
Abstract
Background:
Although access to advance care planning (ACP), palliative care, and hospice has increased, public attitudes may still be barriers to their optimal use.
Purpose:
To synthesize empirical research from disparate sources that describes public perceptions of ACP, palliative care, and hospice in ways that could inform public messaging.
Data Sources:
Searches of PubMed and other databases were made from January 2011 to January 2020.
Study Selection:
Studies reporting survey or interview data with the public that asked specifically about awareness and attitudes toward ACP, palliative care, or hospice were included.
Data Extraction and Synthesis:
Two reviewers independently screened citations, read full texts, and performed data abstraction. Twelve studies met inclusion criteria and included >9800 participants. For ACP, 80% to 90% of participants reported awareness, and a similar proportion considered it important, but only 10% to 41% reported having named a proxy or completed a written document. For palliative care, 66% to 71% of participants reported no awareness of palliative care, and those who reported awareness often conflated it with end-of-life care. However, after being prompted with a tested definition, 95% rated palliative care favorably. For hospice, 86% of participants reported awareness and 70% to 91% rated it favorably, although 37% held significant misconceptions.
Limitations:
A limited number of studies met inclusion criteria, and some were published in nonpeer reviewed sources. The studies reflect public perceptions pre-COVID-19.
Conclusion:
Consumer perceptions of ACP, palliative care, and hospice each have a distinct profile of awareness, perceptions of importance, and reports of action taking, and these profiles represent three different challenges for public messaging.
Introduction
Over the past 20
Public messaging is part of a proven approach to changing health behaviors at the population level. A 2015 National Academy of Sciences workshop outlined four guiding principles for health communication initiatives: (1) identify the targeted behavior, (2) develop an effective strategy for exposing people to the message, (3) take a comprehensive multichannel media approach, and (4) express the message in repeated consistent presentations. 11 A single message may be expressed in a variety of formats, taglines, headlines, and sound bites. Successful models for population-based messaging approaches can be seen in campaigns to change public attitudes and health behaviors such as smoking cessation 12 and HIV awareness. 13 Those successful campaigns were grounded in empirical research, developed by messaging experts, tested with their specific public target audiences, and used in a coordinated and consistent way that sets the stage for more extensive conversations between clinicians and patients.
For serious illness care, public messaging that introduces ACP, palliative care, and hospice could increase demand for these services and lead to increased access and quality. But to create large scale culture change, messaging needs to work at the public level. The most effective messaging speaks of the needs of the audience who will need these services in the future—not to patients already familiar with these topics. To put it bluntly, improving public engagement with ACP, palliative care, and hospice needs to address existing perceptions held by the lay public (which in this review are referred to as the “public”) rather than the convictions and beliefs of patients who have already experienced the benefits of these services or dedicated clinicians who work with those patients. In addition, public messaging that introduces these services to the public should differ from the skilled communication that clinicians perform at the bedside of patients with a serious illness.
To inform future messaging to create more public engagement in ACP, palliative care, and hospice, we sought to analyze the empirical public research conducted on these services over the past decade. Our initial searches in medical databases, conducted in July 2019, suggested that the evidence base was too small to justify a systematic review. 14 We felt that a more useful approach would be to describe the existing body of evidence in a way that could inform future research. 15 Thus, we conducted a scoping review to synthesize data from disparate sources, including data not published in medical literature, to address a broad question, and address gaps in the literature. The question we chose for this scoping review was, “What evidence exists to describe how members of the public perceive ACP, palliative care, and hospice in ways that could inform public messaging that introduces the public to these services?” We completed this review in January 2020, before the full extent of the COVID-19 pandemic was widely appreciated.
Methods
Data sources and searches
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines 16 and the scoping review methods manual developed by the Joanna Briggs Institute. 17 We searched the following databases: PubMed, Communication & Mass Media Complete, Rasmussen, and iPoll. The search strategy was designed to capture citations and reports from the search terms (hospice OR palliative OR advance care) and (public awareness OR social marketing OR public opinion) from the time period January 2011 through January 2020. All searches and selection of search terms were performed by an experienced research librarian (N.S.D.). In addition, we sought unindexed reports known to experts in the field.
Study selection
We included studies that reported U.S. public perceptions about ACP, palliative care, or hospice. We excluded studies that asked patients with a serious illness to describe, report, or rate their communication with clinicians or indicate their attitudes toward ACP, palliative care, or hospice, because our objective was to synthesize evidence that could inform messaging that introduces the lay public to these services. Two investigators reviewed all search results, read all candidate reports, and agreed on the final selection of included studies (Fig. 1).
