
Abstract

Dear Editor:
Background
A number of screening tools are used to measure function in palliative care. Understanding relationships between different measures has implications for clinical assessments and service provision. The Australia-modified Karnofsky Performance Scale (AKPS) 1 and the Resource Utilization Group-Activities of Daily Living (RUG-ADL) 2 are two scales collected routinely by the Australian national Palliative Care Outcomes Collaboration, the world's largest point-of-care symptom and function data collection. 3 The AKPS is an 11-point ordinal interval scale (0–100) that measures a person's performance status as it relates to levels of current activity and needs for support. 1 The RUG-ADL 2 is a four-item ordinal scale, which measures four aspects of physical function—bed mobility, transfers, toileting, and eating. The RUG-ADL tool was developed to measure resource use, which is reflected in its rating system. This study aimed to understand whether the AKPS and RUG-ADL could each aid in the interpretation of the other.
Methods
Design
Ethics approval was sought and received from the Peninsula Health Human Research Ethics Committee (QA/12/PH/12) to conduct a retrospective consecutive cohort clinical audit of community-dwelling palliative care clients admitted to an acute hospital.
Data collection and analysis
One hundred of 128 files met audit inclusion criteria. Data were analyzed in Excel™ (Version 2016; Microsoft Corporation, Seattle, WA).
The first and last AKPS and RUG-ADL scores were taken for analysis. A Pearson's correlation coefficient was calculated for first client encounter on admission and the last recorded measures. A line of best fit as determined for first and last AKPS scores for each RUG-ADL category (bed mobility, toileting, transfers, and eating) was also calculated.
Results
A retrospective audit examined prospectively collected data from 100 consecutive community-dwelling palliative care clients of a community palliative care service admitted to an acute hospital in a five-month period. Mean age of participants was 70.7 years and median age was 73 years (range 16–96). Participants had a range of cancer diagnoses including colorectal (17%) or lung cancers (16%). Ten participants had noncancer life-limiting illnesses.
Strength of relationship or effect size has been defined as larger than typical (≥0.70), large or larger than typical (0.50), medium or typical (0.30), or small or smaller than typical (0.10).4 Pearson's correlation tests revealed large or much larger than typical inverse relationships between AKPS scores and each RUG-ADL category. The Pearson's correlation coefficient and line of best fit for the RUG-ADL and AKPS scores for each activities of daily living domain are represented in Figure 1. This reflects similar patterns for the other three domains of RUG-ADL. The shaded area represents the AKPS score at which completing an RUG-ADL provides no additional information about a person's function.
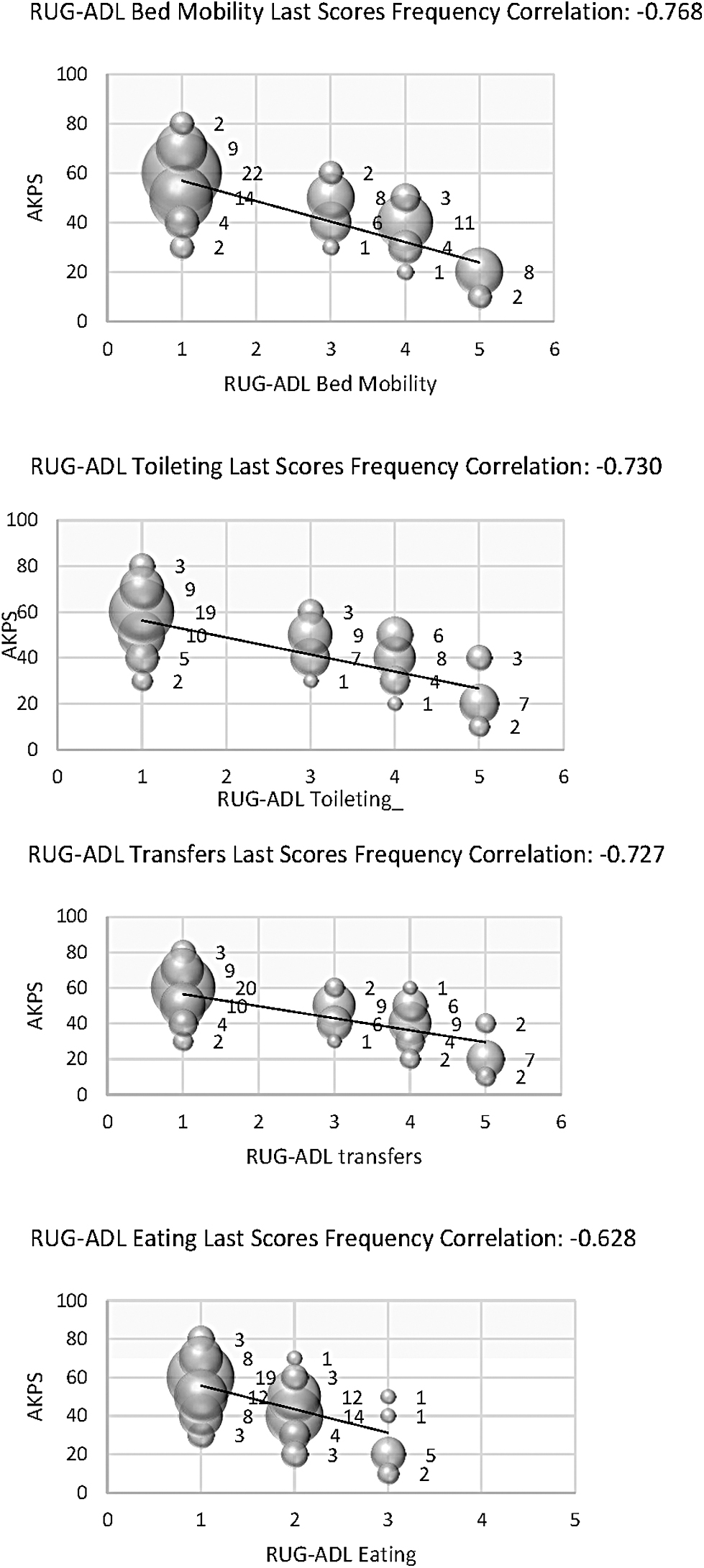
AKPS and RUG-ADL Pearson's correlation coefficient and frequency—last scores. AKPS, Australia-modified Karnofsky Performance Scale; RUG-ADL, Resource Utilization Group-Activities of Daily Living.
Discussion
RUG-ADL adds no information in this cohort when AKPS is >60, and arguably should, therefore, not be routinely measured in these people. RUG-ADL has better discriminatory capacity and provides more functionally useful information the lower the score <60. Given the practical nature of the domains included in RUG-ADL, it is of most value when independence becomes more compromised.