HF and adapting life to this uncertainty. Patients discussed uncertainty related to the unpredictable changes in their bodies due to HF. However, only two out of the six qualitative studies included caregivers, an essential part of the care team.
One main difference emerged among this group of articles. When discussing HF, providers generally focused on long-term trajectory, whereas patients and caregivers focused on navigating and adapting to everyday life. Providers discussed uncertainty in estimating survival, often leading to ambiguity regarding when to initiate PC and which provider should be responsible for initiation. Providers were also uncomfortable starting discussions about end of life and felt that patients were not always aware their disease was end stage. Patients and caregivers focused on the need for day-to-day adaptation and symptom management. Another study examined knowledge and attitudes toward PC, 29 which showed that none of the patients or caregivers interviewed knew about PC, but the majority of participants suggested that the services of PC should be integrated early on in their HF care.
Limitations of included studies
Women were underrepresented in samples of the studies evaluated. Of the 11 studies which presented baseline demographic characteristics of the patient population, the majority (9) had a lower proportion of women than men in the sample. In addition, samples were not ethnically representative. Of the eight United States studies, which included demographic information regarding race and ethnicity, the majority of the studies had a primarily white sample (7). The international studies did not address ethnicity. Caregivers were included in four studies (4). Finally, all quantitative studies cited small sample size as a limitation, with only one randomized controlled trial stating it was adequately powered. 30
Discussion
Integrated summary of the literature
Taken together, this review illuminates several key findings with important implications for future research and practice. The review of 19 studies highlighted the availability of outpatient PC services in home and PC clinics for patients with HF, however, the nature of most services was specialist PC. Of the eight domains, physical, structural, and psychological are commonly addressed by PC programs/interventions and the ethical/legal and cultural domains were rarely addressed by the studies we identified. The availability of outpatient PC was significantly associated with positive patient outcomes to alleviate physical and psychological symptoms, improve quality of life, and decrease rehospitalizations. Still, there are significant gaps in research and clinical care, which promote availability of primary PC and address the cultural and ethical/legal domains in care of patients with HF in outpatient settings.
Changing the paradigm: Optimizing primary PC
Despite limited access to specialty PC in the outpatient setting, current research predominantly uses specialty PC models rather than primary PC models.31,32 Reliance on specialist models for every HF patient with PC needs may be unrealistic.33–35 Therefore, professional organizations recommend educating all providers in primary PC competencies.9,36 However, education alone is unlikely to change practice patterns. 15 HF providers need feasible, efficient, evidence-based ways to implement primary PC for their patients. 37
HF providers already address the physical domain of PC through excellent, guideline-directed symptom management.17,38–40 This is an essential core competency of HF care and PC. However, no standard of care exists to routinely and systematically assess needs in other domains of PC.3,41 This may contribute to the reality that none of the included studies addressed all domains of PC recommended by the Clinical Practice Guidelines for Quality Palliative Care.
Despite the current recommendation to integrate PC based on patient-reported needs rather than provider-estimated prognosis, the majority of existing PC needs assessment tools rely on provider prognosis rather than patient-reported needs.17,38–40 Future research utilizing patient-reported multidomain needs instruments may promote patient and family-centered needs-based primary PC.42,43
Gaps in the cultural and ethical/legal domains of PC
Although the guidelines from the National Coalition for Hospice and Palliative Care recommend addressing all eight domains in PC interventions or services, 9 none of the studies addressed all domains. As providers are trained to focus primarily on the physical domain, PC integration provides opportunity to promote holistic care through assessment of additional domains.
The cultural domain and the ethical/legal domain of PC were the least addressed, potentially resulting in deficits in these domains of PC for patients and families. Culturally competent care can decrease disparities and improve patient outcomes and quality of care. 44 Furthermore, due to the unpredictable trajectory of HF, advanced care planning can promote autonomy and ensure a surrogate decision maker is identified. By addressing these domains, future PC research and practice can address relevant cultural, ethical, and legal needs of patients and families with HF.
Lack of representativeness
Although HF occurs equally in men and women and is more prevalent among African Americans than Caucasians, 45 participants were primarily Caucasian males with advanced HF. A lack of representativeness of women and ethnic minorities in PC research and practice merits evaluation and action. Current research indicates inequitable access and utilization of PC for ethnic minorities and those of lower socioeconomic status.46,47 Combined with an underrepresentation of the cultural domain of PC, a lack of ethnic representativeness presents a challenge to examining if current PC interventions and services are accessible and appropriate for patients and families from different cultural backgrounds.
This important finding highlights the need to ensure appropriate representation of ethnic minorities, lower socioeconomic status, and women in future samples to promote culturally competent PC. In addition, samples, including participants with earlier stages of HF may reveal additional insight into integrating PC earlier in the disease trajectory.
Strengths and limitations
This review had several limitations. First, our search strategy may not have been comprehensive enough to capture all domains of PC, nor integrated disease management clinics that are not described with a PC focus. Exclusion of articles, which included hospice, may have resulted in inaccurate results in the spiritual, end of life, or ethical/legal domains, as these domains are often addressed in hospice. Also, there was only a single reviewer for article screening and selection, which may have introduced bias.
Despite limitations, this integrative review provides a synthesis of the current evidence specifically focusing on outpatient PC in patients with HF. Strengths of the study include consultation with a library scientist to develop a search strategy, use of inclusion and exclusion criteria determined a priori, and the organization of the literature by domains of PC. Inclusion of quantitative, qualitative, and mixed methods studies provides a more highly integrated understanding of the state of the science and care provision in this population.
Conclusion
The current outpatient PC landscape consists of specialty PC in the home or PC clinic setting, rather than utilizing primary PC or collaborative models. PC services and trials improve quality of life, alleviate physical and psychological symptoms, and decrease rehospitalizations. Significant gaps remain in clinical care and research, which address the cultural and ethical/legal domains of care. These findings highlight a need for future PC research which utilizes a holistic, integrated, team-based approach to addressing all domains of PC in representative samples.
Footnotes
Acknowledgments
The authors are grateful to Stella Seal, MLS for her guidance in the search strategy and Anushka Jojodia for designing the eight domains of palliative care graphic.
Funding Information
The lead author is a T32 fellow receiving support from the National Institute of Nursing Research (5T32NR012704-09).
Author Disclosure Statement
No competing financial interests exist.