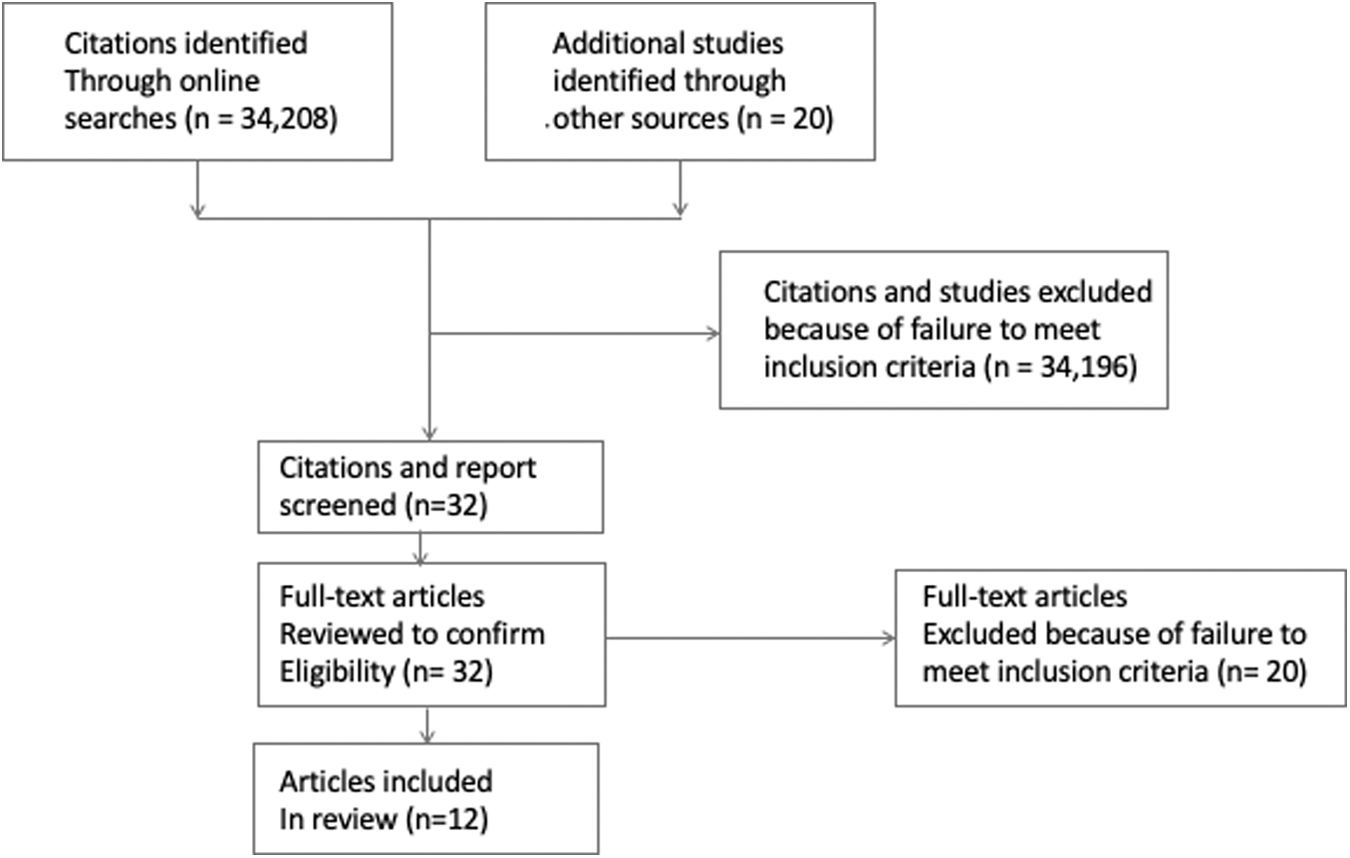
Study selection.
Data extraction
We designed a data charting form that two investigators (M.S.G. and A.L.B.) populated, iterated, and updated. Extracted variables included date of report, study methodology, population characteristics, and key outcomes. We did not confirm abstracted data with authors of the individual studies.
Data synthesis
We grouped study data by ACP, palliative care, or hospice because our early analyses indicated that the public has distinct views about each of these services.
Role of funding sources
The funding sources were not involved in the development of the research question, selection of search strategies, data extraction or analysis, or reporting of results.
Results
Our initial searches resulted in 34,208 citations of which 32 met our criteria to be screened and 12 met criteria for inclusion. The selection process is depicted in Figure 1, and the 12 included studies are summarized in Table 1.
Overview of 12 Studies That Met Inclusion Criteria
ACP, advance care planning; EOL, end-of-life; PC, palliative care.
