
Abstract
Abstract
Background:
Traumatic events are sudden, unexpected, and often devastating. The delivery of difficult news to patients and families in the trauma setting has unique challenges that necessitate communication skills that may differ from those used in other clinical environments.
Objective:
Design and implement a novel curriculum to teach, assess, and provide feedback to trauma residents on the communication skills necessary for delivering difficult news to patients and families in the trauma setting.
Methods:
This communication curriculum was delivered in three separate phases: (1) didactics using a video education e-module, (2) simulated practice of trauma resuscitation with a high-fidelity mannequin followed by role play of delivering difficult news, (3) an observed skills assessment using standardized patients (SPs). Each phase focused on delivery of difficult news of death and of uncertain/poor prognosis after a resuscitation in the trauma bay. Learners were trauma residents that included postgraduate year (PGY) 1–2 general surgery residents and PGY 1–4 emergency medicine residents at a level 1 trauma center. Outcomes include resident comfort, knowledge, and confidence in delivering difficult news in the trauma setting.
Results:
Thirty-nine trauma residents participated in the three-phase curriculum. There was an increase in the mean scores of resident-reported comfort, knowledge, and confidence in delivering difficult news for the seriously injured. SPs rated 78% of residents as competent to perform delivery of difficult news in the trauma bay independently.
Conclusions:
A curriculum to teach and assess trauma residents in the skills necessary to deliver difficult news in the trauma setting is both feasible and effective.
Introduction
Delivering difficult news to patients and their families is an essential skill that all physicians must possess. Although holding goals of care conversations with patients and families are part of the core competencies for residents in all specialties, 1 standardized processes, such as use of the Objective Structured Clinical Exam (OSCE) to assess whether the residents have achieved this competency is rare. In specialties such as surgery and emergency medicine (EM) where technical skills are a priority, residency training has historically placed lesser emphasis on teaching the skills of effective communication. Although curricula are increasingly being designed to help teach communication skills to surgery residents, many of these focus on disclosure of medical errors or communicating serious news related to a biopsy or surgery. We have found that a clear gap exists in curricula focused on teaching communication skills that are unique to the trauma setting. 2
Each setting, for example, perioperative versus oncology, inpatient versus outpatient has its own set of challenges to effective communication with patients and families. Similarly, the trauma setting is unique. Trauma is a sudden unexpected often catastrophic event that may affect previously healthy individuals, sometimes drastically impacting a person's ability to function or even resulting in death. This abrupt nature of the event leaves the family unprepared for the news they are about to receive, and they are often in shock or dealing with strong emotions. There is also no pre-established doctor–patient relationship. The rapidly evolving clinical state after the traumatic event, often has the family and patient grappling with a lot of information coming to them in a rather short period of time. Adding to the stress, in many instances, the trauma clinicians have to deliver this news immediately after an all-consuming intense trauma resuscitation when they themselves have had little time to process their own emotions. 3 The skills needed to deliver difficult news in this setting, therefore, include special considerations for effective communication.
Through a review of the literature, we identified a gap in teaching and assessing resident communication skills specifically in the trauma setting. 2 This literature review also established that simulation and OSCE have been very effective as modalities to teach surgery residents and assess these communication skills in other settings. 2 Therefore, with funding from a graduate medical education grant by the Picker Gold Foundation we designed and implemented a novel curriculum to teach, assess, and provide feedback to trauma residents (including both surgery and EM) on the communication skills to hold difficult conversations with the family of seriously injured patients. We also developed a communication tool and a video didactic resource that have been previously published for educators. In this study, we present the outcomes of the entire curriculum on teaching trauma residents the delivery of difficult news of death and uncertain or poor prognosis in seriously injured patients. We hypothesized through this curriculum we would be able to increase resident comfort, knowledge, and confidence in delivering difficult news in the trauma setting.
Methods
Setting
This curriculum was developed and piloted at a major northeast academic health center with a level 1 trauma center. The emergency department provides care to the trauma patients in a collaborative manner with patients who are walk-ins and brought in with basic life support needs primarily getting care from emergency providers, with activation of trauma team for patients with advanced life support needs.