Study methodologies and publication
The 12 studies spanned a variety of methodologies: 1 systematic review that addressed public perceptions, cross-sectional surveys, and surveys that also included focus groups. Of these 12 studies, 7 were published in peer-reviewed journals, and 5 were published as public reports by their funding organizations.
Study populations and settings
Most included studies involved a population of adults, mostly older with age >60 years, outside of health care settings. The total number of participants involved in studies of ACP, with the exclusion of the systematic review, was >3800. The number of participants in each ACP study ranged from 346 to 2500. The total number of participants involved in studies of palliative care was >5000, and ranged from 350 to 3504 per study. The total number of participants involved in studies of hospice was >1100, and ranged from 148 to 800 per study (Table 1).
Measurements and outcomes
The most common measurements involved awareness of a particular aspect of serious illness care, ratings of importance or favorability, participant misconceptions, and self-reports of direct engagement. The measurements included in these studies were heterogeneous, limiting comparisons that could be made across studies and topics. See Table 2 for key reported elements.
Comparison of Public Perception Findings by Type of Serious Illness Care
Having a health care agent/proxy, or documents, or enrolling in programs.
These data were not from an included study but represent Medicare data 39 and are included for comparison.
NA, not applicable.
Perceptions of ACP
Four studies examining public awareness and perceptions about ACP show that a large majority (80–90%) of people are aware of ACP (described in two surveys as “end-of-life planning”),18,19 and a similar proportion (80–90%) think it is important.18,19 However, taking action is a different matter. A large body of evidence shows that only a minority of the public report having named a health care proxy decision maker (10–41%) or completing a written directive (23–32%). 20
The gap between high awareness and low action taking for ACP is best explained in a 2019 survey that also involved 150 participants recruited into an online community. 21 That study found five different subgroups of consumers based on their attitudes toward ACP. Two of these segments, representing a combined 34% of the participants, had taken action in ACP, and their reasons for doing so included past experiences—often negative instances of being asked to make decisions for a family member who had not left any indication of their wishes for end-of-life care. The remaining segments, representing a combined 66% of the participants, had not taken action and did not wish to, and their reasons for declining to act included mistrust of the health system that their wishes would be followed, confidence that those who mattered to them already knew what they wanted, and inability to act because of other life stresses. 21
Perceptions of palliative care
Six studies examining public awareness about palliative care were included (three of which were different analyses of the same dataset conducted by different investigators),22–24 and all demonstrate that the public are unfamiliar with palliative care. Over 70% of participants could not even rate palliative care for favorability.25,26 In addition, the small proportion of participants who felt familiar with palliative care held perceptions that were mostly inaccurate. For example, 59% of those who said they were familiar with palliative care thought it was the same as hospice or end-of-life care. 26 However, in two studies, when participants received a definition of palliative care that emphasized the benefits and appropriateness at any stage of illness, virtually all (95%) rated it favorably.25,26
Perceptions of hospice
Public awareness of hospice is high, at 83% to 85%,27,28 and public favorability is also high, at 71% to 90%.27,28 Hospice awareness and favorability are higher among participants with more education or personal experience. 29 However, a significant minority of participants, 37%, had misconceptions about hospice, including beliefs that choosing hospice was tantamount to “giving up.” 28
Factors influencing public perceptions
These studies showed consistently that older white females with higher education and socioeconomic status had higher awareness and were more inclined to take action for ACP and hospice.18,19,21–24,28 Personal experience with a family member that was positive, trust in the health system, presence of a strong relationship with a primary care or other clinician also correlated with higher awareness.18,19,21,28
For other ethnic and socioeconomic groups, lower awareness and action taking were correlated with barriers about discussing serious illness, distrust of documents, and mistrust in the health care system. 30 Political party affiliation did not influence views of palliative care or hospice in the one study that included that information. 26
Gaps in existing research
There were no studies addressing awareness or perceptions of specific ethnic or cultural groups, and no studies with a target population of the uninsured. Although we excluded studies of patients with serious illness, the level of participant experience with prior serious illness care or caregiving was not reported.
Discussion
The purpose of this scoping review, conducted well before COVID-19 was declared a pandemic, was to synthesize evidence that addressed the question: “What evidence exists to describe how members of the public perceive ACP, palliative care, or hospice in ways that could inform public messaging that introduces the public to these services?” The 12 studies that met our inclusion criteria included >9800 participants, mostly >60 years of age, outside of health care settings. Taken together these studies indicate that public perceptions of ACP, palliative care, and hospice each have a distinct profile of awareness, perceptions of importance, and reports of action taking. For ACP, 80% to 90% of participants report awareness of the need for end-of-life planning, and a similar proportion consider it important, but only 10% to 41% report having named a proxy or completed a written document.18,19 For palliative care, 66% to 71% of participants reported no awareness, and those who reported awareness of palliative care often conflated it with end-of-life care.23,24,31 For hospice, >80% of participants reported awareness and 70% to 91% rated it favorably, although a minority had serious reservations.