Learners
The EM residency training program is a four-year program with 24 residents and the surgery residency program is a five-year program with 50 residents. The curriculum took place over the course of an academic year and was delivered to trauma (EM and surgery) residents that included general surgery residents (postgraduate year [PGY] 1 and 2) and EM residents (PGY 1–4). All parts of the module were performed during protected education time. Coordination of this block time occurred between the surgery and emergency department to allow the presence of both specialties particularly for the simulated sessions to reflect real practice.
Curriculum
The development of this curriculum was grounded in Kolb's experimental learning theory. This process includes four stages: experience, reflection, conceptualization, and experimentation to solidify learning of skills and concepts. 4 This communication curriculum was delivered in three phases in order “to touch” all stages of Kolb's learning theory: (1) didactics, (2) simulated practice and role play, and (3) OSCE assessment. Each phase focused on both delivery of difficult news of death and of uncertain/poor prognosis in seriously injured patients after a resuscitation in the trauma bay. We also evaluated the effectiveness of each phase as follows.
1. Didactics: Video Education E-Module in Flipped Classroom Format
The authors developed a case-based online video on how to deliver difficult news after resuscitation in trauma. Residents were assigned to view this 30-minute video asynchronously over a two-week period. Residents also received a study guide for difficult conversations after trauma and a pocket card. The video, study guide, and pocket guide introduced residents to the ABCDE framework. This framework was developed by the authors based on a review of the literature, best practices, and solicited feedback from other educators at national conferences, and finally families of patients that had experienced traumatic death. The ABCDE framework was specifically developed for initiating difficult conversations in the trauma setting as it is a familiar framework for advanced trauma and cardiac life support algorithms. The Pocket card and breakdown of the framework can be seen in Figure 1. After completion of the online module, time was set aside during education time to debrief about key aspects of the module. A detailed outline and the materials for this e-learning video module have been published previously. 5
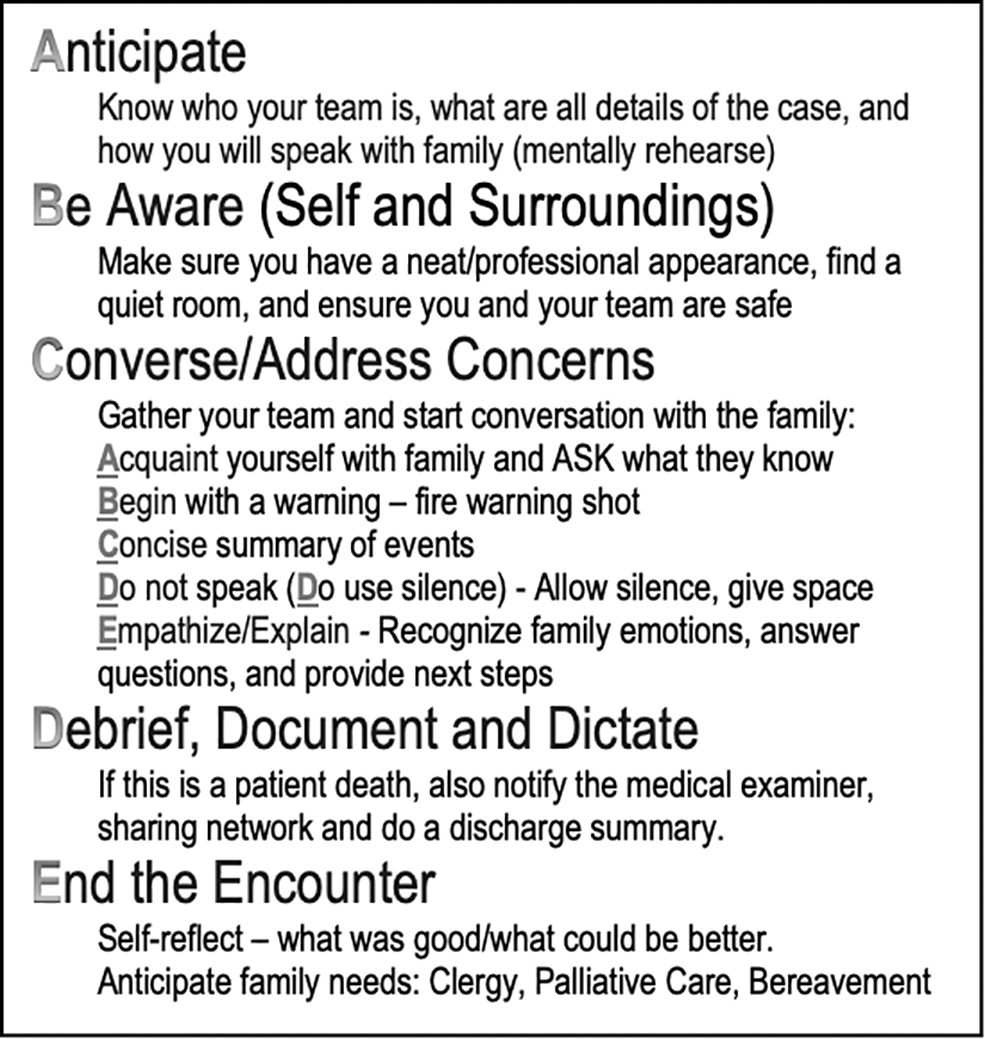
ABCDEs: Trauma communication.
Assessment of the didactic phase
A preassessment consisted of two components, a self-reflection on previous trauma resuscitations and a self-assessment on perceived knowledge, comfort, and confidence in holding difficult conversations in the trauma setting. These components were designed to assess the learners' previous experiences, allow them to reflect on these experiences while establishing the importance of the topic.
The postassessment consisted of two components. The first part was an assessment of the knowledge delivered in the curriculum. It included questions about the steps of breaking bad news as well as common patient reactions and strategies to handle these reactions. The second part was a survey on perceived knowledge, value of self-reflection, and value of the educational experience.
2. Skills practice: Hybrid simulated resuscitation of a high-fidelity mannequin combined with role play of delivering difficult news
This session consisted of two resuscitation scenarios, one resulting in a traumatic death and the other a patient with a poor and uncertain prognosis. Participants were divided into two teams consisting of four to five residents per team; each team had an opportunity to perform one of the scenarios and observe one of the scenarios. The simulation progressed with a case scenario followed by resuscitation of the high-fidelity mannequin that was immediately followed with role play of delivering the news of the resuscitation to the family. Role play was conducted by asking for resident volunteers from the team that performed the resuscitation to play the role of physician and two family members.
Assessment
Participants completed a postassessment on team performance by assessing team behavior domains and a survey on the simulated training environment. Team behavior domains included both self-assessment of team and peer-observer assessment of team. Based on prior literature and scales used in simulation, the team behavior domains included use of support, global awareness, communication, role clarity, and resource utilization. These were assessed using a Likert-like scale ranging from 1 = detrimental to 7 = outstanding. For assessment of the training environment a Likert-like scale (1 = strongly disagree to 4 = strongly agree) was used to ask participants to rate statements on the training environment, simulation/equipment, instructors, and the overall experience.
3. Observed skills assessment: Teaching Objective Structured Clinical Examination
The Teaching Objective Structured Clinical Examination (TOSCE) format was used to observe, assess communication skills, and provide formative feedback. A detailed description of this curriculum, including the case prompts has been previously published. 6 In brief, residents participated in one of two cases that involved delivering difficult news of traumatic death to a family member of a trauma victim or delivering difficult news of poor prognosis. Family members of trauma victims were portrayed by trained standardized patients (SPs). Faculty facilitators and peer observers observed the full interaction of communication between SP and resident. After each scenario, a debriefing session provided formative feedback to the resident.
Assessment
Participants were assessed by the SP and performed self-assessment on their communication skills and demeanor during the TOSCE. Assessment was performed using a checklist and a Likert-like scale from 0 to 3 (0 = unsatisfactory or poorly done to 3 = excellent).
After completion of the entire curriculum, residents completed a postassessment on their comfort, knowledge, and confidence in delivering difficult news in the trauma bay.
This study was reviewed and approved by the Institutional Review Board.
Statistical analysis
Means and standard deviations are reported for continuous variables and counts or percentages for categorical variables. Pre- and post-intervention data analyzed as unpaired Wilcoxon rank sum test. A p-value of <0.05 was considered to be statistically significant.