What does all this mean? Our pre-COVID-19 interpretation was that these distinct profiles indicate that ACP, palliative care, and hospice each face their own messaging challenge. The challenge facing messaging about ACP could be summarized as “high awareness/low action.” Most of the public is aware of ACP, and think it is important, but a minority have taken action. The challenge facing messaging for palliative care is “low awareness/common misconceptions.” Few among the public are aware of palliative care, and of those who are aware, most hold an incorrect view that palliative care is about dying. The challenge facing messaging about hospice is “high awareness/significant reservations.” Most of the public are aware of hospice, but a significant minority have had negative personal experiences with hospice or hold incorrect views about what hospice provides.
What ACP, palliative care, and hospice have in common in these pre-COVID-19 data, however, are that consumer misperceptions, inaccuracies, and conflation of one for the other are almost routine. The public confuses ACP with end-of-life care, palliative care with hospice, and hospice with hastening death. The evidence we reviewed did not characterize how the public feels about confronting death or dying, but a growing body of evidence collected from patients living with a serious illness indicates that a majority are not interested in talking about dying, at least early in their illness.31–34 If the public holds a similar reluctance toward talk about dying, the biggest messaging challenge of all might be for a field that has traditionally promised to provide “a good death” to find new ways to talk to the public. We hasten to add, though, that improving public messaging does not require that clinicians back away from cultivating prognostic awareness or talking about dying in appropriate circumstances. Public messaging has a different purpose than patient–clinician communication.
This scoping review did not evaluate the effect of messaging strategies that could overcome the challenges already described. However, these challenges suggest that one approach may be for individual public campaigns to address a specific population-based goal for ACP or palliative care or hospice—and for public campaigns to treat each service separately rather than trying to show how they overlap or, at times, serve similar functions. For example, a goal for an ACP campaign could be a message that targets concerning consumer assumptions that reduce willingness to take action. Similarly, a goal for a palliative care public campaign could be a message that quality of life is better at any stage of illness if palliative care is accessed. Finally, a goal for a hospice public campaign could stress dependability, trust, and care in the setting best for that patient. (Note that consumer associations of hospice with end of life are so strong that raising death in an introductory public message is unnecessary, and possibly alienating to those reluctant to think about dying.)
We acknowledge that these suggestions about messaging raise questions. For example, a commonly used graphic stresses continuity between palliative care and hospice, and has been useful in defining palliative care. 35 This graphic was designed for clinicians and policy makers, and was never tested for clarity with the public. We also acknowledge that ACP has been defined as supporting adults “at any age or stage of health.” 36 The international consensus process that produced this definition was not designed for public messaging. Finally, variability in service availability and eligibility criteria across the United States may affect people's perception of these services, which even effective messaging cannot overcome. These issues do not, however, preclude innovation in public messaging. Successful public campaigns point toward a single behavior, and they do not attempt to fill in all the details.
The evidence base that we were able to assemble for this scoping review was limited, so some caution should be given to this analysis. A little more than a third of this evidence was not published in the medical literature and was not peer reviewed. The cross-sectional surveys involved telephone interviewing, which can introduce biases. The evidence describing differences by ethnic, socioeconomic, or generational factors is limited. Finally, the effect of the COVID-19 pandemic may well change public perceptions in ways that cannot yet be measured.
Nonetheless, these findings provide important insights into challenges in the pre-COVID-19 era to effective messaging and public campaigns for ACP, palliative care, and hospice. Particularly notable are the two studies on public awareness about palliative care done eight years apart that demonstrate no improvement whatsoever in public awareness about palliative care, even as inpatient palliative care penetration into U.S. hospitals was steadily increasing.2,25,26
In the post-COVID-19 era, however, it seems likely that public perceptions of ACP, palliative care, and hospice will all change because of widespread media coverage of medical care during the pandemic, widespread grief and trauma, and a likely reevaluation of U.S. approaches to public health. COVID-19–related ACP, for example, has been prioritized by many health care systems as part of preparation for crisis standards of care. 37 How the public experiences serious illness care in the age of COVID-19 could shape a whole new set of public perceptions.
In conclusion, this scoping review indicates that pre-COVID-19, ACP, palliative care, and hospice had distinct profiles of public awareness, ratings of importance, and action taking. The results underscore the importance of empirical research that measures public perceptions before the development of public messaging, and suggest that further research may be needed once the COVID-19 pandemic has stabilized.
Footnotes
Funding Information
Supported by The John A. Hartford Foundation and the Cambia Health Foundation.
Author Disclosure Statement
No competing financial interests exist.