Results
Overall 39 trauma residents participated in this curriculum. Residents reported that each section of the curriculum was valuable (84% video education e-module, 89% hybrid simulation session, and 92% TOSCE). After the completion of the curriculum there was an increase in the mean scores of resident-reported comfort, knowledge, and confidence in delivering difficult news of death and poor prognosis (Table 1). The percentage of residents that responded “agree” or “strongly agree” that they were comfortable, knowledgeable, and confident increased in both delivering news of poor prognosis and of death. In delivery of difficult news regarding poor prognosis, the percentage of residents reporting agreement with the comfort statement increased from 82% to 93%, knowledge increased from 85% to 96% and confidence increased from 84% to 89%. In the delivery of difficult news regarding death the percentage of residents agreeing with statement regarding comfort increased from 79% to 93%, knowledge increased from 82% to 97% and confidence increased from 82% to 85%.
Pre–Post Learner Response for Entire Curriculum
Statistically significant.
SD, standard deviation.
Video Education E-Module
Thirty-four residents completed the presurvey for the video education e-module and 28 completed the postsurvey. After the module, there was a trend toward improved resident perception of their knowledge in both delivering difficult news and notification of death in the trauma setting. There was a significant increase in the percentage of residents that valued written self-reflection after the module (Table 2`).
Pre–Post Learner Response for Video Education E-Module
Statistically significant.
Hybrid simulation session
Thirty-one residents participated in the simulation session. Peer observer rated team performance high across all five team behavior domains. The range of mean scores from peer observers in the two scenarios ranged from 5.33 for awareness to 6.19 for role clarity. Figure 2 shows the mean score of peer assessment of team performance by behavior domains. We also found that the residents performing the simulated session rated themselves higher than peer observers in 9/10 instances (p = 0.01). Self-rated mean scores ranged from 5.75 for awareness to 6.4 for role clarity. After the simulation session residents reported that they felt better prepared (81%), more knowledgeable (77%), and more confident (77%) on the topics covered in the simulation. Eighty-one percent of participants reported feeling more prepared to care for patients presenting with both traumatic arrest and multisystem blunt trauma with uncertain prognosis. Ninety percent of participants reported that they would want more opportunities to learn using simulation and would recommend this teaching tool to others.

Peer assessment of team performance.
Teaching Objective Structured Clinical Examination
As previously reported by Lamba et al., 6 25 residents participated in the TOSCE. After TOSCE, SP rated 78% of the residents as competent to perform delivering difficult news independently, 9% as needing close supervision, and 13% as needing basic instruction. The breakdown of TOSCE communication and behavior mean scores using a Likert-like scale by scenario can be seen in Figure 3. The range of mean rating across domains was 2.15–2.92. The lowest mean rating of 2.15 was for “resident expressed understanding” in the poor prognosis scenario and the highest mean rating was for “resident avoided talking down to family member” in the poor prognosis scenario. Mean ratings show concordance between resident self-rating and SP rating. There was a slight trend for higher rating by SP in all domains except “professional manner” and “expressed empathy” in the death scenario and “professional manner” and “expressed understanding” in the poor prognosis scenario.

Mean teaching objective structured clinical examination ratings of residents by standardized patients by scenario.
Conclusions
We demonstrated that implementing a trauma communication skills curriculum for residents is both feasible and effective. After completion of the curriculum, trauma residents felt better prepared, more knowledgeable, and more confident in delivering difficult news in the trauma setting. Through an observed skills assessment 78% of participants were competent to have these difficult discussions independently.
Literature has demonstrated that communication skills can be taught to learners of all levels. 7 Teaching communication skills has been accomplished in surgical residents mostly through role play or simulation,8,9 yet most published communication curricula are centered around perioperative discussions involving informed consent and medical errors, or delivering difficult news in the inpatient or outpatient surgical settings.10,11 To our knowledge only one other trauma-specific simulation-based curriculum included a communication aspect 12 that included role playing to explain brain death. This is the first comprehensive communication curriculum to both teach and assess skills of delivering difficult news for seriously injured patients specifically in the trauma setting. The three-phase structure of our curriculum worked well, in particular closely tying the role play of delivery of difficult news to the simulated resuscitation closely mirrored real practice and helped provide relevance. The use of dedicated study time with no additional hours was equally important.
Since a literature review before designing the curriculum identified no known communication tools specific to the trauma setting, we developed the ABCDE framework. 3 This framework is very familiar to trauma practitioners who use a similar stepwise mnemonic for the primary survey in advanced trauma resuscitations. This framework also allowed us to be action oriented with active verbs that guide the learner. Effective communication requires the same attention and stepwise approach as the performance of any other technical procedure. This is important because although many other tools are used in different settings such as SPIKES (setting up, perception, invitation, knowledge, emotions, summary) in oncology, 13 these are not behaviorally anchored, and not as congruent with the unique needs of the trauma setting.
The traditional way of learning communication skills was either by trial and error or from role models at the bedside. With duty hour constraints and increasing clinical workloads these opportunities are more limited. Also, the real setting does not allow for practice or the safe space to make errors and receive feedback. Simulation is, therefore, an attractive modality to teach residents surgical skills, 14 trauma skills,15–17 and to assess nontechnical skills of team communication and leadership in clinical scenarios. 18 Simulated practice allowed for teams of residents to work together on a resuscitation and closely linked communication to these technical skills ensuring a high level of engagement. Another important aspect of the curriculum was the observed clinical skills assessment using a TOSCE. Although OSCEs are very commonly used in undergraduate medical education 19 to assess competency, their use in graduate medical education is sparse and feedback on communication skills is rarely provided. Using the simulation and TOSCE residents were not only able to both practice their skills, receive formative feedback, but also be assessed on competency.
It is important to note that our academic medical center has some unique resources that allowed for the success of this curriculum. The Picker Gold Foundation grant funding allowed us the funds to train and use SPs. This was a close collaboration between both EM and surgery residency programs with high-level support from both departments. We also had faculty facilitators (3) who were dual certified in hospice and palliative medicine along with their primary expertise in surgery and/or EM. This allowed for an ease of debriefing and for providing feedback to the residents on both their technical skills during resuscitation and communication skills. This level of expertise in both the clinical skills of trauma and communication skills may not be available at other institutions. If that is the case, we would recommend a defined process to briefly develop faculty such as a review of the didactic video, and case scenarios or flow of case assess ahead of teaching sessions. Although many programs and institutions have access to a Clinical Skills Center, this curriculum can also be provided using the ED setting itself. For example, we have used a low-fidelity mannequin in the lesser used pediatric resuscitation room to run the case scenarios and found anecdotally that participants actually find it more “realistic.”
There were several limitations to our study. Owing to the relatively small number of residents in each specialty that participated and the different training levels (PGY 1–2 from surgery and PGY 1–4 from EM) we were unable to make meaningful comparisons within the learner levels or within the two specialties. The SPs we trained and used in the curriculum, routinely interact with medical students, not residents. During the debriefing, SP commented on resident's casual attire and may have rated them lower on professionalism since medical students are usually expected to dress up for their interactions with SP. SP also perceived some residents who expressed knowledge with confidence as somewhat arrogant since they were not used to this level of expertise within their student learners. Attending physicians who were also present during the TOSCEs, however, believed that resident confidence was appropriate to their level of training. In the future we plan to address this important issue to better prepare the SP. As listed earlier, the tools, resources, and curricula developed are generalizable; however, the level of faculty expertise and resources may vary across programs. Finally, we have demonstrated competence in a simulated setting and self-reported increase in knowledge, comfort, and confidence in delivering difficult news. How this translates into real practice with families of trauma victims and when and how these skills should be reinforced due to decay over time is yet to be determined.
In conclusion, a curriculum to teach and assess trauma residents in the skills necessary to deliver difficult news of death and poor prognosis in the trauma bay is both feasible and effective. Through this curriculum, residents are able to improve their knowledge, confidence, and comfort with difficult conversations in trauma so that they may effectively have these conversations with their patients and families. This curriculum may be easily adapted by other residency programs to train trauma residents in these important skills.
Footnotes
Funding Information
Funding for this project was from a graduate medical education grant by the Picker Gold Foundation (Grant Number CH-13-003).
Author Disclosure Statement
No competing financial interests exist.